
Abstract
Introduction:
Eating disorders commonly affect young girls and women. Four eating disorders are analyzed in this study: anorexia nervosa (AN), bulimia nervosa (BN), eating disorders not otherwise specified (EDNOS), and binge eating disorder (BED). Eating disorders are a modern concept and as such there is no critically appraised research on how Traditional Chinese Medicine (TCM) conceptualizes of or treats eating disorders. The purpose of this study is to identify and quantify the TCM patterns relevant to eating disorders based on a systematic evaluation of the results of a self-reported questionnaire.
Methods:
One hundred and ninety-six (196) female participants (142 with a self-reported eating disorder and 54 with no eating disorder) completed an online survey, designed to collect data on their current general health and, where relevant, their eating disorder. The Berle methodology was used to identify TCM patterns involved in eating disorders to tabulate and score the number of signs and symptoms experienced by the participants.
Results:
For many of the TCM patterns, statistically significant differences were found between presentation severity across the four eating disorders.
Conclusions:
For the first time, there is evidence-based research to classify the TCM patterns involved in AN, BN, EDNOS, and BED. Evidence is given to support the anecdotal theories of TCM patterns involved in eating disorder presentation. These results have relevance on how eating disorders are treated and viewed by TCM practitioners.
Introduction
Considerable research has addressed how an eating disorder progresses, how the categories of eating disorders are related, and the diagnostic criteria and subtyping for each eating disorder. 2,3 Currently, BED is a subcategory of EDNOS and it is defined as recurrent binging (excessive eating within a discrete time, e.g., 2 hours) at least twice a week, a feeling of being out of control while binging, feelings of guilt and self-disgust at binging, and no regular use of inappropriate compensatory behaviors. 1 However, recent research suggests that BED is a stand-alone eating disorder category having distinctively different psychopathology, development, course, and outcomes from other eating disorder groups. 4,5
Present research suggests that AN, BN, and EDNOS share similarities in psychopathology, development, and presentation.
4,6
The diagnostic criteria for AN consists of the refusal to maintain minimal healthy body weight, an intense fear of gaining weight, a distorted body image and, where relevant, amenorrhea.
1,7
The diagnostic criteria for BN is as for BED except there is the use of inappropriate measures to compensate for the binging (such as self-induced vomiting, fasting, excessive exercise, or misuse of laxatives, diuretics, and/or medications).
1
EDNOS is a category for disorders of eating that do not meet the criteria for any specific eating disorder. Examples of this include the following: • Meeting all the AN criteria except the minimal weight range or not being amenorrheic • Meeting all the BN criteria except for the frequency of binging or using inappropriate compensatory behaviors for eating “normal” amounts of food • Any other food-related maladaptive behavior that affects a person's self-worth (e.g., chewing food and spitting it out without swallowing
1
)
Figure 1 shows how the four eating disorders relate to each other.
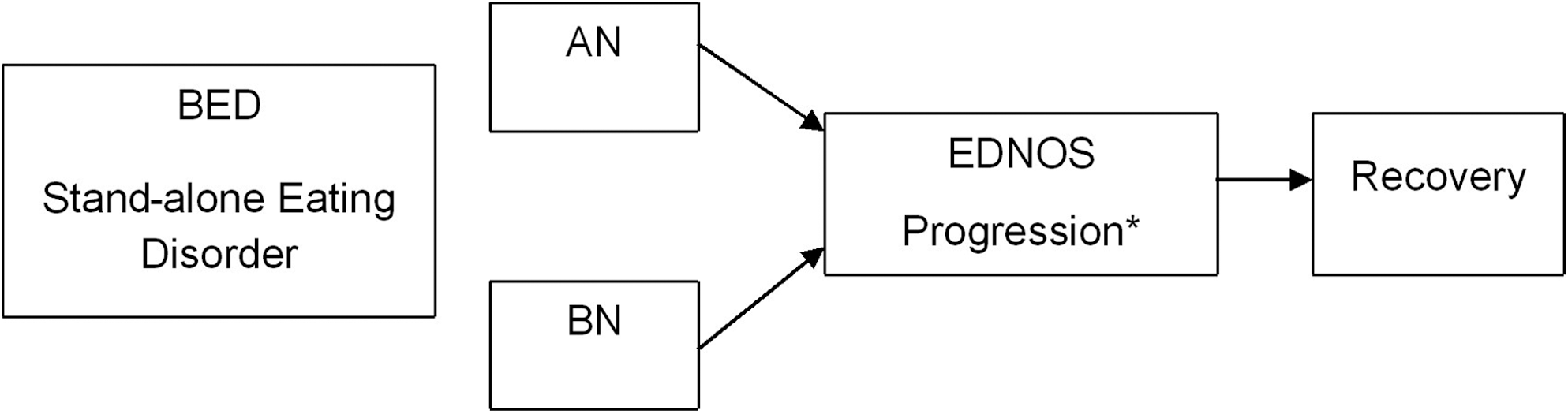
Understanding eating disorders. This flow chart explains how Western medicine understands eating disorders and their relationship to one another. BED, binge eating disorder; AN, anorexia nervosa; BN, bulimia nervosa; EDNOS, eating disorder not otherwise specified. *This process, although less common, can occur in the opposite direction from recovery (e.g., from “healthy” to having an eating disorder, either AN or BN).6
