
Abstract
Objectives:
The study objective was to evaluate the use of Danshen formulations in preventing renal disease in Henoch-Schönlein Purpura (HSP) either as sole agents or in combination with other drug regimens.
Methods:
Search strategy—Databases searched were the Cochrane Central Register of Controlled Trials, PubMed, Embase (Excerpta Medica Database), the Chinese Biomedicine Database, CNKI (Chinese National Knowledge Infrastructure), and VIP-database for all relevant studies without any language restriction. The cut-off date for the search was October 2010. Selection criteria—All randomized controlled trials with enrolled patients of all ages without renal disease before random assignment were included. The primary outcomes were the number of patients who developed renal disease and the incidence of adverse effects of drugs. Data collection and analysis—For dichotomous outcomes, the incidence of renal disease in patients with HSP was calculated as a relative risk with 95% confidence intervals. For continuous outcomes, the weighted mean difference with 95% confidence intervals was used.
Results:
A total of five trials (513 children aged 2–14 years old) were included in the meta-analyses, which indicated that Danshen formulations (injections or tablets) with symptomatic therapy significantly reduced the risk of developing renal disease in children with HSP compared to symptomatic therapy alone 6–12 months after treatment (relative risk: 0.35, 95% confidence interval: 0.20–0.61). Adverse effects of Danshen formulations were not explicitly reported in these studies.
Conclusions:
Danshen formulations may help prevent renal disease in children with HSP without serious side-effects. However, the evidence is of low quality (as assessed using the GRADE approach), and thus there is insufficient proof to strongly recommend the use of Danshen formulations in children with HSP. Large, properly randomized, placebo-controlled, double-blind studies are needed to substantiate its use.
Introduction
The common clinical manifestations of HSP are characterized by the triad of palpable purpura, abdominal pain, and arthritis, 6 and renal disease is the primary long-term and most serious complication. In a recent systematic review of 12 studies including 1133 unselected patients, renal disease occurred in 34.2% of patients; furthermore, renal complications developed in 85% of cases within 4 weeks of diagnosis, in 91% within 6 weeks, and in 97% within 6 months. 7
The prevention and treatment of renal disease in HSP is controversial. For example, one systematic review concluded that early corticosteroid treatment may reduce the risk of developing persistent renal abnormalities. 8 However, a recent Cochrane systematic review of four randomized controlled trials (RCTs) found no significant difference in the risk of persistent kidney disease at 6 and 12 months with prednisone administered at presentation compared to placebo. 9
In children with severe renal disease, treatment with conventional drugs (e.g., corticosteroids, cyclosporine A, and cyclophosphamide) alone or combined with other adjuvant treatment (e.g., immunoglobulin, anticoagulants, enzymes, and vitamins) have had variable success in improving renal outcomes, but their use is not adequately guided by evidence obtained from properly designed, randomized, placebo-controlled trials. 9 –11
The Chinese herb Danshen is the dried root of Salvia miltiorrhiza, which is used as a common adjuvant medicine for treating purpura, especially the Henoch-Schönlein type, in modern Chinese clinical practice. Many studies have suggested that treatment with Danshen formulations effectively prevents the development of renal disease 12,13 and/or reduces its severity 14,15 in patients with HSP. Furthermore, Danshen formulations may inhibit platelet aggregation, 16 improve renal microcirculation, 17,18 alleviate free-radical injury to the kidneys, 19 have anti-inflammatory properties, inhibit proliferation from mesangial cells, 20 and regulate abnormal immune function, 21 all of which are plausible mechanisms for renoprotective effects.
On the other hand, adverse effects of Danshen formulations, especially the injectable types, have emerged as a problem that must be addressed. Common side- effects include allergic reactions such as slight skin reactions and serious anaphylactic shock, 22,23 but no one knows whether children with HSP are more susceptible to these side-effects. Danshen formulations have been used for years to treat HSP in China; however, the effects and safety of the agent have not been systematically reviewed. The aims of this systematic review were to determine the effects of different Danshen formulations on renal disease in HSP patients, both as sole agents and in combination with other drug regimens.
