
Abstract
Objectives:
The objective of this study was to compile existing scientific evidence regarding the effects of essential oils (EOs) administered via inhalation for the alleviation of nausea and vomiting.
Methods:
CINAHL, PubMed, and EBSCO Host and Science Direct databases were searched for articles related to the use of EOs and/or aromatherapy for nausea and vomiting. Only articles using English as a language of publication were included. Eligible articles included all forms of evidence (nonexperimental, experimental, case report). Interventions were limited to the use of EOs by inhalation of their vapors to treat symptoms of nausea and vomiting in various conditions regardless of age group. Studies where the intervention did not utilize EOs or were concerned with only alcohol inhalation and trials that combined the use of aromatherapy with other treatments (massage, relaxations, or acupressure) were excluded.
Results:
Five (5) articles met the inclusion criteria encompassing trials with 328 respondents. Their results suggest that the inhaled vapor of peppermint or ginger essential oils not only reduced the incidence and severity of nausea and vomiting but also decreased antiemetic requirements and consequently improved patient satisfaction. However, a definitive conclusion could not be drawn due to methodological flaws in the existing research articles and an acute lack of additional research in this area.
Conclusions:
The existing evidence is encouraging but yet not compelling. Hence, further well-designed large trials are needed before confirmation of EOs effectiveness in treating nausea and vomiting can be strongly substantiated.
Introduction
To date, the main pharmacological intervention for nausea and vomiting involves antiemetic prescription. Considerable progress has been made in antiemetic therapy, particularly with the use of a 5-HT3 receptor antagonist, a highly effective antiemetic, particularly beneficial for high-risk patients, especially chemotherapy and radiotherapy recepients. 4 Nevertheless, despite the availability of this modern treatment, nausea and vomiting remain among the most common symptoms experienced by a large number of patients in medical conditions such as postoperative, chemotherapy, and radiotherapy recipients, with the reported incidence reaching to over 50% of the populations. 5 –7 Self-care remedies such as drinking ginger or peppermint teas, eating bland foods, and relaxation have been commonly attempted, especially for temporary or mild nausea and vomiting. 3,8 Unfortunately, nausea and vomiting can also impose negative impacts on the quality of life (QoL), 9 thus warranting greater attention to improve patients' health outcomes. With an emphasis on improvements in current practices along with the increasing demand for holistic care, the integration of complementary therapies into mainstream treatment may help to achieve desirable patient outcomes.
Aromatherapy refers to the therapeutic use of fragrant substances, called essential oils (EOs), to help improve physical and mental health and QoL 10 and represents a possible form of complementary and alternative medicine (CAM) for nausea and vomiting. EOs are usually obtained by steam distillation of aromatic plants, 11 whereas other kinds of extracts that are not obtained by steam distillation are not considered as EOs. 12 Different aromatic plants produce EOs with different fragrance and therapeutic characteristics depending on their chemical constituents. 13 For example, lavender (Lavandula angustifolia) and its main constituents, linalyl acetate and linalool, exhibit local anesthetic effects in animal in vitro models. 14 Additionally, in other animal studies, α-bisabolol from chamomile (Matricaria recutita) EOs was identified as having strong anti-inflammatory effects. 15 The main therapeutic properties of EOs also include antiseptic, antibacterial, wound-healing, immune-stimulant, as well as calming, sedative, analgesic, uplifting, and stimulating effects. 16
For thousands of years, aromatherapy has been used in countries such as Egypt and India as an ancient tradition of herbal medicine. 17 Aromatherapy could be applied either through inhalation of fragrances, topical application (with or without massage enhancement), or both. In France, the practice of medical aromatherapy involves internal use (ingestion) of EOs 15 such as the consumption of peppermint (Mentha piperita) oils for gastrointestinal disorders to reduce colonic spasm during colonoscopy 18 and the symptoms of irritable bowel syndrome. 19 Other than that, EOs can also be diffused in the air, added in the warm bath water, or used in plant poultices or compresses. However, for the purpose of this review, the focus is on the therapeutic use of EOs primarily via inhalation of its vapors. Due to its advantage of being a noninvasive and relatively low-risk treatment, aromatherapy could serve as a promising modality to improve patient care. 20 However, with the advances of evidence-based medicine, empirical research is consistently required to evaluate the efficacy of this treatment modality. For the time being, substantial evidence for clinical trials on aromatherapy is limited to relaxation alone. 15
Despite the limited clinical evidence, there are encouraging indications from basic science research that certain EO vapors are absorbed by inhalation and alter brain function. 21 –23 Herz 24 proposed two hypothetical mechanisms for the effects of odors on mood, behavior, and physiology: pharmacologic and psychologic mechanisms. Pharmacologically, the fragrances of EOs may deliver direct effects on the central/autonomic nervous system and endocrine system regardless of conscious evaluation. Following inhalation, volatile EO molecules pass to olfactory receptors in the nose, which recognize their molecular characteristics, and send signals to the brain via the olfactory nerve. In addition, some of the constituents pass into the bloodstream via the lungs and consequently produce their effects directly on brain neurons after passing through the blood–brain barrier. 25 Apart from that, based on psychologic hypothesis, the potential effects of smell depend on emotional learning, conscious perception, as well as belief and expectations. As such, the perceived quality of the odors is also accountable for the individual responses.
