
Abstract
Objectives:
The objective of this study was to investigate the drivers of complementary and alternative medicine (CAM) use in the general population in Australia and to identify key policy implications.
Data and methods:
The National Health Survey 2007/2008, a representative survey of the Australian population, provides information on CAM use (practitioners and products) in the last 12 months. All adult respondents (N=15,779) aged 18 years or older are included in this study. Logistic regression is employed to determine the effect of socio-economic, condition-specific, health behavior variables, and private health insurance status on CAM use.
Results:
In addition to socio-economic variables known to affect CAM use, individuals who have a chronic condition, particularly a mental health condition, are more likely to use CAM. There does not appear to be a correlation between CAM use and more frequent General Practitioner use; however, ancillary private health insurance is correlated with a greater likelihood of CAM use, as expected.
Conclusions:
The Australian government does not currently intervene in the CAM market in a systematic way. CAM is clearly considered to be a legitimate and important component of health care for many Australians, despite the limited availability of clinical evidence for its efficacy and safety. Policy interventions may include the regulation of CAM products, practitioners, and information as well as providing subsidies for cost-effective modalities.
Introduction
However, despite the size of the CAM “market” and the high estimates of prevalence of use, there has been little research undertaken from a policy viewpoint, especially considering the role of government. The Australian government does not currently intervene in the CAM market in the systematic way it does with conventional medicine, despite the perception by many that CAM is a legitimate and important part of primary care.
In economic terms, health “markets” do not operate competitively, generally providing a clear rationale for government intervention. 5 This is because consumers do not have sufficient information upon which to make optimal decisions, and there is a high level of risk and uncertainty in determining the future demand for health care. When considering the CAM market, it is obvious that these key assumptions also do not hold. Although work is ongoing, there is still a perceived lack of clinical evidence upon which to make treatment decisions for CAM, 6 and negative effects from CAM can exist. 7,8 CAM also suffers from the problem of information asymmetry, where consumers are not able to make well-informed decisions on their own. 9 Furthermore, it is well accepted that all individuals face uncertainty with regard to health status and therefore their need for health care, including CAM. The institutional response to uncertainty, in this instance, traditionally includes the consideration of insurance and subsidy schemes to protect the population from catastrophic or unexpected expenditures.
This is similar to the conventional medicine market. It therefore appears justified that consideration of government intervention in the CAM market is warranted. Accepting this logic, policy interventions such as regulation and subsidy might be discussed. However, little still is known about patterns of CAM use at a population level, especially in relation to conventional medicine use.
Many different factors influence the use of CAM products and practitioners. Being female and middle-aged has been positively associated with CAM use4, 10 –14 and has been studied specifically in Australia [15 –17]. CAM use has been shown to vary across cultural groups. 18 –20 Particular chronic conditions have also been positively associated with its use: diabetes, 21 –23 mental health conditions, 24,25 cancer, 26 –28 arthritis, 29 back pain, 30 and hypertension. 31
CAM use is seen by many as an important and legitimate component of health care and self-management of chronic disease. 21,32 There is some evidence to suggest that CAM is more commonly used as a complement to conventional medical care rather than a complete substitute. 11 –13,33 However, some groups may view CAM practitioners as their preferential form of care, for example, Chinese medicine practitioners 34 or naturopaths, 35 or as a substitute for particular health issues. 36 Also, there may be an increased likelihood for certain individuals to be more frequent users of both CAM and conventional medicine. 12
Co-users of CAM and conventional medicine may not always report their CAM use to their general practitioners (GPs), and conversely they may not provide full details of conventional medicine use to CAM practitioners. 11,37 Such behavior is not without risk; there are known interactions between some CAM therapies and conventional medicines; for example, St John's wort (Hypericum perforatum) is known to potentially alter the plasma concentrations of many prescription medicines. 38
The effect of subsidizing CAM use by third-party insurance is also of interest. There are reported associations between having private health insurance and increased CAM use. 1,12 Many private health insurers in Australia already subsidize CAM therapies, and it is likely that ancillary (“extras”) cover would incentivize CAM use if demand was sensitive to price. This is important when considering the possibility of increases in demand, were the government to subsidize CAM in the future.
