
Abstract
Background:
Multiple clinical trials within the past decade have aimed to study the safety and efficacy of various probiotic strains in treating patients with irritable bowel syndrome (IBS). However, there exists much heterogenicity in study design among these trials, namely, in bacterial strain, dose, dosage form, sample size, study duration, and population demographics.
Aim:
The aim of this study was to identify the shortcomings of clinical trials using probiotic treatments in subjects with IBS, so that researchers may realize where limitations exist, allowing them to curtail these limitations in future trials.
Methods:
An extensive PubMed search was conducted using the following keywords:
Results:
Stark differences in study design existed among the 20 original articles analyzed, as well as an outstandingly high “placebo effect,” making the ability to compare these articles as a means for evidence-based treatment therapy in IBS very difficult.
Conclusions:
Future large, randomized, double-blind, placebo-controlled clinical trials must be conducted, embodying minimal variability in study designs, to appropriately assess the efficacy of specific probiotic strains over placebo.
Introduction
Pathophysiology of IBS
Although there are many proposed mechanisms of IBS, the exact pathophysiology remains unclear. Three (3) proposed mechanisms include visceral hypersensitivity, altered bacterial environment in the gut, and small bowel inflammation.
Visceral hypersensitivity in IBS may result from altered somatovisceral and motor dysfunction of the intestine from a variety of causes. 6 These causes include genetics, motility factors, colonic infections, mechanical irritation to local nerves, inflammation, stress, and other psychologic factors. Abdominal pain in IBS has been shown to be associated with degranulating mast cells releasing tryptase and histamine in close proximity to colonic nerves in the gastrointestinal (GI) tract, causing inflammation, and subsequently, pain, locally. 7 A preclinical trial conducted in 2007 showed that administration of Lactobacillus acidophilus induced the expression of opioid and cannabinoid receptors in the colonic epithelial cells, decreasing pain radiation in that area. 8
Second, an imbalance of gut flora in the GI tract may lead to the overgrowth of pathogenic bacteria causing fermentation, gas, bloating, and abdominal pain. Several studies indicate that IBS patients have different fecal flora when compared with healthy controls. 9 –11 One (1) study shows that patients with IBS have an increase in hydrogen gas production in the gut due to the abundance of pathogenic bacteria. 12 Supplementation with Lactobacillis plantarum has been shown to decrease colonization of bacterial groups with gas-producing ability, such as clostridia, 13 indicating that probiotic supplementation may be useful in treating IBS symptoms such as flatulence.
Lastly, IBS symptoms may be caused by increased inflammation of the GI tract. 14 –17 O'Mahony et al. showed that patients with IBS have an abnormal interleukin-10 (IL-10)/IL-12 (anti-inflammatory/proinflammatory) ratio compared to otherwise healthy controls. Bifidobacterium infantis 35624 therapy was shown to normalize this ratio, by boosting IL-10 levels, and decreasing IL-12 levels, with a net effect of decreased inflammation. 14
Recent IBS clinical trials using probiotic therapy have shown mixed efficacy results. One (1) recent study published in 2010 shows the unfavorable effects of L. plantarum MF 1298 versus placebo in a cross over study. 18 Another trial conducted by Drouault-Holowacz et al. shows that a probiotic combination was not significantly superior to placebo in relieving symptoms of IBS. 19 Although almost all of these trials are randomized, placebo-controlled, double-blinded studies, it is important to note the lack of standardization among them. It is difficult to compare these trials due to differences in bacterial strain, dose (in colony forming units [cfu]), dosage form, dosing interval, study duration, demographics, endpoint measures, and sample size.
Clinical trials conducted in IBS also have a remarkable “placebo effect,” with a mean response rate between 36% and 40.2%, making it harder for these trials to prove probiotic efficacy over placebo. 20,21 Also, there are limited pharmacokinetic data on current probiotic strains; therefore, bacterial dose, dosing interval, and duration of clinical trials vary. However, there have been a few causal studies determining dose–response relationships with certain probiotic strains. O'Sullivan et al. concluded that the recommended dosage for Lactobacillus GG to achieve intestinal colonization was 1×1010 cfu. 22 Whorwell et al. analyzed B. infantis 35624 in a population of 362 women and found that a dose of 1×108 cfu provided the greatest benefit in reducing the primary outcome of abdominal pain/discomfort. 23
This review will aim to address the lack of standardization of probiotic clinical trials in patients with IBS over the past decade and warrant the need for better-controlled clinical trials with probiotic treatment in patients with IBS in the future.