The current notion of eating disorders is a modern concept, and a literature search of the English research databases found no critically appraised research on how Traditional Chinese Medicine (TCM) conceives of or treats eating disorders. While ancient Chinese medical texts mention wasting away and not eating, 8 –10 the psychologic presentation (i.e., body dissatisfaction and drive for thinness) in eating disorders is vastly different from the TCM scenarios mentioned. As there is no conceptual understanding of eating disorders in TCM, there are no categories for the biomedical equivalent of BED, EDNOS, BN, or AN within TCM.
Despite the lack of critical evaluation of eating disorders in a rigorous scientific manner, there are widespread conceptual theories about how eating disorders can be defined within the TCM paradigm. These include the suggestion that eating disorders, particularly AN, are not autonomous illnesses and therefore no eating disorders should be categorized into specific TCM patterns. 11 In contrast, several TCM textbooks and anecdotal journal articles have attempted to identify possible TCM patterns of disharmony in those with an eating disorder. The TCM patterns suggested nearly always involve the Zang organs of the Spleen, Heart, and Liver 12,13, * despite there being no clinical research or case series to provide evidence that these organs and their respective patterns are seen specifically in people with an eating disorder.
Generally AN is presented as a deficient condition 14, † and BN as a Heat condition, 15, ‡ with authors failing to provide evidence to substantiate their diagnostic concepts. The poor and limited information on eating disorders available from TCM textbooks and related literature highlights the lack of understanding of eating disorders from a TCM perspective. The TCM patterns of disharmony that have been suggested as representing eating disorders are often listed generally under the umbrella term of “eating disorders,” and only a few authors separate the patterns according to AN or BN, while none address BED or EDNOS specifically. Recently, Berle et al. 16 have developed a TCM methodology that has the capacity, in part, to answer how TCM conceives of, and treats, eating disorders in terms of pattern identification in diagnosis and treatment prescription.
The purpose of the current research therefore was to identify and quantify the TCM patterns of disharmony relevant to eating orders by systematically evaluating the signs and symptoms reported by respondents who self-identified as having an eating disorder.
Materials and Methods
Survey participants were recruited via invitation. Several international and national eating disorder organizations and treatment clinics (Beating Eating Disorders UK, Eating Disorder Foundation of Victoria, Centre for Excellence for Eating Disorders) were contacted and an advertisement was inserted on their website, or the organization invited patients listed on their database to participate. Two hundred and ten (210) participants with a self-reported eating disorder completed the online survey. A similar method was used to recruit participants without an eating disorder who would be a comparator control group. Members of social clubs such as “Step into Life” and a “Skiing Club” resulted in 123 healthy noneating disorder participants completing the online survey.
The survey questionnaire included a list of signs and symptoms associated with eating disorders from a TCM perspective. In addition, questions on the individual's age and gender as well as questions on general health (e.g., sleep, menstruation, headaches, and so on) were included. Furthermore, relevant specific eating-disorder questions were included, which related to the Western medicine diagnosis and treatment of their eating disorder including specific signs and symptoms related to an eating disorder. The questionnaire was administered online via Survey Monkey.§ Prior to commencing the study, ethics approval was obtained from the Human Research Ethics Committee of Victoria University, HRETH07/241.