Although aromatherapy represents the most regularly practiced CAM modality by users, it is also one of the least-researched therapies. At the present time, there are no reviews for aromatherapy on the Cochrane database. 26 A new review is in process as a team is updating the review and preparing a protocol to evaluate the effectiveness of aromatherapy for postoperative nausea and vomiting 26 (this was also confirmed through personal communication with the main author). As such, the objective of the current review is to compile the currently available scientific evidence on the effects of aromatherapy for nausea and vomiting.
Methods
The authors sought to identify all clinical trials and reviews involving the therapeutic use of inhaled aromatherapy to alleviate nausea and vomiting. Eligible articles included all forms of evidence (nonexperimental, experimental, case report). Interventions were limited to the use of EOs by vapor inhalation to treat symptoms of nausea and vomiting in various conditions regardless of age group. Studies where the intervention did not utilize EOs or were concerned with only alcohol inhalation and trials that combined the use of aromatherapy with other treatments (massage, relaxations, or acupressure) were excluded. An inclusive search for clinical research was carried out in major biomedical, nursing, and specialist CAM databases such as CINAHL, PubMed, EBSCO Host, and Science Direct. The search encompassed all articles published by the end of November 2010. The basic search terms used included
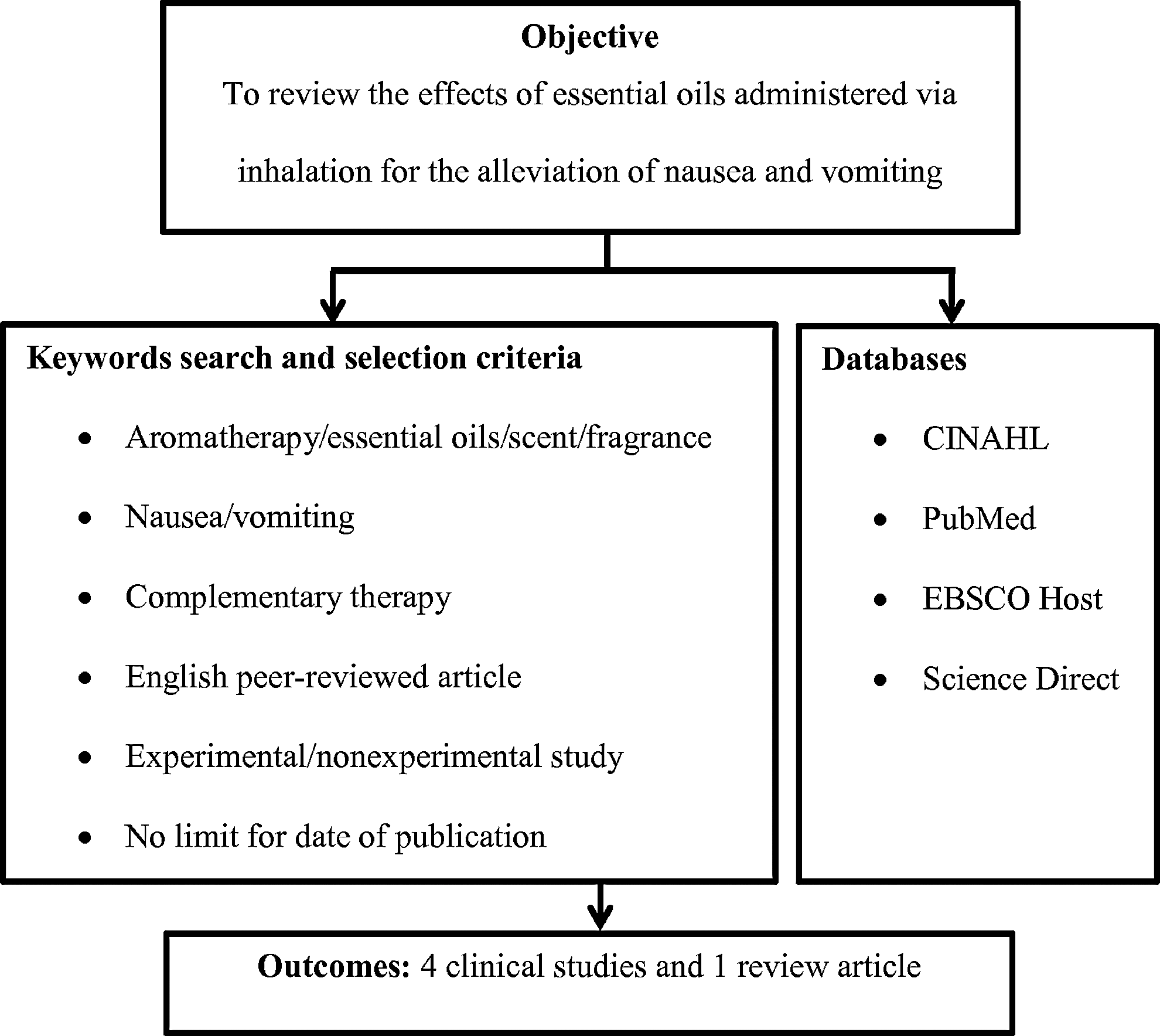
The flow in the literature search process.
Results
All reviewed studies are summarized in Table 1. The searches identified four clinical studies and one review article involving a total of 328 study participants. Three (3) studies investigated postoperative nausea and vomiting (PONV) and one study focused on oncology nausea and vomiting. All studies concluded that inhaled aromatherapy served as an effective treatment for the nausea and vomiting. Other considerations for practical use of aromatherapy included the reduction in antiemetic requirement such as prochlorperazine, droperidol, ondansetron, or metoclopramide, increased patient satisfaction, and improved cost effectiveness.