The objective of this article is to analyze the drivers of CAM use at a population level, paying particular attention to the relationship between CAM and conventional medicine use, the role of chronic illness, and the effect of private health insurance. This is the first analysis to use representative population data from the Australian National Health Survey (NHS) with the aim of informing CAM policy development.
Data and Methods
The National Health Survey (NHS) 2007/2008 randomly sampled households (20,788 individuals) within urban and rural locations across Australia using a multilevel sampling methodology. 39 Sampling fractions for different States were set to account for sparsely populated areas such as the Northern Territory. Household and individual sampling weights were calculated to adjust for the probability of selection. Person and household weights, adjusted for seasonality, were then calibrated against population benchmarks to compensate for over- or underenumeration of particular categories and included in the models presented.
Respondents were asked health-related information regarding long-term medical conditions, health behaviors, their consultations with health professions, and a range of sociodemographic information. This analysis focuses on the responses of all adults, aged 18 years and over, in the sample (15,779).
Variables
The variable of interest is whether an individual chose to use CAM in the previous 12 months. Here, CAM use is represented by separate variables: either visiting a CAM practitioner, or using a CAM product (that is, taking a vitamin, mineral, or herbal supplement regardless of whether it was purchased over the counter or prescribed by a CAM or medical practitioner). For practitioner use, data are available for four types of CAM practitioners only: acupuncturists, naturopaths, chiropractors, and osteopaths. Information on other practitioners has been combined into an “other” category in the NHS due to small numbers and therefore could not be included in this analysis.
The influence on CAM use of a range of sociodemographic variables is considered including age, gender, employment, marital status, and education. Cultural background is represented by whether participants were born in Australia or elsewhere and whether English is the main language spoken at home.
The effect of chronic disease is included in the analysis using self-reported presence of cardiovascular disease, diabetes, cancer, arthritis, osteoporosis, and asthma (a group of chronic illnesses recognized as part of the National Health Priority Area [NHPA]). The experience of a major stress event in the past 12 months is also included. The influence of general health status is measured using a measure of self-reported health and bodily pain; a five-category self reported health variable is collapsed into two categories of either “excellent/very good/good” or “fair/poor,” while bodily pain experienced in the 4 weeks prior to the survey is categorized as “moderate/severe/very severe” or “mild/very mild/none.” The effect of lifestyle factors including smoking, exercise, alcohol intake, and eating patterns is considered, as is health service utilization in the previous 12 months. Finally, the effect of different types of private health insurance coverage was also considered by including dummy variables for individuals who had ancillary (“extras”) coverage alone, ancillary and hospital coverage, or hospital coverage alone.
Models
The effect of these variables on CAM use is considered using four different logistic regression models, where the coefficient reflects the odds of an individual using CAM in the last 12 months. The first analysis includes any CAM practitioner use, irrespective of CAM product (vitamin, mineral, or herb) use; the second model considers product use exclusive of practitioner use; the third includes individuals who used both practitioner and products; and the fourth reports any CAM use. All analyses are undertaken using STATA 10 (StataCorp) and the results are presented as odds ratios with 95% confidence intervals.
Results
Participant characteristics
A summary of the sample characteristics is presented in Table 1. Overall, the prevalence rate for any type of CAM use is around 39% of the adult population. Participants who reported CAM use are more likely to be female, have a post high-school qualification, and report a higher number of chronic conditions. There does appear to be more CAM use with increased income.
p<0.01.
p<0.05.
The age of respondents reporting CAM use broken down by the type of use is shown in Figure 1. The highest proportion of CAM practitioner use is in the 35–39-year age group; however, peak use for vitamins is in the 60–64-year age bracket. Overall, there is a general trend of decreasing use with increasing age.

Complementary and alternative medicine (CAM) use by age category.
A summary of participant characteristics, by type of CAM use (practitioner only, vitamin, mineral and herb use only, and both) is presented in Table 2. As expected, there are differences in correlations between CAM practitioner and product use and different chronic illnesses, likely reflecting the specific treatments available.