Methods
A literature search was completed using the U.S. National Library of Medicine PubMed database using the terms
Results
Bacterial genus and species and number of CFU
Comparison among clinical trials is much easier when variables throughout the trial's design and execution are limited. Variables in clinical trials can vary depending on which disease state and treatment are being analyzed. With probiotic treatments in IBS, there is a vast array of variables, particularly in the bacterial strain or strains that are utilized, and which dose (in cfu) is decided upon (Table 1). There are also very limited data pertaining to which bacterial strain and dose are most efficacious in this disease state, although most available trials have suggested that Bifidobacteria and Lactobacillus genuses appear to have the most efficacy in IBS. 24 –27 There are no two clinical trials researched for this review that include the same bacterial strain at the same dose. There are two sets of trials that use the same bacterial strain at differing doses, which include B. infantis 35624, 14,23 and VSL#3, a probiotic combination. 28,29 B. infantis 35624 is used in the first trial at varying doses of 1×106, 1×108, and 1×1010 for dose optimization, and in the second trial at 1×1010 cfu. 14,23 Similarly, the probiotic combination VSL#3, which contains B. infantis 35624, was used in doses of 450 billion lyophilized bacteria/day, 28 or 900 billion lyophilized bacteria/day. 29 There are also three clinical trials that use the same bacterial genus and species, but differ in strain and dose. 1,18,30 These trials all share the L. plantarum genus and species. One trial uses strain 299V at a dose of 5×107 cfu/mL, 1 another uses MF 1298 at a dose of 1×1010 cfu/capsule, 18 and another uses DSM 9843 at 5×107cfu/mL. 18 These studies proved unsuccessful in optimizing strain and dose, two variables that definitely pose a challenge when comparing the results of these studies.
cfu, colony forming units.
When considering an oral probiotic supplement, a strong emphasis is placed on the probiotic's ability to surpass stomach hydrochloric acid and degradation by bile salts to reach its site of action in the small intestine. The ability of probiotic strains to hydrolyze bile salts, using bile salt hydrolases (BSHs), is an important determinant in bacterial strain selection. It has been found that certain bacterial strains possess a higher ability to penetrate to the small intestine than others. For example, one study comparing Lactobacillus reuteri and Bifidobacterium longum in vitro found that microencapsulated L. reuteri capsules had better BSH activity than the B. longum did, suggesting the use of L. reuteri for targeted delivery into the GI tract due to its ability to metabolize bile salts. 31 However, microbial BSH activity has also been suggested to be potentially detrimental to the human host, and thus it has not yet been agreed upon as to whether high BSH activity is a desirable trait of a bacterial strain. 32
There is also an overabundance of studies in this review utilizing probiotic “cocktails,” which combine multiple bacterial strains in one product. 19,28,29,33 –38 These trials make it difficult to distinguish which bacterial strain or strains are actually causing a therapeutic benefit, or if an additive or synergistic effect exists between particular bacterial strains. One trial conducted in 2005 by Kajander et al. suggests that IBS is a multietiological condition and that a probiotic mixture may be more efficacious than a single strain for treatment. 34 This hypothesis may be the reason that many clinical trials use probiotic “cocktails” to prove therapeutic benefit over placebo. The only way to prove efficacy of a particular bacterial strain and dose is to conduct a randomized, double-blind, placebo-controlled clinical trial assessing the efficacy of one particular bacterial strain at a time.
IBS diagnostic criteria, study population, and sample size
The most widely used and up-to-date criterion to diagnose IBS is the Rome III criteria, last updated in 2006. The Rome criteria is a system “developed to classify the functional gastrointestinal disorders (FGIDs) of the digestive system in which symptoms cannot be explained by the presence of structural or tissue abnormality, based on clinical symptoms.” 39 Rome III criteria defines IBS as recurrent abdominal pain or discomfort at least 3 days/month in the last 3 months associated with two or more of the following: improvement of pain with defecation, onset of pain associated with change in frequency of stool, and onset of pain associated with a change in form (appearance) of stool. Because it is almost 5 years since Rome III has been updated, and IBS is an emerging disease, one can see the need for updated IBS guidelines. However, at the time most of the trials utilized in this review were conducted, various Rome criteria (I, II, and III) were available, so clinicians made an attempt to use the newest criteria available to them (Table 2). There exists much disparity in the Rome criteria utilized in this review, with only three trials using the Rome III criteria. 37,40,41 Some trials did not use Rome criteria at all, and one in L. plantarum 299V used “generally accepted criteria, which constituted a combination of abdominal pain and two or more of the Manning criteria.” 1
Many studies analyzed in this review contain more female than male subjects, with only few possessing equal gender numbers, or more male subjects than females subjects (Table 1). Gawronska et al. and Enck et al. both had more male subjects than females in the treatment group only, not in the placebo group. 36,42 Zeng et al. and Hong et al. both had more male subjects than females subjects. 33,37 It is essential to match baseline gender characteristics in all clinical trials so as to not limit how applicable the results may be among genders.