Of the total of 333 respondents, 132 were excluded because they completed less than half of the survey and 5 because they were male (137 in total), giving an effective response rate of 60%. Gender was not initially one of the exclusion criteria. However, only 1.5% of the respondents were males, and although males with eating disorders present similarly to females and there are some differences in depression and alcohol dependence, 17 it was therefore reasoned that there were too few male respondents to make interpretation of their data meaningful. The remaining 196 female respondents included 142 with an eating disorder and 54 without an eating disorder. Tables 1 and 2 show the characteristics of the 196 participants.
Also included, for those with an eating disorder (n=142), is their diagnosis, history, and length of time they have had their eating disorder and their treatment history.
BED, binge eating disorder; EDNOS, eating disorder not otherwise specified; BN, bulimia nervosa; AN, anorexia nervosa.
This study utilized a similar method reported by Berle et al. 16 for data collection and analysis. For a particular disease, the first step of this methodology involved reviewing the published literature to identify the various TCM patterns associated with that particular disease, and then collating the signs and symptoms that are associated with each of these patterns.
For eating disorders, a total of 21 TCM patterns were identified (Table 3). Signs and symptoms for each TCM pattern were then collated primarily from the World Health Organization standard terminology text 18 but also from Deng's diagnostic text 19 and Wiseman's Practical Dictionary 20 (Appendix 1). The process of determining the signs and symptoms for each pattern was as follows: The World Health Organization standard terminology text 18 was used as the master source of information. Deng and Wiseman were used as additional sources of information, and symptoms were added only after much consultation and debate by the authors. Berle et al. 16 was also used where patterns matched, to keep the continuity of this method and pattern identification. Tongue and pulse were excluded from the collated signs and symptoms due to the nature of the survey. It was impractical to ask participants not trained in tongue and pulse diagnosis to attempt this highly skilled task. For each TCM pattern, a checklist of these signs and symptoms was tabulated.
Each respondent was then required to indicate which of these tabulated signs and symptoms they experienced to ascertain the number of signs and symptoms present for each TCM pattern. Similarly to Berle et al.,
16
we define a Pattern Severity Index (PSI) according to the following formula:
Statistical analysis
The PSI data for each pattern is summarized as a mean and standard error for each of the 21 patterns of the four eating disorder categories and for those with no eating disorder. The PSI means were calculated using the statistical software EViews. 21
Further calculations made a comparison of the mean PSIs of those with an eating disorder and compared them to those with no eating disorder. For example, the PSI for those with no eating disorder was subtracted from the PSI means for BED, EDNOS, BN, and AN individually to report the difference from those without an eating disorder.
A regression model was computed to determine whether there was any significance between the means for each pattern of disharmony between the eating disorder subgroups. See Appendix 2 for model description.
A regression analysis was used to determine whether age, history of eating disorder, length of eating disorder, or eating disorder diagnosis had explanatory power for the PSIs for each pattern, controlling for eating disorder. Significance was determined as p<0.05.
Results
Table 4 shows the mean PSI scores for each of the patterns separately and for each of the four eating disorders and for those with no eating disorder. Statistically significant differences between the means for each pattern are represented by superscripts.
Means in the same row with different superscript are significantly different (p<0.05).
For those without an eating disorder, the most strongly expressed patterns were Liver Qi Depression and Spleen and Kidney Yang Deficiency, while for those with an eating disorder of any type, Liver Qi Depression, followed by Spleen and Stomach Deficiency Cold, were the two most strongly expressed TCM patterns.
Table 4 shows generally, but not uniformly, the trend for an increase in severity of symptoms from non–eating disorder to BED, to EDNOS, to BN, and finally AN, with AN ranking as the most severe eating disorder in 19 of 21 patterns. The two exceptions are Stomach Heat and Kidney Yang Deficiency, which are both most strongly expressed for BN.
For all 21 patterns listed, the mean PSIs for both AN and BN were significantly different from those with no eating disorder. For BED and EDNOS, there were, respectively, 11 and 16 patterns whose differences from no eating disorder were significant. In 10 of the 21 patterns, all four eating disorder severities were statistically significantly different from those without an eating disorder.