Table 3 summarizes key aspects of conventional medicine use by CAM use. CAM users appear to be more likely to use all forms of conventional medicine, including GPs, specialists, and allied health professionals, as well as screening tests compared to non-CAM users. However, as CAM users are also more likely to have a chronic condition, this effect is accounted for, as well as the effect of other sociodemographic variables.
p<0.001.
GP, general practitioner; BP, blood pressure; SD, standard deviation.
Consumer choice of different combinations of primary care is presented in Figure 2. It can be seen that the proportion of participants who choose CAM alone is higher than for GP services alone. However, the combined use of CAM with different conventional medicine services is also relatively high.
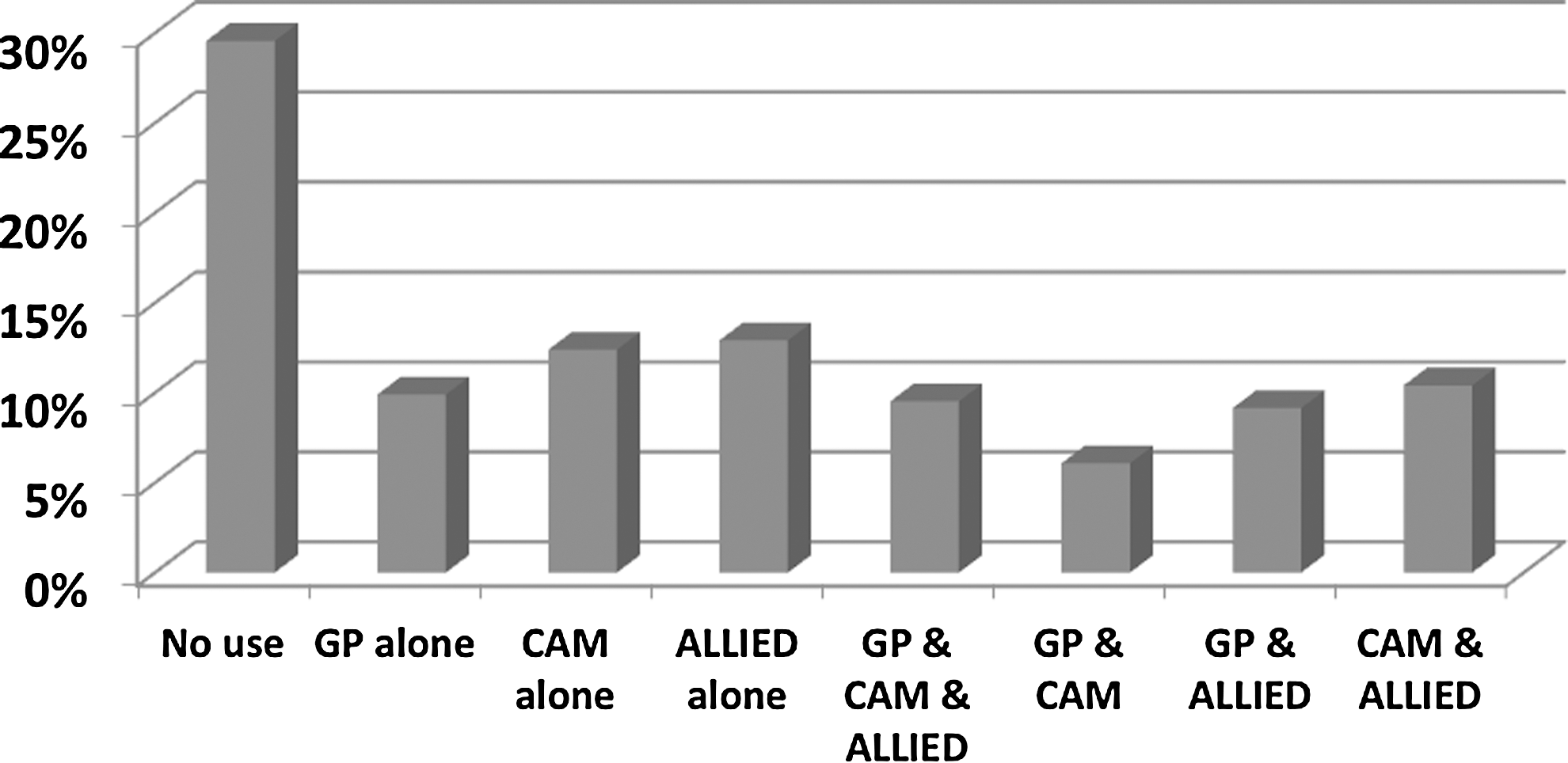
Choice of general practitioner (GP), any complementary and alternative medicine (CAM), and Allied Health Professional use.