Materials and Methods
Criteria for considering studies for this review
All RCTs evaluating the use of Danshen formulations (either as sole agents or in combination with other drug regimens compared to a placebo and other formulations or other drugs) for preventing the development of renal disease in patients of all ages with HSP were included. The term “Danshen formulation” was defined as a formulation containing only or mainly Salvia miltiorrhiza. The formulation had to be produced in certified Good Manufacturing Practice facilities of a pharmaceutical factory and in accordance with the guidelines of the State Food and Drug Administration of the Peoples Republic of China. The patients had to be free of renal disease before being randomly assigned, and studies including patients with HSP nephritis were excluded. The first period of randomized crossover studies was also included. The primary outcomes were the number of patients who developed renal disease (i.e., hematuria, proteinuria, nephrotic syndrome, hypertension, acute nephritis, renal dysfunction, need for dialysis or transplantation) and adverse effects.
Search methods for identification of studies
Six (6) electronic databases including the Cochrane Central Register of Controlled Trials (CENTRAL; The Cochrane Library, Issue 10 2010), PubMed (1966 to October 2010), Embase (Excerpta Medica Database) (1980 to October 2010), the Chinese Biomedicine Database (1976 to October 2010), CNKI (Chinese National Knowledge Infrastructure) (1979 to October 2010), and VIP-database (1989 to October 2010) were searched for all relevant studies without any language restriction. The PubMed search strategy was modified as required to search other databases, and the key words used were as follows:
Data collection and analysis
Titles and abstracts from the preliminary search results were independently checked by two authors (CZ and FHL) to identify clearly irrelevant studies that needed to be discarded. The full texts of the remaining studies were evaluated to judge whether the inclusion criteria were met. If key points were unclear, the original authors of the articles were consulted by telephone for clarification.
Data extraction
Data extraction was conducted on the full-text copies of all included trials, using data extraction forms especially designed for this purpose. Data regarding the characteristics of the study (i.e., sample size, age, disease period, and clinical features of patients with HSP) and the types and doses of different Danshen formulations, follow-up time, side-effects, primary outcomes (number of patients who developed renal disease), and the definition of renal disease were independently abstracted from the remaining articles by two authors (CZ and FHL). Disagreements were resolved by discussion and consensus mediated by a third author (XSL).
Quality assessment
The risk of bias in individual studies, assessed by the GRADE approach, was evaluated based on five factors: sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other potential biases. 25 The GRADE approach was used to evaluate the quality of evidence, and the results are summarized in a Summary of Findings Table. 26 The quality rating across studies assessed with the GRADE approach has four levels: high, moderate, low, or very low.
Data analysis
Review Manager 5 (Version 5.0.2) was used to analyze the results. For dichotomous outcomes, the incidence of renal disease was calculated in patients with HSP as a relative risk with 95% confidence intervals (CIs). For continuous outcomes, the weighed mean difference (WMD) was used with 95% CIs). The statistical test used for identifying heterogeneity across studies was the chi-squared (χ 2 ) test with Cochran's statistic Q, and the statistic I 2 was used to quantify inconsistency between studies. 27 For p values < 0.1 or > 0.1, a random effects model was used to calculate the summary statistics. In accordance with the authors' clinical experience, it was hypothesized that certain differences in the dosing route of Danshen formulations (e.g., oral or intravenous infusions) between studies would be closely related to the heterogeneity of treatment effects, so relevant subgroup analysis was attempted. Data were presented using GRADEProfiler 3.2.2 (GRADE Working Group 2004–2007), 28 and GRADE Quality Assessment Tables were constructed. Funnel plots were used if there were sufficient numbers of studies to include.
Results
Results of the search
Sixty (60) trials likely to be RCTs were identified by title or abstract review of 229 studies obtained from the electronic search. However, after full-text review, 55 of these trials were excluded because they were either false RCTs identified by querying the study authors via telephone (15 trials) or the studies enrolled patients with HSP nephritis before random allocation (39 trials). In addition, there was one duplicated study that was excluded.
Ultimately, a total of five trials 12,29 –32 involving 513 children (aged 2–14 years old) were included in this systematic review and analysis (Fig. 1). All of the studies were conducted in China and were published in Chinese.