To determine those TCM patterns whose PSIs differ most between those respondents with and without an eating disorder, the mean PSI for those with the eating disorder of interest minus the mean PSI for those with no eating disorder were calculated. The top three patterns for which there are the largest differences in mean PSI scores from those with no eating disorder are: • AN: Spleen Qi deficiency, Spleen and Stomach Deficiency Cold, Heart Qi Deficiency • BN: Liver Qi Stagnation and Stomach Heat, Spleen Qi Xu, Heart Qi Deficiency • EDNOS: Spleen and Stomach Deficiency Cold, Liver Qi Stagnation and Stomach Heat, Spleen Qi Xu
• BED: Stomach Yin Xu, Liver Qi Depression, Heart Qi Deficiency
For each pattern, regression analysis showed that, once the type of eating disorder was controlled for, the PSI scores did not co-vary significantly with the participant's age, the duration of their eating disorder, the duration of their treatment, or whether their eating disorder was formally diagnosed.
Discussion
In TCM there exists a school of thought that suggests that eating disorders are not considered an autonomous illness. 11 This study has demonstrated significant differences in severity presentation between those with and without an eating disorder, particularly in AN and BN, suggesting that eating disorders can be identified as separate autonomous TCM syndromes.
The present study highlighted that both Liver Qi Depression and Spleen and Stomach Cold Deficiency were found to be strongly exhibited by sufferers of eating disorders of any type (the two most strongly expressed TCM patterns in all four of the eating disorder categories). Although Liver Qi Stagnation is intermittently mentioned as being involved in eating disorder presentation, 12, * Spleen and Stomach Cold Deficiency has certainly not, to our knowledge, been mentioned prior to this research. Further investigation into why the two abovementioned patterns present so strongly in those with an eating disorder of any type may help to provide more effective treatments and a better understanding of the causes, pathogenesis, and evolution of an eating disorder from a TCM perspective.
Specifically with the subcategories of an eating disorder, AN and BN present extremely similarly, but what seems to differentiate AN from BN is the ordering of the patterns that differ most from those with no eating disorder.
AN has a stronger representation of Spleen and Stomach and Deficiency patterns, suggesting that the Spleen and Stomach patterns play an important differential role in AN presentation. In BN, however, there is a greater prominence of Stomach Heat and Liver Qi Stagnation patterns in addition to the familiar Spleen and Stomach patterns. This implies that the pattern of Liver Qi Stagnation has a more differential role in the presentation of BN than in AN. This understanding of the intricacies of presentation of the TCM patterns seen in AN and BN may help practitioners refine their treatment of AN and BN and increase the effectiveness of their treatment.
Spleen Qi Deficiency and Heart Qi Deficiency have been identified by anecdotal evidence as TCM patterns being involved in those with AN.* The findings of the current study comparing those without an eating disorder to those with AN provide some preliminary evidence that both of these patterns are involved. Spleen and Stomach Deficiency Cold, however, is not mentioned as being involved in AN, and perhaps the addition of some warming treatment approaches such as moxibustion of warming herbal formulas that focus on both Spleen Qi Deficiency and Spleen and Stomach Deficiency Cold would yield more efficacious results than treating Spleen Qi Deficiency alone.
Stomach Heat has been put forward as a presenting pattern in BN in many texts 15, † and until this time, the evidence for the inclusion or presentation of Stomach Heat has again been anecdotal. The current study provides evidence to partially support this theory, suggesting that Stomach Heat in combination with Liver Qi Stagnation is a better representation of BN presentation than Stomach Heat alone. A treatment protocol that addresses Stomach Heat and Liver Qi Stagnation may therefore provide more efficacious results than treating Stomach Heat alone.
Based on the evidence that compared AN, BN, and EDNOS to those with no eating disorder, this study supports the theory that EDNOS is a progression from either AN or BN. The four patterns that present with the strongest differences in EDNOS are a combination of the top three patterns in both AN and BN (e.g., Spleen and Stomach Cold Deficiency, Liver Qi Stagnation and Stomach Heat, Spleen Qi Deficiency and Heart Qi Deficiency). Relapses back into full-blown BN or AN from EDNOS are common in the treatment of eating disorders, 22 and TCM practitioners using the differential findings mentioned above may be able to better understand AN, BN, and EDNOS and where appropriate help to maintain recovery and to help prevent relapses.