These studies varied from simple observational studies to the use of a randomized controlled trial. The outcomes evaluated included PONV and oncology nausea. Visual analog scale (VAS), standard descriptive ordinal scale, nausea section of the Edmonton Symptom Assessment System (ESAS), as well as the reported incidence were the instruments used to measure the intended outcomes. In the Anderson and Gross 5 trial, a 100-mm VAS was rated by the respondents at 2 and 5 minutes postintervention. A study by Tate 27 collected the information related to nausea on a 4-hourly and 12-hourly basis.
The interventions also differed as evidenced by the use of a variety of EOs. In two studies, peppermint oil was used for nausea and vomiting treatment in the experimental group. 5,27 Specifically in one trial, patients were asked to inhale the vapors deeply through the nose three times from a scented gauze pad held directly under their nostril, then to exhale slowly through the mouth. 5 In another study, consenting patients were also offered peppermint oils that were administered through the inhaler for 5 seconds. 28 Geiger 25 used ginger essential oil in his study in which 5% Zingiber officinalis (ginger) in grape-seed oil was applied below the nose immediately before surgery. Additionally, the solution was put on the pulse-points of both wrists for patients to sniff if they experienced nausea postoperatively. The Stringer and Donald 29 trial employed a personalized aromatherapy inhalation device, known as Aromastick, whereby a choice of two blends of essential oils was available for patients to choose. One of the revealed blends consisted of peppermint and lemon (Citrus limonum). This device was held by patients approximately 6 inches under their nose while breathing in and it could be used as necessary, allowing self-symptom management.
Three (3) studies of controlled trials reported using different controls or placebos. Geiger 25 and Tate 27 compared their aromatherapy intervention to a no-treatment group. Additionally, peppermint essence was also used in the study by Tate 27 in his three-arm evaluations to assess the efficacy of peppermint EOs for PONV. Conversely, the respondents in the Anderson 5 trial were provided with placebo gauze pads prepared by placing 2 mL of isotonic saline.