The largest probiotic clinical trial in patients with IBS included in this review was conducted in 362 subjects, 23 whereas some of the smallest trials included less than 30 subjects. 18,22,28,33,42 Although there were 362 subjects in the largest trial, most trials were conducted in anywhere from 20 to 70 subjects, indicating that the median would be a better measure of central tendency than the mean with associated values of 62.5 and 105.1 subjects, respectively (Fig. 1).
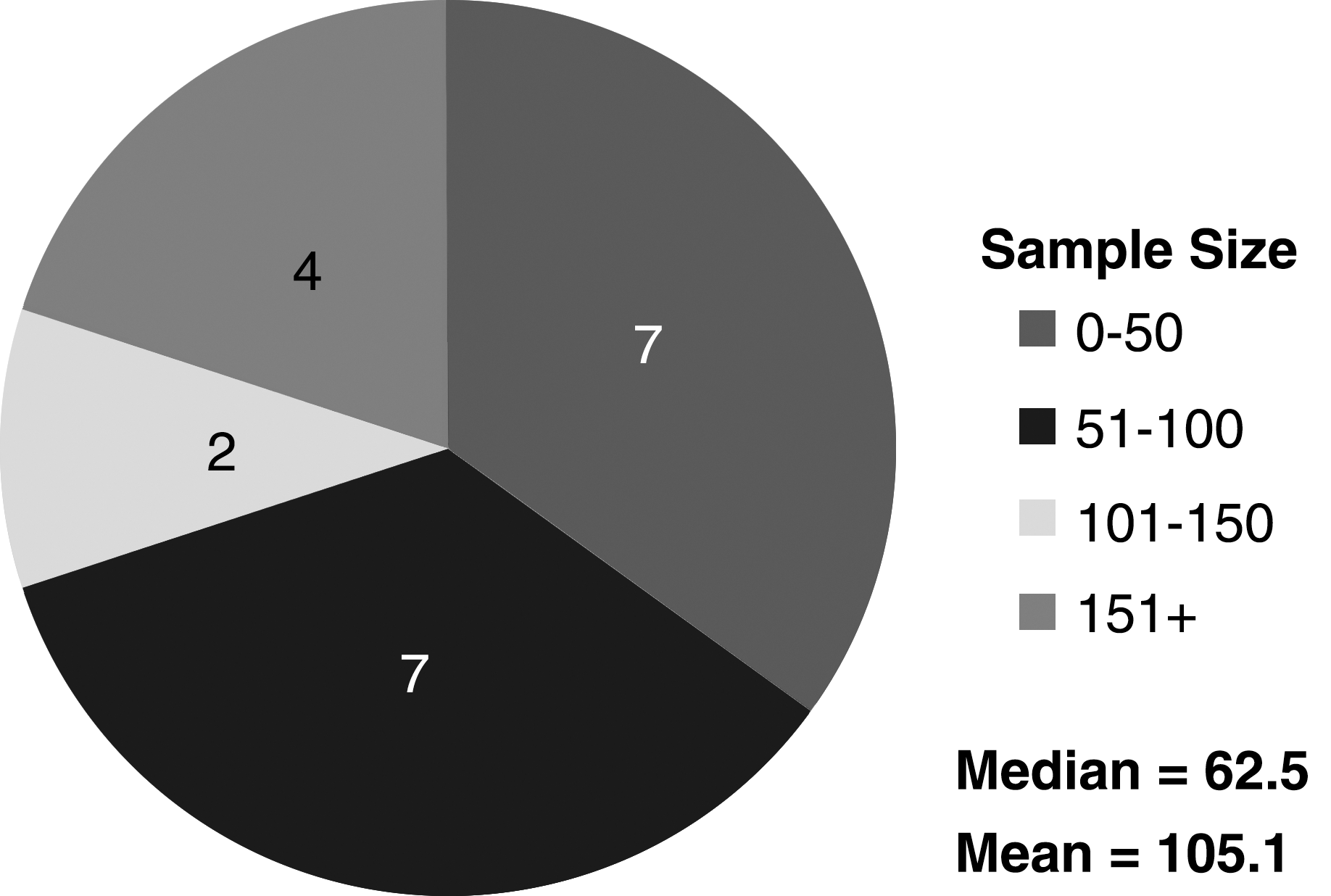
Pie chart depicting trial sample sizes.