Compared to those with no eating disorder, BED presents very differently from those with EDNOS, BN, and AN. Again, this study's findings support the Western medicine theory that BED is a separate and stand-alone eating disorder category. An overview of the BED patterns with the greatest variation from those with no eating disorder show a predilection for patterns involving both Heat and Full conditions (Full and Empty Heat conditions and Stagnation). This is in stark contrast to the overview of EDNOS, BN, and AN, which have a stronger representation of Deficiency and Cold patterns, especially involving the Spleen, Stomach, and Heart and Cold Deficiency. This implies that BED needs to be treated and understood as being a separate syndrome from EDNOS, BN, and AN.
One limitation of self-reported surveys is that some respondents may have under- or over-reported their symptoms. Furthermore, due to individual interpretation of some of the signs seen in the patterns (e.g., pale face) and the Chinese expression of symptoms (e.g., scorched lips), the survey may not have captured all relevant data for each respondent. Additionally, a limitation specific to online surveys is the possibility of multiple responses from a single individual, and this cannot be ruled out in the present study. There is much debate about the signs and symptoms delineated in TCM patterns of disharmony. The process used in this study is based on that of Berle et al., 16 who were pioneers of this concept. Future research into TCM patterns of disharmony standardization could help refine this process. Finally, the issue surrounding cross-validation and reliability of the current survey in different patient cohorts and settings is beyond the scope of the current project.
Conclusions
This study addresses the paucity of information regarding TCM pattern presentation and understanding of eating disorders, specifically the conditions of AN, BN, EDNOS, and BED. It demonstrates that for the TCM patterns, statistically significant differences exist between presentation severity across the four eating disorders. This implies that eating disorders can be identified as a separate, autonomous syndrome in TCM. The results also provide evidence-based findings on the TCM patterns involved in eating disorder presentation, supporting the anecdotal evidence. Liver Qi Depression and Spleen and Stomach Cold Deficiency were found to be strongly expressed by those with an eating disorder of any type. Compared to those with no eating disorder, the TCM patterns Spleen Qi Deficiency, Liver Qi Stagnation, and Stomach Heat, Spleen, and Stomach Cold Deficiency and Heart Qi Deficiency feature strongly in AN, BN, and EDNOS. In contrast, Stomach Yin Deficiency, Liver Qi Depression, and Heart Qi Deficiency feature strongly in BED. These results have the potential to impact how eating disorders are understood, viewed, and treated by TCM practitioners. With the identification of TCM patterns involved in the four eating disorder categories and the proposed treatment approach, it is expected that TCM practitioners will be able to understand and treat eating disorders more effectively. Future research to evaluate these results and their role in directing acupuncture and Chinese herbal treatment is warranted.
Footnotes
Acknowledgments
We wish to thank all organizations, but particularly the Beat Organization (Beat Eating Disorders UK) for their help in recruiting participants for the survey.
Disclosure Statement
No competing financial interests exist.
| Heart Blood Deficiency | Heart Yin Deficiency | Heart Qi Deficiency | Heart Yang Deficiency | Phlegm clouding the Heart Spirit | Food damage | Heat harassing Heart Spirit |
|---|---|---|---|---|---|---|
| • Palpitations • Insomnia • Dizziness • Forgetfulness • Pale nails • Dream disturbed sleep • Pale or sallow complexion • Pale lips |
• Mental irritability • Palpations/fearful throbbing • Insomnia • Low fever • Night sweating • Warm palms and soles of feet • Thirst • Profuse dreaming • Dry lips and throat • Bitter taste in the mouth • Constipation • Yellow urine |
• Palpitations • Easily frightened • Shortness of breath • Difficulty falling asleep • Listlessness • Forgetfulness • Spontaneous sweating • Pallor • Lack of strength |
• Palpitations • Tendency to be easily frightened • Dyspnea • A feeling of pressure in the chest • Difficulty falling asleep despite desire to sleep • Forgetfulness • Aversion to cold • Spontaneous sweating • Cold limbs • Fatigued spirit • Lack of strength • Shortage of qi • Laziness in speaking • Bright pale complexion |
• Impairment of consciousness • Psychotic depression or coma • Phlegmatic sound in the throat |
• Sour and rotten vomit • Distension and fullness of the abdomen • Rotten and malodorous belching • Aversion to food • Abdominal pain • Intestinal rumbling • Diarrhea • Diminishing of abdominal pain after discharge, then return of pain • Rotten and malodorous fecal matter |