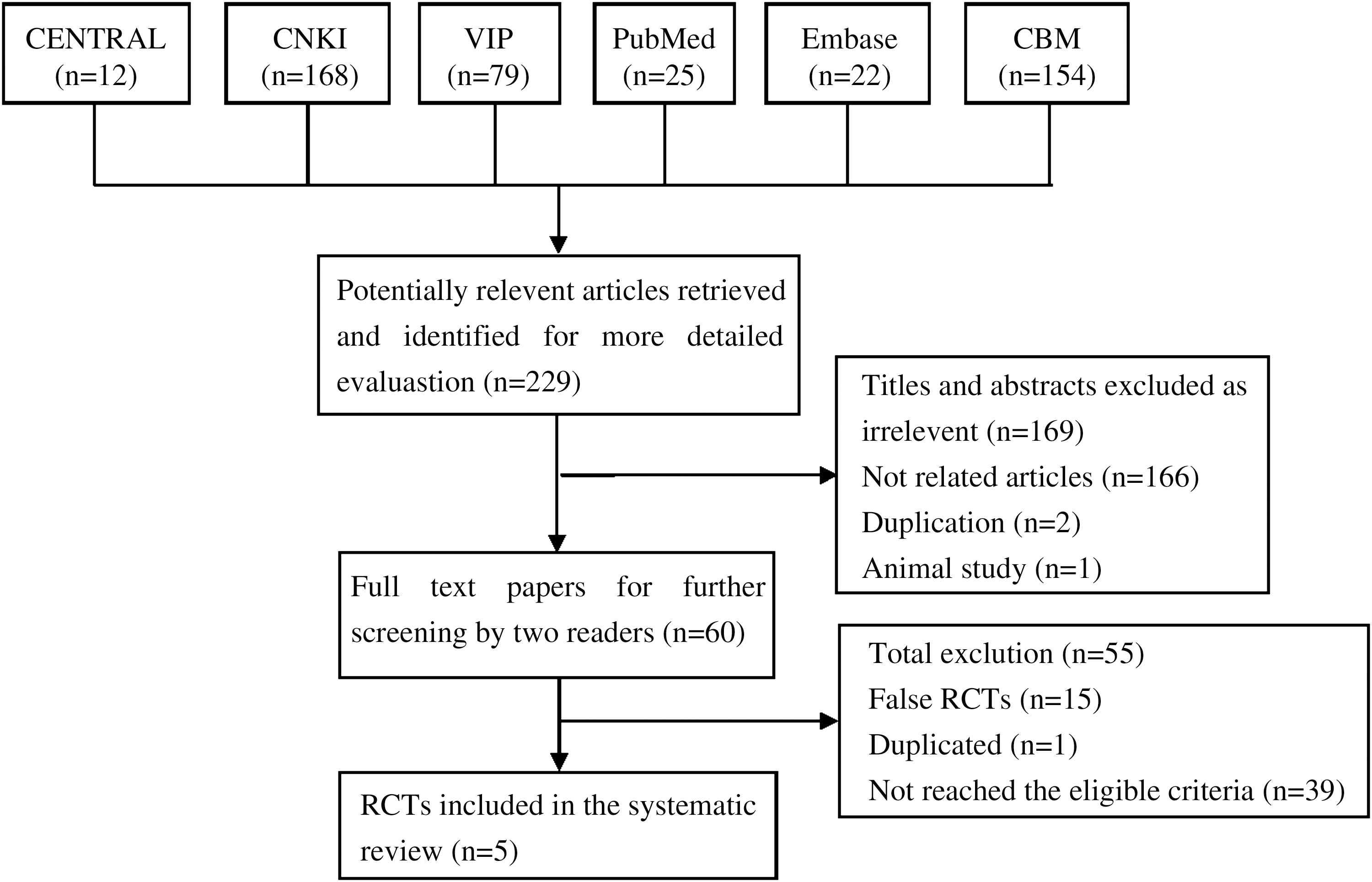
Results and process of the literature searches. CNKI, Chinese National Knowledge Infrastructure; VIP, China Scientific Journal database; CBM, China biological medical literature database; RCTs, randomized controlled trials.
Included studies
All of the trials compared the effect of Danshen formulations in combination with symptomatic treatment to that of symptomatic treatment alone (Table 1).
Hematuria/proteinuria: hematuria and/or proteinuria on dipstick.
Symptomatic treatment may include one or several kinds of the following treatment: antiallergic treatment (vitamin C, cimetidine, calcium agent, astemizole, etc.), antiplatelet treatment (rutin, dipyridamole, etc.), antibiotics treatment if infection existed, and glucocorticoid treatment if gastrointestinal symptom was severe.
T, treatment group; C, control group; S, skin type; J, joints type; G, gastrointestinal type; M, mixed type; GC, glucocorticoid; CDI, compound Danshen injection; FDT, Fufang Danshen tablets; UA, urinary albumin; UP, urinary protein; GFR, glomerular filtration rate; NS, not stated.