Dosage form, interval, and study duration
Dosage form differences may play a significant role in decreasing the homogenicity of the trials herein. As mentioned earlier, pharmacokinetic data on most all probiotic strains are unclear and further investigation is needed to determine appropriate pharmacokinetic parameters for specific strains. Therefore, researchers must estimate dosage form, dosage intervals, and trial durations based upon previous conducted trials and in vitro pilot studies. Most trials researched in this review have dosing intervals ranging from once daily to twice daily, and use 4, 6, or 8-week trial durations (Table 3). Sinn et al. list the absence of pharmacokinetic data in their trial comparing Lactobacillus acidophilus-SDC 2012, 2013 as a limitation, mentioning, “the encapsulated product was not tested for its shelf stability, effectiveness of delivery, or intestinal survival.” 40 Secondly, the optimal dosage of L. acidophilus-SDC 2012, 2013 for administration was not determined.
All preparations were administered orally.
Other dosage forms depicted in the trials researched for this review include: a fruity drink containing 5% of an oatmeal soup, 1 a malted milk drink, 14 fermented milk, 33,35 Prosymbioflor, 36 Flortec, 43 powder sachets to be dissolved in water, 19,37 capsules, 13,34,38,40 –42 and powder sachets to be dissolved in yogurt. 28,29 This variety of oral dosage forms again hinders inter-trial homogeneity.
Subjective study endpoint measures
Study endpoints should be objective in nature and have hard outcome measures to eliminate subject biases and reduce the placebo effect. The more definitive the outcome measures, the more reliable the study results. Objective study outcomes should aim to be uniform across all clinical trials of a particular disease state to help standardize trial results and decrease the complexity of inter-trial comparison. IBS, by nature, is an extremely subjective disease. IBS subjects with the same theoretical abdominal pain level may rate their pain severity differently on the same scoring scale. The IBS clinical trials assessed in this review usually used validated questionnaires or scales to measure HRQoL and primary study endpoints. Examples include: the Functional Digestive Disorders Quality of Life Questionnaire,[44] Gastrointestinal Symptom Rating Scale, 33 RAND 36-item health survey, 34,45 IBS Symptom Severity Index, 35,46 Visual Analog Scales, 14,29,30 and the Likert scale (0–5). 14,22 One other highly validated scale, the 7-point Bristol stool form scale, is used widely among trials to measure the consistency of bowel movements. 23,29,35,37,40,47 Other studies used nonvalidated questionnaires such as global symptom scores, improvement scores, treatment preference, and symptom severity scores. 1,18,28,36,38,41 –43
Remarkable “placebo effect”
As with all clinical trials, the “placebo effect” is of great concern to study authors and designers when preparing a study. The lower the placebo effect and the greater the therapeutic effect, the less probability that the results are due to chance, and the stronger they can be weighted. Clinical trials conducted in patients with IBS tend to have a particularly high placebo effect, usually between 30% and 50%. 20,21 It is known that IBS is a condition with few outcomes that are able to be objectively measured. Therefore, there is a high degree of subjectivity in many outcomes of IBS clinical trials, as mentioned above. More subjectivity across patient populations may lead to a higher placebo effect. Patel et al. and Pitz et al. state in their meta-analysis and review article, respectively, that more stringent entry criteria, an increased number of office visits, once-daily placebo dosing, and a crossover study design have been helpful in decreasing the placebo effect in IBS clinical trials. 20,21
Expectation is also an important determinant of the placebo response. 21 If patients are told they are receiving a drug to alleviate a particular condition, the patient will expect the signs and symptoms of that condition to dissipate. “In a study of gastric motility assessment using a magnet imbedded in a placebo pill, patients were told they were receiving a relaxant, a stimulant, or a placebo at different times. Gastric motility was consistent with the patient's expectations for each treatment.” 21,48 It is important to note that this study was conducted over 40 years ago and the expectation of the placebo response may be different in today's population.