A substantial number of patients had reported the benefits of using aromatherapy. This was evidenced by 82% of respondents indicating the benefits of Aromasticks for nausea management whereby almost half (47%) settled their nausea problem. 29 Another study also showed that 80% of high-risk patients did not experience PONV after the application of 5% ginger EOs nasocutaneously. 25 In addition, self-reported nausea score was significantly different between the placebo and experimental groups. 27 Despite overall nausea score decreasing significantly after aromatherapy administration, the reduction was independent of treatment 5 attributed to the favorable effects of controlled breathing patterns.
Discussion
Study outcomes
The overall findings from the reviewed studies suggest that aromatherapy can offer beneficial effects for nausea and vomiting. However, there are very few published research articles as well as apparent methodological flaws on this subject matter, providing room for improvement. Most of the studies included had examined the efficacy of aromatherapy on PONV patients, enabling the possibility of evaluating its effectiveness for various types of clients. However, they were confined only to limited sample sizes (n=17–160) and their study designs were not entirely satisfactory. Difficulties in recruiting and retaining patients were problems common to all clinical trials due to the use of broad exclusion criteria and inadequate outreach to populations such as individuals with low income, ethnic minorities, and the elderly. 30 This factor would limit the patient participation and clearly reduce generalizability. With only one study adopting a randomized control design, 5 attempts to evaluate the actual clinical benefit of this complementary therapy remain challenging.
Placebo/control
Selecting the appropriate placebo for aromatherapy intervention can be difficult. Wiebe 31 suggested that the control for CAM trials should sufficiently mimic active treatment to support the blinding of patients. 32 For instance, the study by Tate 27 used a fragrance-matched artificial placebo (peppermint essence) as a comparator, lacking in menthol composition compared to peppermint EOs. Most aromatherapists believe that synthetic fragrances are inferior to EOs, although they are often composed of many of the same compounds. 33 This is because synthetic fragrances lack natural or vital energy; however, this has been contested by odor psychologists and biochemists who believe in the importance of therapeutic odor in treating various illnesses. 34 Menthyl acetate, which is responsible for peppermint's minty aroma and flavor, 35 might also be favorable in nausea conditions. However, because adaptation to the odorant occurs quickly (in which the smell receptors become less responsive to respond to repeated or continued stimuli of constant odor intensity), this condition reduces the potency of the odor to treat an ill condition, thus supporting the pharmacologic effects of EOs. 34,36 Therefore, the respondents could be blinded by using peppermint essence, since the smell was similar except it was devoid of the active therapeutic compound in peppermint essential oils (menthol). However, an experienced practitioner might be able to distinguish the differences considering the lack in menthol in peppermint essence, hence moderating its cool sensation properties. As such, the evaluation on the blinding may give valuable information, especially in adopting a double-blind study design. For instance, Graham et al. 37 revealed that their attempts to blind patients for aromatherapy intervention were not 100% effective, although most were uncertain or wrong about the treatment they actually received. Therefore, it is important for future trials to choose the appropriate placebo as well as to conduct the blinding assessment in order to minimize (if not eliminate) the placebo detection effect.
Assessment methods
There were no standard and consistent measures to assess nausea and vomiting. Three (3) studies measured the severity of nausea either using the VAS, nausea section of ESAS, or a standardized descriptive ordinal scale, whereas another two studies only reported the incidence of the symptoms. VAS is commonly used to measure a variety of subjective responses including the assessment of “feeling.” 38 Generally, it consists of a 100-mm-long line in which the lower anchor end corresponds to “no symptom” and the higher anchor end signifies “unbearable symptom.” Nausea intensity measurement using VAS serves an advantage over other methods, considering that continuous data have ratio properties and are well suited for statistical analysis, unlike categorical scales 38 in the nausea section of ESAS or standardized descriptive ordinal scale. This instrument is also easy to be self-administered for the patients because of its simplicity and speed of completion as well as being unhindered by a language barrier. 39 However, the estimation of nausea intensity with VAS requires an ability to transform a complex subjective experience to a visual–spatial display, which involves perceptual judgment and accuracy. Potential investigator bias might also occur, since patients may require lengthy instructions from trained staff before completion. Despite these limitations, VAS may still serve as a useful self-reported tool in assessing nausea and vomiting considering individual subjective perception of these symptoms.