Two (2) types of Danshen formulations were used in the included studies, both of which are patented Chinese medicines. The first was Fufang Danshen in tablet form, also known as the original preparation of Compound Danshen Dropping Pills (a patented Chinese herbal medicine that has successfully completed Phase II clinical trials in the United States), which contains the same herbal ingredients (Salvia miltiorrhiza, Panax notoginseng, synthetic borneol, etc.). The second formulation was a compound Danshen injection made from the aqueous extracts of Danshen and Dalbergia odorifera. All of the formulations in the studies were administrated according to their instructions.
Two trials 30,32 (238 children) examined the effects of compound Danshen injection (0.5–1.0 mL/kg/day i.v.×2 weeks) on preventing renal disease in children with HSP 12 months after treatment. Two (2) trials 12,31 (187 children) evaluated the effects of sequential therapy of compound Danshen injection and Fufang Danshen tablets (injection 0.5–1.5 mL/kg/day i.v.×2 weeks, followed by 1–2 tablets 3 times/day×2 weeks) 12 months after treatment. One (1) trial 29 assessed the effects of Fufang Danshen tablets alone (1–2 tablets 3 times/day×3 months) 6 months after treatment. Glucocorticoids were not administered to either group in three of the trials, 12,31,32 while the other two did administer them. 29,30 One (1) trial 29 had a follow-up time of 6 months, while the other four trials 12,30 –32 had a follow-up of 12 months. Two (2) trials 31,32 used urinary dipstick proteinuria and hematuria as primary endpoints. In the remaining trials, 12,29,30 renal disease was defined by hematuria, proteinuria, 24-hour urine protein quantitation, and reduced renal function. Clinical presentation, kidney pathology, and prognosis of all of the children who developed renal disease were not described.
Risk of bias in included studies
All studies were of poor methodological quality and at high risk of bias (Table 2). “Randomly allocating the children” was mentioned by all five studies, but none of them described the methods used. After telephoning the study authors, it was determined that four studies 12,30 –32 used a random-number table, and the remaining study 29 used computer software.
Computer-generated sequence of random numbers.
All five studies did not provide any information about allocation concealment. After telephoning the study authors, it was established that none of the studies adopted an adequate allocation concealment method (investigators knew the intervention group before eligible children entered into the study).
Blinding of key study personnel (patients, investigators, assessors) was not used in any study. Dropouts or withdrawals were not reported in any study, and no trial reported an intention-to-treat analysis. Because the study protocols were not available, it was not possible to determine whether any of the studies' prespecified (primary and secondary) outcomes were reported in a prespecified way, so selective outcome reporting was possible, especially the side-effect reporting.
Effects of methods
Two studies 30, 32 (238 children) evaluated the difference in the risk of developing renal disease at 12 months between compound Danshen injections in combination with symptomatic therapy and symptomatic therapy only. The pooled analyses of these RCTs showed that compound Danshen injection with symptomatic therapy significantly reduced the risk of renal disease compared to symptomatic therapy alone (RR: 0.39, 95% CI: 0.17–0.85). There was no marked heterogeneity among the studies (p=0.87, I 2 =0%; Fig. 2).
