
Abstract
Objective:
The objective of this study was to determine whether prolotherapy, an injection-based complementary treatment for chronic musculoskeletal conditions, improves pain, stiffness, and function in adults with symptomatic knee osteoarthritis (KOA) compared to baseline status.
Design:
This was a prospective, uncontrolled study with 1-year follow-up.
Setting:
The study was conducted in an outpatient setting.
Participants:
Adults with at least 3 months of symptomatic KOA, recruited from clinical and community settings, participated in the study.
Interventions:
Participants received extra-articular injections of 15% dextrose and intra-articular prolotherapy injections of 25% dextrose at 1, 5, and 9 weeks, with as-needed treatments at weeks 13 and 17.
Outcome measures:
Primary outcome measure was the validated Western Ontario McMaster University Osteoarthritis Index (WOMAC). Secondary outcome measure was the validated Knee Pain Scale (KPS). Tertiary outcome measure was procedure-related pain severity and participant satisfaction.
Results:
Thirty-six (36) participants (60±8.7 years old, 21 female) with moderate-to-severe KOA received an average of 4.3±0.7 prolotherapy injection sessions over a 17-week treatment period and reported progressively improved scores during the 52-week study on WOMAC and KPS measures. Participants reported overall WOMAC score improvement 4 weeks after the first injection session (7.6±2.4 points, 17.2%), and continued to improve through the 52-week follow-up (15.9±2.5 points, p<0.001, 36.1%). KPS scores improved in both injected (p<0.001) and uninjected knees (p<0.05). Prescribed low-dose opioid analgesia effectively treated procedure-related pain. Satisfaction was high and there were no adverse events. Female gender, age 46–65 years old, and body–mass index of 25 kg/m2 or less were associated with greater improvement on the WOMAC instrument.
Conclusions:
In adults with moderate to severe KOA, dextrose prolotherapy may result in safe, significant, sustained improvement of knee pain, function, and stiffness scores. Randomized multidisciplinary effectiveness trials including evaluation of potential disease modification are warranted to further assess the effects of prolotherapy for KOA.
Introduction
Prolotherapy is a complementary injection therapy for chronic musculoskeletal pain, including knee osteoarthritis (KOA), 11,12 that has been hypothesized to stimulate healing of chronic soft-tissue injury. Hypertonic dextrose is a commonly used prolotherapy injectant. 11 A single randomized controlled trial (RCT) reported significant improvement in KOA pain scores when treated with prolotherapy 13 ; however, the effectiveness of prolotherapy for KOA using validated measures has not been assessed. Therefore, a prospective uncontrolled pilot study was conducted to test the hypothesis that dextrose prolotherapy improves knee pain, function, and stiffness compared to baseline status in participants with symptomatic moderate to severe KOA.
Methods
The study protocol was approved by the University of Wisconsin Institutional Review Board.
Eligibility criteria and participant recruitment
Adults 40–76 years old were enrolled and followed from July 2004 to July 2008. They were recruited from University of Wisconsin Sports, Rehabilitation and Family Medicine clinics, prior control groups of an ongoing RCT assessing prolotherapy for KOA and the community. Inclusion criteria were a diagnosis of KOA based on clinical criteria for KOA defined by the American Rheumatological Association, 14 identification by a radiologist of KOA on an existing knee radiograph within 5 years, tenderness of one or more anterior knee structures on physical examination conducted by the lead physician (DR), and moderate-to-severe knee pain for at least 3 prior months, defined by scoring “3” or more on the question “What is the average level of your left/right knee pain over the last week?” using a 0–6 ordinal response scale. Exclusion criteria included the following: pregnancy, significant comorbidity (including uncontrolled diabetes mellitus defined as glycosylated hemoglobin >7.5%), anticoagulation therapy, history of, or planned, total knee replacement, prolotherapy or any other knee injection within the past three months, inflammatory or postinfectious knee arthritis, daily use of opioid pain medication, allergy or intolerance to study medication, lack of x-ray report of the affected knee or body–mass index (BMI)>45 kg/m2. Each knee was assessed separately for eligibility. Interested, eligible persons attended an informational meeting and gave informed consent.