Results of the four logistic regression models are presented in Table 4. As shown elsewhere, 4 being female and better educated is associated with a higher likelihood of CAM use, although the association is only found to be statistically significant for users of both products and practitioners. Individuals born in South Asia are less likely to report CAM use, which might be reflective of the restricted definition of CAM in this survey.
p<0.001.
p<0.05.
Bolding indicates statistically significant ORs and corresponding CIs.
CAM, complementary and alternative medicine OR, odds ratio; CI, confidence interval; GP, general practitioner; BP, blood pressure; PHI, private health insurance; SE, Southeast.
In terms of conventional health service utilization, overall it does not appear that CAM users are more likely to use GP or specialist services when controlling for other factors including health status. They do, however, appear more likely to visit allied health practitioners and use a lower number of prescription medicines for chronic illness. Individuals who reported CAM use are generally more likely to report healthy behaviors such as moderate or vigorous exercise, eating fruit, and being a nonsmoker, although this differs between CAM practitioner and product users.
People with ancillary “extras” that private health insurance covers are more likely to use CAM; however, having hospital-only coverage does not affect the probability of use. Being employed is a strong positive predictor of CAM practitioner use, although surprisingly, income shows no effect. * Individuals living in urban areas are less likely to report CAM practitioner use than those living in rural or remote areas. People who reported having one or more NHPA conditions are more likely than others to report CAM use, although patterns of use across different conditions varies. The number of chronic conditions is not statistically significant. The strongest predictor for CAM use is having a mental health condition. Overall, chronic conditions, apart from cardiovascular disease and cancer, are associated with increased CAM use.
Discussion
The results of this nationally representative sample can be used to offer insights about a policy framework for CAM and the rationale for any government intervention in the market. The overall prevalence rate of CAM use of around 40% is lower than those previously reported in Australia; 1,4 however, this is unsurprising given that information on only four types of CAM practitioners (acupuncturists, naturopaths, chiropractors, and osteopaths) is available from the NHS and therefore is likely to be an underestimate. As seen in Figure 3, CAM use may or may not be combined with conventional medicine use and thus may be used as a complement by some groups and as a substitute by other groups.
However, thinking about all CAM use in a single category is rather misleading. As shown by the results of the separate models in Table 4, results are not uniform for people who only use either CAM products or practitioners, or for those who use both (compared to any CAM use). Other authors have argued that a more prescriptive definition of CAM is helpful. 27,40 The current authors propose that each CAM modality be considered in its own right in terms of any policy intervention. Important examples of a more focused approach on specific areas of policy and cost-effectiveness are already emerging in the literature. 41 This not only simplifies the direction of any intervention but also means that existing government mechanisms (such as regulatory and subsidy bodies) can be used as appropriate rather than attempting to set up duplicate mechanisms. Some CAM practitioner boards specific to identifiable groups have already been established (for example, the Chinese Medicine Practitioners Board in the state of Victoria).
In terms of the market not operating “competitively,” there may be justification for government intervention in the CAM market. However, it is important to critically analyze the extent of market failure to determine the merits of any proposed government intervention. Figure 2 shows that at least 26% of the adult population uses some type of CAM and conventional medicine use concurrently. In a recent survey, only 50% of those using CAM spoke with their doctor about their CAM use, 37 meaning that a significant proportion of people in Australia could be at risk of interactions between CAM and conventional medicine use. This reinforces the arguments of others that CAM product and practitioner use should be regulated. 42 –44
Conversely, the positive correlation between CAM use and healthy behaviors provides evidence of the potential gain for improved health and has been shown in other representative populations. 45 Although further research into this association is warranted, at a population level this raises the question of whether certain CAM modalities should be considered for subsidy. What has yet to be investigated is whether CAM use may substitute for more frequent and expensive conventional care, which could be cost saving in certain circumstances. There seems to be little reason why the existing bodies that undertake health care technology assessments cannot be used to make individual modality assessments.