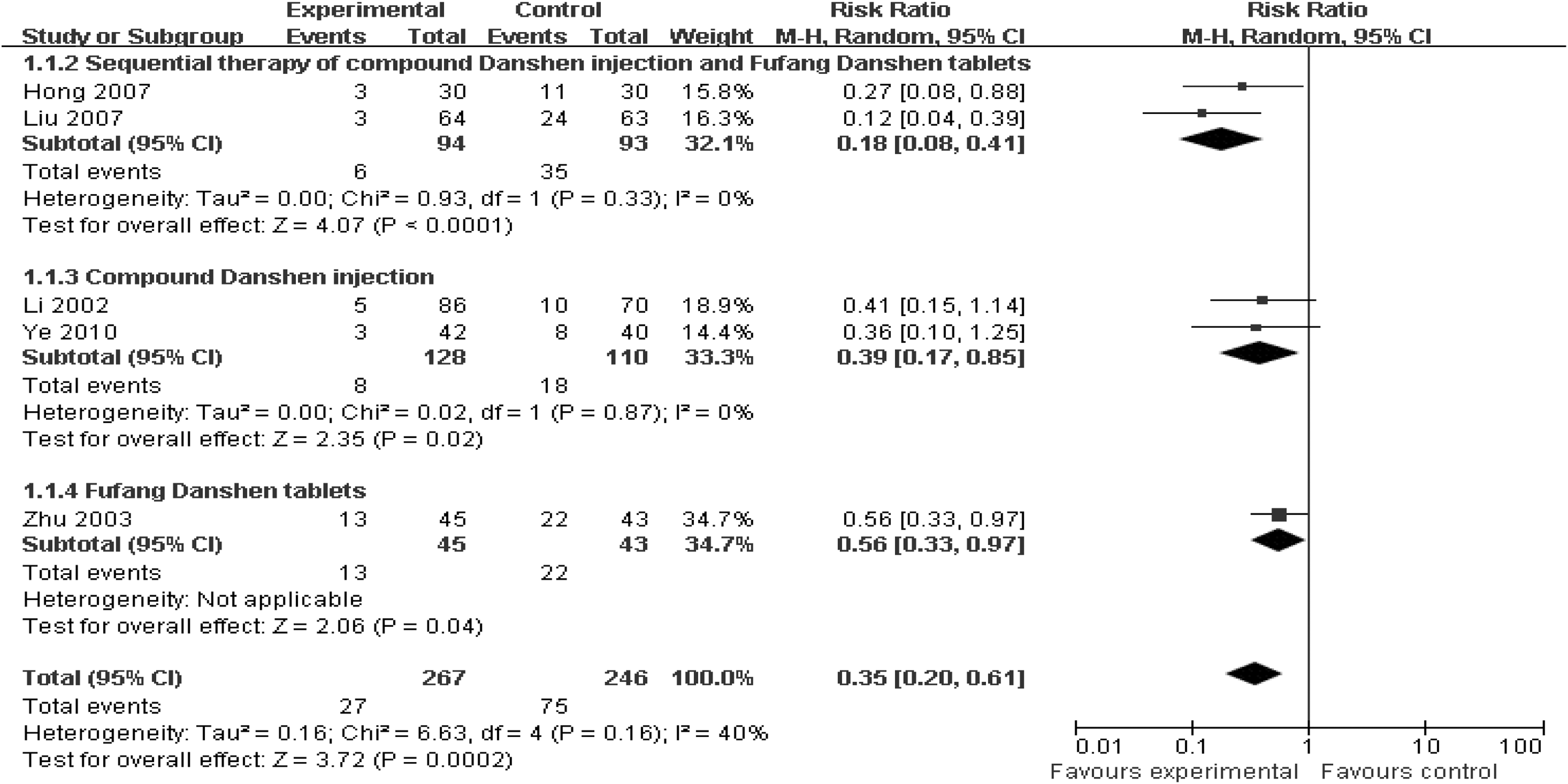
Forest plot of comparison: Danshen formulations in combination with symptomatic treatment versus symptomatic treatment. CI, confidence interval; M-H, Mantel-Haenazel test.
A pooled analysis of two trials 12,31 (187 children) showed a significant decrease in the risk of developing renal disease with sequential therapy (injection and tablets) and symptomatic therapy compared to symptomatic therapy alone (RR: 0.18, 95% CI: 0.08–0.41) at 12 months. There was no significant heterogeneity among the studies (p=0.33, I 2 =0%).
One (1) trial 29 (88 children) found that the risk of developing renal disease was significantly lower at 6 months with Fufang Danshen tablets compared to symptomatic therapy alone (RR: 0. 56, 95% CI: 0.33–0.97; Fig. 2).
Finally, all trials (513 children) were included in the meta-analyses, which indicated that Danshen formulations (injection or tablets) in combination with symptomatic therapy significantly reduced the risk of developing renal disease in children with HSP compared to symptomatic therapy alone beginning about 6–12 months after treatment (RR: 0.35, 95% CI: 0.20–0.61). There was no substantial heterogeneity among the five studies (p=0.16, I 2 =40%; Fig. 2).
One (1) trial 29 reported no adverse effects related to Danshen formulations; side- effects were not discussed in the other four trials. 12,30 –32
The substitution of a fixed-effects model for a random model did not change the initial qualitative interpretation of the pooled treatment effect on the risk reduction of renal disease.