• Fever • Thirst • Vexation • Insomnia • Manic or delirious speech • Flushed face • Constipation • Dark-colored urine |
| Food accumulation | Stomach Heat | Stomach Yin Deficiency | Stomach Qi Deficiency | Spleen & Stomach Deficiency Cold | Stomach–Spleen disharmony | Spleen Qi Deficiency | Spleen Yang Deficiency |
|---|---|---|---|---|---|---|---|
| • Glomus oppression in the chest and stomach duct or hardness with glomus lumps • Acid regurgitation • Abdominal pain that is worse with pressure • Constipation • Torpid intake • Reduced appetite • Rotten belching |
• Thirst • Foul breath • Hyperorexia • Oliguria with dark urine • Constipation • Ulceration of the mouth or gingivitis • Scorching pain of the stomach that refuses pressure • Preference for cold fluids • Acid up flow • Rapid hungering • Swelling and pain of the teeth • Scorched lips |
• Dry mouth • Thirst • Anorexia (lack of appetite) • Constipation • Retching • No intake of food or swift digestion with increased appetite • Scorching pains of the stomach duct • Hiccoughs • No desire to eat even when hungry • Possible wasting thirst • Dysphagia |
• Dull epigastric pain relieved by pressure • Anorexia • Torpid intake • Tastelessness of food • Distension and fullness of the stomach • Nausea • Vomiting • Belching • Hiccough |
• Colds and pains over the stomach • Cold limbs • Chronic diarrhea • Abdominal fullness • Belching • Vomiting thin fluid • Lassitude • Anorexia |
• Epigastric stuffiness and distension • Anorexia • Fatigue • Sloppy stool • Abdominal distension after eating • Lack of strength • Belching • Borborygmi • Shortage of qi • Torpid intake • Laziness in speaking |
• Dizziness • Reduced food intake • Fatigue • Fatigued limbs • Sallow face • Indigestion • Abdominal distension • Lassitude • Anorexia • Loose bowels • Shortage of qi • Laziness in speaking |
• Cold limbs • Emaciation • Coldness and pain in the abdomen • Edema • Anorexia • Abdominal distension • Abdominal fullness • Aversion to cold • Chronic diarrhea • No thirst • Lassitude • Torpid intake |
| Spleen and Kidney Yang Deficiency | Kidney Yang Deficiency | Kidney Yin Deficiency with fire effulgence | Liver Qi Stagnation and Stomach Heat | Liver Fire flaming upwards | Liver Qi Depression | Liver Qi invading the Stomach |
|---|---|---|---|---|---|---|
| • Bright white facial color • Fifth watch diarrhea/chronic diarrhea • Physical cold (aversion to cold) • Swollen limbs • Cold limbs • Coldness and pain in the loins and lower abdomen • Bland taste in the mouth • Lack of thirst • Torpid intake • Diminished appetite • Abdominal distension after eating • Head dizziness • Ringing in the ears • Cold pain of the lumbus and knees • Inhibited urination |
• Aversion to cold • Tinnitus • Cold limb • Dizziness • Listlessness • Lack of strength • Weakness and soreness of the loins and knees • Predilection for sleep • Premature ejaculation or impotence/ frigidity/infertility • Nocturia |
• Tidal fever • Tinnitus • Night sweating • Flushed checks • Vexing heat in the chest, palms and soles • Nocturnal emission • Premature ejaculation • Hypersexuality • Lumbar pain |
• Vomiting sour fluid • Torpid stagnant stomach intake • Stomach duct pain • Aversion to food • Abdominal distension • Diarrhea • Dizziness |
• Distension, pain and burning sensation in hypochondriac region • Irritability • Hot red face • Difficulty sleeping • Red eyes • Constipation • Irascibility (easily angered) • Bitterness and dryness in the mouth • Headache • Dark urination |
• Depression • Frequent sighing • Hypochondriac or lower abdominal distension or moving pain • Feeling of foreign body in the throat • Distending pain of the breast • Irregular menstruation/ abdominal pain prior to menstruation/ Premenstrual syndrome • Agitation/irascibility • Flatulence/bloating |
• Hypochondriac pain • Irritability • Epigastric distension • Epigastric pain • Anorexia • Belching • Nausea • Vomiting • Torbid intake • Dizziness |
Appendix 2. The Regression Model Was Used to Determine Whether There Was Any Significance Between the Means for Each Pattern of Disharmony Between the Eating Disorder Subgroups
The model was
where PSI i is the Pattern Severity Index (PSI) score for individual i for a particular pattern of disharmony and BED i , EDNOS i , BN i , and AN i are indicator variables for the eating disorder (BED=binge eating disorder; EDNOS=eating disorder not otherwise specified; BN=bulimia nervosa; AN=anorexia nervosa). The coefficients in the regression model have the simple interpretations:
β1 is the average PSI i for those with BED,
β2 is the average PSI i for those with EDNOS,
β3 is the average PSI i for those with BN,
β4 is the average PSI i for those with AN.