In contrast to previous research, 11,12 there appears to be little evidence of a relationship between CAM use and more frequent GP use; however, CAM users do seem to be more likely to visit allied health professionals. CAM users also seem less likely to be using prescription medications for chronic illness after controlling for health status. Again, this may represent a population subgroup that is better at controlling lifestyle risk factors (possibly through CAM use), although lifestyle factors are included in the model. There is, however, a strong correlation between private health insurance coverage and increased CAM practitioner use (note that products are not currently subsidized by insurers) which does provide evidence of the possibility for over-consumption if CAM was to be subsidized by the government. In this case, mechanisms for controlling the availability of subsidized interventions could be considered, in the same way as for conventional medicine.
There is a strong correlation between CAM use and many of the NHPA chronic conditions. Having a mental health condition greatly increases the likelihood of an individual to use both CAM products and practitioners. The size of the relative risk ratio presented in Table 4 is large and may represent a large proportion of the population “self-treating” mental health conditions, rather than seeking care from their GP. There may also be a comorbidity effect, as people who have chronic conditions are more likely to suffer depression. 46,47 Regardless, the question has to be asked as to why such a large proportion of those with mental health issues are accessing CAM. Underfunding of the conventional system could be one reason, effectiveness of CAM another. This question requires further investigation. Overall, however, the potential gain from subsidizing (proven) cost-effective CAM treatments in this subpopulation is large.
Apart from mental health conditions, other chronic conditions such as arthritis, osteoporosis, and asthma have a strong correlation with CAM use. This is unsurprising as vitamin, mineral, and herbal products are readily available and often specifically marketed for these conditions (e.g., glucosamine for arthritis). When this result is considered alongside other evidence suggesting that most individuals get their information on CAM from family and friends and the Internet, 37,48 it strengthens the argument that there are potential benefits of regulating information about CAM by the government. Organizations such as the National Prescribing Service could be supported to circulate evidence-based consumer information as it becomes available.
There are a number of limitations to the analysis presented. First, information on the length of time that individuals had lived with chronic illness and the severity of disease are not available. Second, the use of many vitamin, mineral, and herb preparations (e.g., calcium and iron) may be prescribed by a medical doctor. Therefore, these products may be viewed and used in the same way as another prescription medication. This cannot be differentiated in the survey from other vitamin, mineral, and herb use, and accordingly the results may overestimate CAM product use. Third, as noted, only limited information is available for CAM practitioner use, and the survey is likely to underestimate the prevalence. Finally, no information is available on why individuals actually choose to use CAM.
Conclusions
This article provides a framework for considering whether government intervention would be justified in the CAM market and the possibilities for any such intervention. It seems clear that the reasoning for intervention in the conventional medicine market is equally warranted in the CAM market. Thinking about the existing policy mechanisms for conventional medicine, there are arguably sufficient means for the government to extend existing policies to cover CAM for regulation of practitioners, products, and information, as well as to potentially subsidize cost-effective modalities. Political will, funding constraints, and various stakeholder opinions are all potential barriers; however, inaction is not supported by these results.
Footnotes
Acknowledgments
The CAMelot Team have contributed to preparation and editing. Funding has been provided by the National Health and Medical Research Council of Australia (NHMRC 491171). Chief Investigators are: Lenore Manderson (Monash); Brian Oldenburg (Monash); Vivian Lin (LaTrobe University); Bruce Hollingsworth (Monash University); Maximilian de Courten (Copenhagen).
Disclosure Statement
No competing financial interests exist.
*
When the model is run without the employment variable, the relationship between higher income and increased probability of CAM use (particularly CAM product use) becomes statistically significant. This is important as CAM product use peaks in the 60–65 year age bracket where the relationship between employment status and income is unclear.