Outcome measures
The primary outcome measure was change in the total score of Western Ontario McMaster University Osteoarthritis Index (WOMAC), a validated quality-of-life instrument designed to evaluate KOA severity using pain, stiffness, and function subscales. 15 The WOMAC total score, constructed as the average of the three subscale scores, ranges from 0 to 100, with 100 indicating maximum (best) knee-related quality of life, and has been shown to be responsive to change. Minimal clinical important differences on the WOMAC for KOA have been reported as 12% 16 –25%. 17 Secondary outcomes included the Knee Pain Scale (KPS), 18 a validated questionnaire assessing pain and function of the individual knee. KPS assesses pain frequency using a 0–4 Likert scale, and pain severity using a 0–5 Likert scale, with higher values indicating worse pain frequency/severity. KPS data were collected separately for each treated knee as well as for untreated knees to evaluate whether unilateral prolotherapy could have bilateral effects on knee pain scores. To the authors' knowledge, the minimal clinical important difference has not been published for the KPS. The WOMAC and KPS were collected in person and prior to any procedure at baseline, 5, 9, and 12 weeks, and by phone at 26 and 52 weeks postentry.
Tertiary outcomes included procedure-related pain severity and patient satisfaction. Participants reported pain levels on a 1–7 ordinal response scale immediately following and 2 days after a given injection session. Opioid medication use was recorded (yes/no). Participant satisfaction was assessed by the question “Would you recommend the therapy you received in this study to others with KOA like yours?” (yes/no). Participants were able to make brief qualitative comments about their treatment and clinical response.
Demographics, self-reported weight and height and severity of KOA-related findings on knee radiographs were collected at baseline to characterize the sample and to evaluate as covariates (age, gender, BMI, and x-ray-based KOA severity score) for statistical analysis. A fellowship-trained musculoskeletal radiologist (RK) using the 1–4 Kellgren-Lawrence KOA scoring system 19 evaluated existing, available knee radiographs. Among participants for whom existing radiographs were available and who also received injections on both knees, the more severe of the two radiographs was obtained.
Intervention
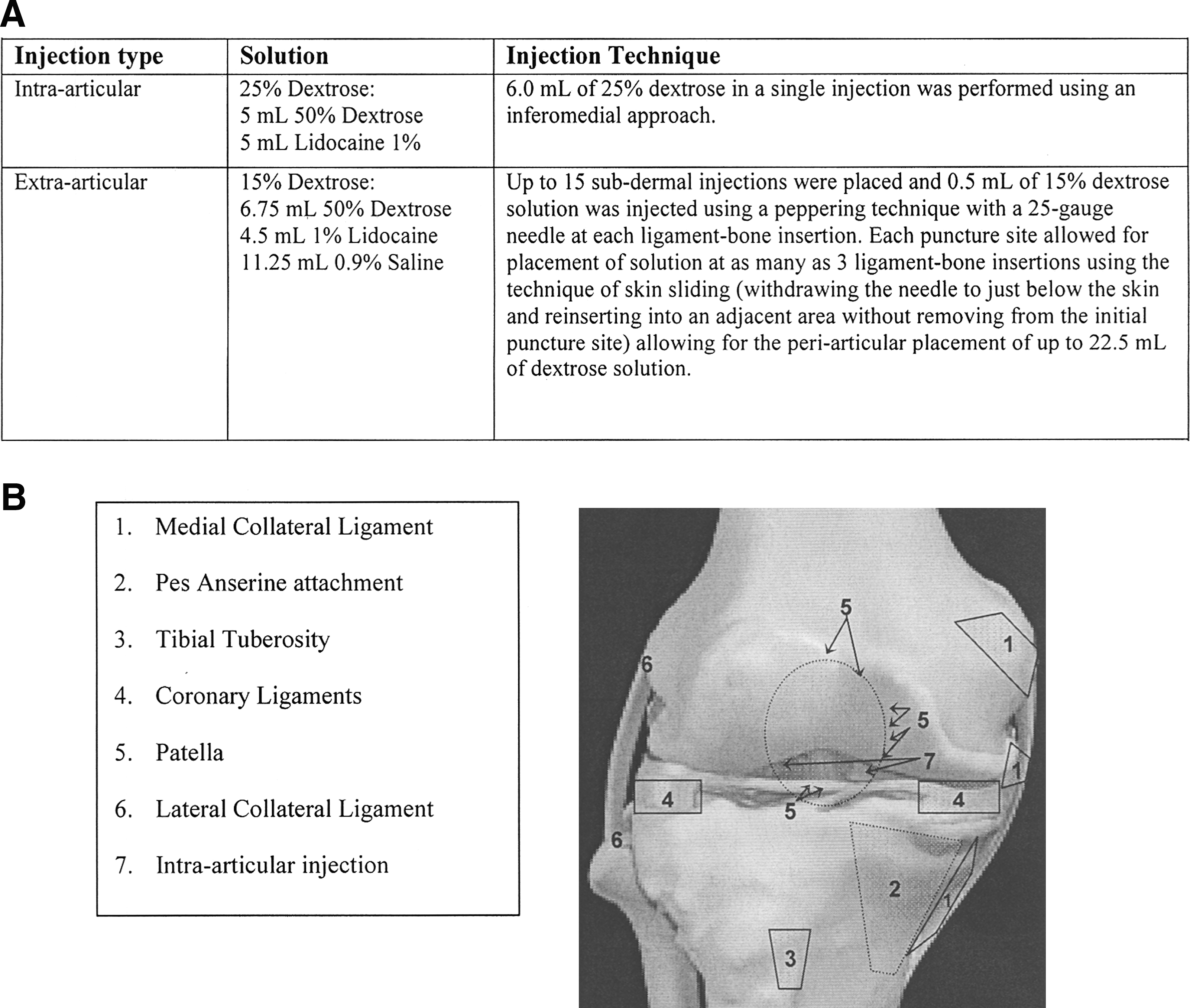
Injections were performed at 1, 5, and 9 weeks postentry, with optional sessions at weeks 13 and 17, per physician (JJP) recommendations and participant preference. Participants were offered an optional single 5-mg oxycodone tablet for analgesia 30 minutes prior to injection. The injector (JJP) examined the knee, marked tender anterior points, placed anesthetic skin wheals of 1% lidocaine and performed injections according to an existing protocol (Fig. 1). 20 Extra-articular injections were done “on bone” at major tender tendon and ligament insertions through up to 15 skin punctures using a peppering technique and placing a possible total 22.5 mL of solution. The single intra-articular injection was 6 mL of 25% dextrose using an inferomedial approach. Postinjection, participants were offered acetaminophen and eight 5-mg oxycodone tablets to use as needed for up to 1 week and were advised to have relative rest for 2–3 days, with progressive resumption of routine activity over 1 month. They were discouraged from using nonsteroidal anti-inflammatory medications and from starting new therapies for knee pain during the study period.