Discussion
Probiotics as mainstays in IBS
Probiotics continue to serve as mainstays in IBS therapy because newer, serotonin-modulating medications, alosteron and tegaserod, have either been pulled from the market, or their indicated populations narrowed after being on the market for some time. Alosetron, a 5-HT3 antagonist used for diarrhea-predominant IBS in women, was voluntarily removed from the market in November 2000 due to serious, but infrequent, adverse events such as ischemic colitis and severe constipation. 49 Alosetron was placed back on the market in 2002 with a Risk Management Plan due to overwhelming public interest. However, since it has been reintroduced, alosetron use has been vastly limited. A risk/benefit study was conducted by Johnson et al., and showed that women were willing to tolerate a 2.65% increase in impacted-bowel risk with administration of alosetron. 50
Tegaserod, a 5-HT4 agonist used for treating constipation-predominant IBS, was suspended from the market in March 2007 due to an increased risk of serious cardiovascular ischemic events (CVIE). There is conflicting evidence on the prevalence of cardiovascular events with this treatment. A very large observational cohort study showed that there was no increased risk of CVIE with tegaserod treatment, 51 with other trials showing similar results. 52 –54 One (1) smaller retrospective trial in 67 patients showed that cardiovascular events during tegaserod therapy may be increased in patients with other risk factors for cardiovascular events, and that tegaserod use should not extend to this population. 55 Lastly, one case report indicated that a man experienced a MI after only two 6-mg doses of tegaserod. 56 In summation, alosetron and tegaserod both have the potential to cause severe, but infrequent adverse events.
Probiotics in the military
The military has also discussed the use of probiotic-containing foods to be dispensed in dining facilities to prevent or treat acute infectious diarrhea, IBS, respiratory tract infections, allergic rhinitis, dental health issues, and female urogenital conditions. 57 In IBS, the review concluded, “the evidence strongly indicates that probiotics are efficacious for the improvement of IBS symptoms in adults. However, the exact species, quantity, and duration of supplementation need to be further studied.” 57
The placebo effect
Patients with IBS responded extremely well to probiotic therapy in the clinical trials analyzed for this review. They also, however, responded extremely well to placebo in these trials. The rate of such a high placebo effect in this population (mean response between 30% and 50%) could be due to the fact that patients with IBS have very burdensome symptoms, are anxious to be treated, and may respond to any alteration in therapy, even if that alteration is placebo. Therefore, it is difficult to conclude from these trials whether or not probiotics have a distinct advantage over placebo in treating IBS symptomatology. For example, Kim et al. found no difference in proportion of responders for satisfactory relief of bloating, stool-related symptoms, abdominal pain, and bloating scores, in probiotic VSL#3 versus placebo. 29 Niedzielin et al. found that all 20 patients with L. plantarum 299V treatment experienced an improvement from baseline in abdominal pain, whereas 11/20 (55%) experienced improvement in the placebo group. 1 This high placebo effect trend continues among trials, using a variety of endpoint measures. 5,18,19,22,23,28,30,35,37,38,42
Conclusions
Probiotics may be useful in treating a variety of conditions experienced by a wide audience, namely, IBS. There is a need for properly conducted probiotic clinical trials to increase the rate at which probiotics are prescribed and recommended by physicians. Most all practitioners rely on evidence-based medicine to prescribe medications for their intended purposes. Some practitioners may prescribe medications for “off-label” uses, but not all are comfortable with that approach. As mentioned throughout this review, several factors complicate the interpretation of these trials. Future clinical trials must aim to standardize the following variables to make the results as clinically meaningful as possible: IBS diagnostic criteria, bacterial strain, dose, dosing interval, dosage form, study demographics, and study duration. With these criteria met, the results of future clinical trials will prove efficacy of a particular probiotic and will be reproducible to use in a large population. Because IBS has such a high prevalence worldwide, affecting its subjects both emotionally and physiologically, it is of the utmost importance that researchers strive to prove the efficacy of probiotics over placebo in treating patients with IBS.
Footnotes
Disclosure Statement
No financial conflicts exist.