Essential oils (EOs)
Inconsistencies in terms of the type of EOs and how they were delivered (including dose, blended or single oil used) hampered comparisons between these studies. Peppermint and ginger oils have been regularly used in the aromatherapy intervention for nausea, using various methods of administration including oral preparations. The selection of these EOs was associated with the role of their chemical constituents, which help in the relief of gastrointestinal symptoms. 24,26 Peppermint oils have been shown to be an effective remedy for morning sickness, dyspepsia, and other gastrointestinal complaints; its effectiveness is attributed to its antispasmodic properties. 40 In addition, the botanical form of ginger was often advocated as beneficial for nausea and vomiting in various conditions including motion sickness, pregnancy-induced and postoperative conditions. 41-42 On the other hand, aromatherapists particularly use the EOs in a blend form, since they are believed to be more effective as the therapeutic value is generated by the reaction and balance of the oils' constituents. 33 The evidence from the Stringer and Donald 29 trial on the effectiveness of blended EOs to reduce nausea and vomiting is still debatable, as its retrospective design prevented the exclusion of various study biases. Considering these facts, the important issues mentioned need to be further explored to maximize the potential benefits of EOs use via inhaled aromatherapy.
Side-effects
No known side-effects prior to aromatherapy administration were reported by these studies, suggesting the minimal invasive property of these EOs. In fact, only a few isolated cases of allergic reactions were documented in the literature. 43 Yet, with its volatility and the skin's absorbent nature, some EOs do possess the potential to initiate allergic reactions. 44 Aromatherapy oil should therefore not be considered as a safe alternative to existing pharmacotherapy until rigorous safety trials have been completed. Concerning inhalational aromatherapy, only one incidence of idiosyncratic allergic reactions with Anthemis nobilis essential oils was reported (after inhalation of one drop of smelling strip). 44 This incidence was among two serious cases that were indicated by the author after 10 years of teaching in aromatherapy. Thus, although the reviewed studies had not indicated any untoward incidences, the risk still exists, requiring precautionary measures to minimize any unwanted consequences from EOs use.
Outcomes on antiemetic use
The reported outcomes in these reviewed studies have also highlighted the reduction in the use of analgesic and antiemetic medications. These positive responses are of value for extrapolating to gauge the benefits toward less inherent expenses and potential side-effects related to the pharmacologic interventions, although the claims were not based on validated outcomes measures. Therefore, future trials are recommended, which should include an analysis of medication use as a result of aromatherapy administration as well as cost effectiveness assessment related to this complementary treatment.
Limitations
Despite the rather captivating findings from this review, there are several limitations that need to be mentioned. First, only five articles were reviewed and more than half of the studies used small sample sizes. Even though a thorough research strategy was employed, it cannot be assured that all relevant trials have been located. Second, although all the studies have stated that the aromatherapy intervention was administered via inhalation, the method and duration varied widely, which may directly or indirectly influence the outcomes. Third, due to the restriction imposed by the search selection criteria, only one study was a randomized controlled trial, while the others were using a quasi-experimental design. No scoring system or quality assessment for data extraction was adopted for this review, considering the subdued data and the small number of available studies that satisfied the selection criteria. Although the excluded studies are not displayed in this review, the inclusion criteria had served as a precise tool in selecting the articles through which non-peer-reviewed publications such as dissertations and non-English articles were excluded.
Conclusions
In summary, it is concluded that inhaled aromatherapy using peppermint and ginger EOs may have potential benefits in alleviating nausea and vomiting in postoperative and oncology patients. Although the overall outcomes seem promising, methodological weaknesses such as small sample sizes, quasi-experimental design, imprecise measuring tools, inappropriate placebo, and varied doses or methods of EOs application restricted these studies, thus compromising any concrete conclusion. Hence, studies of this nature need to be further replicated and improved before confirmation of the effectiveness of EOs in treating nausea and vomiting can be strongly substantiated.
Footnotes
Acknowledgments
The authors would like to sincerely thank Associate Professor Dr. Nik Mazlan Mamat, Dean, Kulliyyah of Allied Health Sciences, International Islamic University Malaysia (IIUM) for his support and guidance.
Disclosure Statement
No competing financial interests exist.