Analysis
Data were analyzed using SAS® 9.1 statistical software (SAS Institute Inc., Cary, NC). Distributional data characteristics were assessed; primary and secondary continuous variables were normally distributed. Descriptive statistics were applied to describe outcomes at each time point; mean value±standard deviation (SD) was reported at baseline unless otherwise specified.
Repeated-measures analysis of variance compared baseline to follow-up WOMAC total and subscale scores and the subscales of the KPS (five time points over the 52-week follow-up period). Mean values±standard error was reported for this analysis. The unit of analysis in the WOMAC model was the participant. Because WOMAC evaluates participant's KOA-specific quality of life regardless of the number of knees (one or two) affected, the analysis of the WOMAC scores was on a “per participant” basis, regardless of whether one or both knees were injected. In addition to the unadjusted repeated-measures analysis, covariate analyses were also conducted, based on interaction of the covariates with the time-related trend in the model. Separate covariate analyses were conducted for participant age, gender, BMI, race, education, income, tobacco use, diabetes, prior knee surgery, Kellgren-Lawrence severity, and duration of knee pain. Percent improvement in WOMAC scores was calculated as the percentage change in total WOMAC score from baseline to 52 weeks relative to the potential improvement obtainable (100 minus the baseline). The number needed to treat (NNT) to achieve a minimal clinical important difference of 12% on the WOMAC total score, 16 and to achieve overall improvement of 25% and 50% were calculated.
The unit of analysis for the KPS model was the individual knee. Because KPS assesses each knee separately (that is, each participant completes two KPS questionnaires at each time point: one per knee), the KPS scores for each knee were analyzed individually. If a participant had both knees treated, that participant accounted for two knees in the treated-knees model. A hierarchical repeated-measures model corrected the standard errors for the interaction between the reports on two knees by the same individual.
A separate repeated-measures model analyzed KPS scores for knees that were not treated during the study. The model included untreated knees for individuals who only received treatment on a single knee. The significance test for change from baseline is reported for WOMAC scores and for KPS-assessed scores of treated and untreated knees. Two-tailed p-value<0.05 was established as a statistical significance level.
Results
The recruitment and participation scheme is given in Figure 2. Thirty-eight (38) participants were enrolled. Two (2) participants withdrew consent after enrollment: 1 prior to injection due to scheduling difficulties and 1 after a single treatment session due to a herniated spinal disc unrelated to the study. Therefore, 36 participants were included in the analysis. Of these, 30 were recruited from community or outpatient clinics, and 6 from the former control groups of a prior prolotherapy RCT. The study sample (N=36; Table 1) consisted of white adults (60±SD 8.7 years old, range 46–71 years), the majority of whom were women (N=21) and who reported BMI over 25 kg/m2. The reported duration of knee pain was 81.2±SD 72.9 months (range: 3–360). Most participants had tried and failed one or more conservative measures. Thirty-one (31) radiographs were available for evaluation; 0 radiographs were available for 5 participants, and 1 for each of the remaining 31 participants.