If any of the coefficients are equal, then the regression model was simplified. For example, if β1=β2, then the model simplifies to
This would imply that individuals with BED and EDNOS have the same average PSIs, while those with BN and AN have different PSIs.
There are 52 possible patterns of equality in the coefficients. Each of the 52 implied regression models was estimated, and the preferred model was chosen to be the one with the optimal HQ (Hannan-Quinn) criterion. This criterion provides the best trade-off between goodness of fit and model simplicity (a model with fewer coefficients is simpler).
For example, the best regression for Stomach Heat was found to be β1≠β2=β3≠β4. The implication is that the average PSI for Stomach Heat does not differ significantly between EDNOS and BN, nor do the PSIs differ between BED and AN, but the differences between the pairs BED, EDNOS and BN, AN are significant.
*
Deadman P. Eating disorders. Personal communication. E-mail, 2007:1; Eating Disorder Resource Centre of BC. Eating disorders and body image, 2006; Fletcher M. Fight eating disorders with Chinese medicine. Pacific College of Oriental Medicine, 2002–2005:2; Mahoney H. Sexual abuse/incest and the resulting patterns of energetic disharmony in the young female: Can Traditional Chinese Medicine play a role in understanding these patterns? Australian Acupuncture College of Melbourne, 1989; Munir NE. Anorexia and bulimia: Healing Centre, An alternative healing method, 2007; Scott J. Eating disorders. Personal communication. UK, 2007:1.
†
Eating Disorder Resource Centre of BC. Eating disorders and body image, 2006; Fletcher M. Fight eating disorders with Chinese medicine. Pacific College of Oriental Medicine, 2002–2005:2; Munir NE. Anorexia and bulimia: Healing Centre, An alternative healing method, 2007; Wimmer R. Treating the female athlete triad: Eating disorders, Part one. Acupuncture Today, 2003:2; Smith RD, Acupuncture Colleges (Australia). Anorexia nervosa: west meets east a study of collateral damage, 1993.
‡
Flaws B. Bulimia and Chinese Medicine. Blue Poppy Press, 2001; Wimmer R. Treating the Female Athlete Triad: Eating Disorders, Part One: Acupuncture Today, 2003:2.
§
*
Deadman P. Eating disorders. Personal communication. E-mail, 2007:1; Eating Disorder Resource Centre of BC. Eating disorders and body image, 2006; Fletcher M. Fight eating disorders with Chinese medicine. Pacific College of Oriental Medicine, 2002–2005:2; Munir NE. Anorexia and bulimia: Healing Centre, An alternative healing method, 2007; Scott J. Eating disorders. Personal communication. UK, 2007:1.
*
Deadman P. Eating disorders. Personal communication. E-mail, 2007:1; Eating Disorder Resource Centre of BC. Eating disorders and body image, 2006; Fletcher M. Fight eating disorders with Chinese medicine. Pacific College of Oriental Medicine, 2002–2005:2, Mahoney H. Sexual abuse/incest and the resulting patterns of energetic disharmony in the young female: Can Traditional Chinese Medicine play a role in understanding these patterns? Australian Acupuncture College of Melbourne, 1989; Munir NE. Anorexia and bulimia: Healing Centre, An alternative healing method, 2007; Scott J. Eating disorders, Personal communication, UK, 2007:1.
†
Flaws B. Bulimia and Chinese medicine, Blue Poppy Press, 2001; Fletcher M. Fight eating disorders with Chinese medicine. Pacific College of Oriental Medicine, 2002–2005:2; Munir NE. Anorexia and bulimia: Healing Centre, an alternative healing method, 2007; Wimmer R. Treating the female athlete triad: Eating disorders, part one. Acupuncture Today, 2003:2.