Discussion
Summary of main results
The meta-analyses indicated that Danshen formulations (injection or tablet) in combination with symptomatic therapy significantly reduced the risk of developing renal disease in children with HSP compared to symptomatic therapy alone 6–12 months after treatment. Although adverse effects of Danshen formulations were not explicitly reported in these studies, there was no evidence to indicate that children with HSP were more vulnerable to allergic side effects related to Danshen compounds.
Quality of the evidence
All of the studies had a high risk of bias associated with an increased likelihood of results favoring the trial intervention. The following factors may have affected the results.
First, the methodological quality of the studies was poor. No articles described the procedure of randomization. Furthermore, allocation concealment and blinding (of patients, investigators, and/or outcome assessors) was not applied in any study (Table 2), and no study reported sample size calculation. These characteristics may lead to bias in selection, performance, and detection and may result in false-positive findings.
Second, although there was no significant inconsistency across the five trials in terms of the test for heterogeneity (p=0.16, I
2
=40%), three clinical factors that could have affected the results should be noted (Table 1). 1. The time period between HSP diagnosis and the start of each study was not clear in three studies,
29
–31
and was less than 14 days in the other two studies.
12,32
Any differences in the timeline would lead to different results, because risk of renal disease changes over time once HSP develops.
33
–35
2. In addition to inadequate blinding, renal outcomes were not defined consistently among the studies, which could readily lead to measurement bias. For example, three studies
30
–32
defined renal outcomes from urinary dipstick proteinuria and hematuria tested only once, while two studies
12,29
used a test with 24-hour urine protein quantitation, and renal function tests were conducted when the urinary dipstick test was abnormal. 3. The mode of delivery of Danshen formulations was not the same in the five studies. Two (2) studies
30,32
(238 children) evaluated the effect of compound Danshen injections, while one trial
29
(88 children) focused on the effect of Fufang Danshen tablets, and two trials
12,31
(187 children) studied the effect of sequential therapy (compound Danshen injection and Fufang Danshen tablets). Based on the current authors' clinical experience, it was concluded that the different dosings were closely related to the different treatment effects, so a relevant subgroup analysis was attempted. The analysis of each subgroup revealed a positive primary outcome, and the effect size of each was different, which verified the hypothesis of the current study.
Third, the CIs were generally wide in each trial, indicating imprecise results. For example, the narrowest CI 12 was 0.04–0.39 and the widest 30 was 0.10–1.25. The most plausible explanation for these wide CIs is that few children and few events were included in the studies, which would lower the quality of the evidence 25 (Fig. 2).
Fourth, unfortunately, all of the eligible studies were carried out in China and published in Chinese, and therefore positive results were more likely to be published than negative ones. 36 –38 Although a comprehensive search of journal and conference databases was conducted to ensure that all published and unpublished trials were identified, it was not possible to verify whether additional studies with negative findings remain unpublished. A funnel plot could not be used to investigate publication bias in this review because of the small number of studies.
For the above reasons (very serious limitations in design, serious imprecision, and high publication bias), the risk of bias for these trials is substantial, and the evidence rating by GRADE assessment was low (Table 3).
Allocation concealment and blinding (patients, investigators, or outcome assessors) was not used in any studies.
Only five trials were included, so there was high probability of publication bias.
Relative risk (RR)<0.5 (based on consistent evidence from five studies, with no plausible confounders).
CI, confidence interval; HSP, Henoch-Schönlein purpura.
Conclusions
Implications for systematic reviews and evaluations of health care
Based on the pooling results of the five RCTs, Danshen formulations may have a positive effect on preventing the development of renal disease in children with HSP. However, because of the low quality of evidence, future studies are necessary to confirm this hypothesis.
Implications for methodological research
It is hoped that future trials will avoid the limitations mentioned in this review that degrade the quality of evidence. In particular, they should pay more attention to the following key aspects of trials: randomization and allocation concealment procedures should be implemented strictly and described in detail, blinding of key personnel in trials should be used and specified, baseline characteristics of the patients should be described in detail, outcomes should be clearly defined, and the severity of the developed HSP nephritis should be analyzed quantitatively. Long-term follow-up is needed to evaluate the benefits and risks associated with Danshen formulations.
Footnotes
Acknowledgments
This work was supported by the Chinese Cochrane Centre, Chinese Evidence-Based Medicine Centre, INCLEN Resource and Training Centre, West China Hospital, Sichuan University, Chengdu, China.
Disclosure Statement
No competing financial interests exist.