Enrollment of participants and completion of the study. BMI, body–mass index; WOMAC, Western Ontario McMaster University Osteoarthritis Index; KPS, Knee Pain Scale.
Percentage does not add up to 100 due to participants' varied use of conventional therapies.
Existing knee radiographs were obtained for the more severely affected injected knee in each participant. Percentage does not add up to 100 due to missing data on five baseline knee radiographs.
SD, standard deviation; BMI, body–mass index; WOMAC, Western Ontario McMaster University Osteoarthritis Index; KPS, knee pain scale; OA, osteoarthritis.
Prolotherapy intervention
Thirty-six (36) participants received an average of 4.3±0.78 prolotherapy sessions; 22 participants had both knees treated, contributing 44 knees to the KPS analysis. Fourteen (14) participants had only one knee treated. The total sample size for the WOMAC and KPS analyses of treated knees was therefore 36 participants and 58 knees, respectively. The sample size of the KPS analysis of untreated knees was 14.
WOMAC
Repeated-measures analysis showed overall improvement in the total and subscale WOMAC scores (Table 2) during the study compared to baseline (p<0.001). The WOMAC scores progressively improved from baseline through 5, 9, and 12 weeks. Although a slight dip in the scores was noted at 24 weeks, they recovered by 52 weeks by which time participants reported a 36.1% (15.9±2.5 points) improvement in the overall WOMAC score (p<0.001). Covariate analysis showed that female gender (p=0.05), age (46–65 years old, p=0.04), and a BMI≤25 kg/m2 (p=0.04) were associated with greater improvement in WOMAC scores. Improvement in the WOMAC scores was not related to the participant recruitment source, number of received injection sessions, injection of one or both knees, duration of KOA pain, prior KOA therapies, tobacco use, or diabetes. Improvement in WOMAC scores at 52 weeks was also not associated with pretreatment Kellgren-Lawrence scores (18.7 point improvement for participants with Kellgren-Lawrence scores of 1–2 and 11.7-point improvement for participants with Kellgren-Lawrence scores of 3–4; p=0.09). The NNT to achieve the minimal clinical important difference of 12% 16 was 1.3; the NNT to achieve more robust overall improvements of 25% and 50% were 1.7 and 3.9, respectively. Thirty-eight percent (38%) of the participants achieved a 50% or greater improvement in the total WOMAC score at 52 weeks. The WOMAC score of 4 participants worsened over the 52-week study period, with no covariates being predictive. Qualitative comments revealed that three of these participants engaged in early strenuous physical activity after two or more prolotherapy treatment sessions. Overall, 15 participants reported engaging in strenuous physical activity earlier than recommended after clinical improvement at one or more points during the study.
Significance (p-value) is reported for overall treatment effect (repeated-measures model).
WOMAC, Western Ontario McMaster University Osteoarthritis Index; Wk, week; SE, standard error; NA, not applicable.
KPS
Similar to the WOMAC, KPS scores improved progressively through the 52-week study period (Table 3; p<0.001) in injected knees (n=58), regardless of the number of knees injected. Participants reported less severe baseline KOA pathology in uninjected knees (n=14) but interestingly, reported a statistically significant improvement in KPS scores even in the uninjected knees for both pain frequency (50%, p<0.001) and severity (43%, p=0.001) at 52 weeks (Table 3).
Results are presented as mean score (baseline) or mean score change (weeks 5–52) (standard error).
Twenty-two (22) participants had both knees treated (44 knees) and 14 participants had one knee treated (14 knees) for a total of 58 knees treated and 14 knees untreated.
Significance (p-value) is reported for overall treatment effect (repeated-measures model).
KPS, knee pain scale; Wk, week.
Procedure-related pain, satisfaction, and safety
As expected, all participants experienced self-limited postinjection pain, with 68% reporting oxycodone use prior to injections (“premedication”) and 45% reporting oxycodone use after the injections. Ninety percent (90%) of those using oxycodone reported that it substantially decreased procedure-related pain. Participants reported that procedural pain waned by the second day after injection, from 3.8±1.4 points to 3.1±1.4 points on the 1–7 ordinal response pain severity scale. One (1) participant experienced local numbness distal to the knee that spontaneously resolved in 2 hours. Twenty-nine (83%) participants reported that they would recommend prolotherapy to patients with similar KOA. There were no adverse events.
Discussion
This uncontrolled pilot study of participants with KOA found substantial, consistent improvement in knee pain, function, and stiffness at 52 weeks after treatment with prolotherapy. The 36% improvement on the validated WOMAC measure exceeded reported minimal clinical important difference of 12% 16 –25% 17 on the WOMAC; 38% of participants exceeded 50% improvement at 52 weeks. 21 While improvement was generally progressive over 52 weeks, there was a slight dip in scores in both the WOMAC and the KPS at 24 weeks, perhaps because some participants overused their knees following substantial improvement in knee pain at one or more time points in the study. These results may therefore underestimate the potential effect of prolotherapy in patients who adhere to recommendations for a gentle return to activity or sport following prolotherapy. These results provide level 3B evidence 22 that prolotherapy may be an effective treatment for pain and disability related to KOA.
Participants also reported significantly improved KPS scores on uninjected knees. This may represent a reduction in compensatory mechanisms of the uninjected side. Individuals with KOA have reduced knee and hip motion (i.e., angular velocity in the sagittal plane) on the affected side relative to controls, 23,24 thus placing additional burden on the unaffected limb when trying to maintain a given walking speed. 25,26 This may result in overuse, pain, and disability of the contralateral knee. Participants may have needed to compensate less on the uninjected side as a result of postinjection improvement of the primarily affected knee, sparing it from overuse and improving bilateral knee function. Overall, WOMAC and KPS data suggest that prolotherapy may improve upon standard of care for KOA, given that most participants were refractory to prior therapeutic measures. Such positive change may improve quality of life in the near term and delay progression of KOA in the long term. Clinical improvement may accrue preferentially to those who are of normal weight, female, and middle-aged.
These effects are consistent with another prolotherapy study, though comparison is limited by different injection protocols and outcome measures. 12 Direct comparison of these data to those in studies of hyaluronic acid injection and other conventional therapies is also difficult given the heterogeneity of reporting methods in many trials, but improvements of 20%–40% compared to baseline have been reported for conventional therapies and acupuncture. 4,8
Prolotherapy is an evolving modality gaining popularity in sport and family medicine, 11,27 though its mechanism of action is unclear. Dextrose injections have been hypothesized to stimulate healing of chronically injured extra-articular and intra-articular tissue 28 ; animal model studies reported increased inflammatory markers 29 and significantly enlarged cross-sectional area in medial collateral ligaments. 30 The potential of prolotherapy to stimulate release of growth factors favoring soft-tissue healing 12,31 and a positive neural effect have also been suggested. 32 Needle trauma and volume expansion of local tissue may also produce a tissue-level effect. 33 The combined effect of dextrose-specific effects, needle trauma, and volume expansion may explain positive results in this study. The source of pain in KOA is multifactorial. Prolotherapy injections target multiple potential nociceptors, including the relatively avascular articular cartilage and richly innervated intra-articular and extra-articular tissue including periosteum, periarticular ligaments, periarticular muscle, synovium, and joint capsule 6,34 and have been hypothesized to have intra-articular and extra-articular effects. 11,12,27
Limitations and Strengths
Limitations of this study include small sample size and lack of comparison group. The assessment of participant satisfaction was indirect and subject to bias. Radiographs were not available for all participants, and the use of Kellgren-Lawrence criteria for baseline radiological assessment of KOA severity is controversial, given that scores have not been uniformly correlated to patient-centered outcomes. The Kellgren-Lawrence score, however, is likely to remain an important measure for gauging disease severity in symptomatic patients. 35 The enrollment of 6 participants who had completed a prior prolotherapy trial may have introduced bias, though participant recruitment source was not a significant covariate. Strengths include pragmatic assessment using validated, patient-oriented outcomes and robust, consistent results with minimal missing data.
Directions for Future Research
Determination of clinical utility of prolotherapy for KOA will require assessment in a larger randomized multidisciplinary effectiveness trial that includes biomechanical and imaging outcome measures to assess for potential disease modification. 36,37
Conclusions
Prolotherapy resulted in safe, significant, and sustained improvement on validated pain, function, and stiffness measures in participants with KOA. Prolotherapy performed by an experienced operator may be an appropriate therapy for selected patients with moderate-to-severe KOA who are refractory to conservative care.
Footnotes
Acknowledgments
Grant support was provided by the National Institutes of Health, National Center for Complementary and Alternative Medicine grant number 5K23AT001879-02; and by the National Institutes of Health grant number K23AA017508-01A1.
Clinical Trials Identifier: NCT00085722.
Disclosure Statement
No competing financial interests exist.