
Abstract
Background:
Over 40% of children with cancer have reported that chemotherapy-induced nausea and vomiting (CINV) are the two most distressing side-effects of treatment even when antiemetic drugs have been used.
Objectives:
The purpose of this article is to report the findings from a feasibility and pilot study using auricular point acupressure point for CINV in a small group of children in Taiwan.
Methods:
This was a crossover randomized design study. CINV symptoms were assessed on 10 patients just prior to and for 7 days following each of three rounds of chemotherapy drugs (CTX). They received standard care (SC) and were not entered into a test treatment group until they completed the baseline assessment, which was conducted during their first round of chemotherapy after entering the study. Just prior to receiving the second round of CTX, patients were randomized into one of two treatment conditions: auricular acupressure intervention, in addition to standard care (AAP) or auricular acupressure using sham auricular points (SAP) in addition to standard care. For the third round of CTX, they were switched to the other treatment group.
Results:
The enrollment rate for this study was 77% of the children invited to participate and of those, 88% provided completed data sets for all three treatment conditions. Patients in the AAP group reported significantly lower occurrence and severity of nausea and vomiting than patients in the SC group (p<0.05). There were no significant differences of nausea and vomiting for patients between the AAP and SAP groups. All of the patients took antiemetic medication on the day they received CTX, and 80% of patients reported that the antiemetics did not help to treat CINV.
Conclusions:
These preliminary findings did show evidence that AAP is acceptable to the children and their parents to prevent/treat CINV. However, there were no statistically significant differences between the AAP and SAP groups in the prevention/treatment of CINV. There were clinical trend differences between the groups, which may due to the small sample size. In a larger study, it would be important to determine whether the effects of the AAP and SAP treatment are independent of any psychologic effects, such as the researcher's increased presence in both treatment groups.
Introduction
Auricular therapy, along with acupoints in other body parts, is a well-established treatment strategy in Traditional Chinese Medicine (TCM). Auricular therapy, as proposed by Dr. Nogier, a well-known French neurosurgeon, is based on the understanding that the ear represents a simulation of an inverted fetus within the womb and therefore provides acupressure points corresponding to all parts of the human body, including the internal organs. 13,14
In TCM, a disease is viewed as being caused by the imbalance of a person's energy, or qi. 15 Qi is the basal energy of the body that flows through the entire body and is the basis for all movement and action. 15 When acupoints are pressed, the stimulation regulates qi, activates meridians and collaterals, balances the yin and yang, and is thus suitable for treating health problems and restoring health. 15
Study Purpose
The aims of this study were to (1) examine the feasibility of recruiting children with cancer into a future larger study for the auricular acupressure point (AAP) to prevent/treat CINV, (2) evaluate the feasibility of performing the research procedures, and (3) determine whether there is preliminary evidence to suggest that the experimental AAP treatment is more effective than the placebo SAP and standard care for CINV.
Methods
This was a crossover, randomized design feasibility study. Subjects were entered into the study for three successive rounds of chemotherapy. CINV data from the next round of chemotherapy after being entered into the study (“study round 1”) was used as the standard care (SC) group and provided baseline data. Prior to “study round 2,” subjects were randomized into two treatment conditions: (1) auricular acupressure intervention, in addition to standard care (AAP); and (2) auricular acupressure using sham points in addition to standard care (SAP). For “study round 3,” the groups were crossed over to the other treatment condition.
Subjects
Patients were eligible for this study if (1) they were between 5 and 18 years; (2) were diagnosed with cancer and had at least one round of chemotherapy treatment; (3) were prescribed chemotherapy drugs (CTX) with high or moderate level emetogenic potential chemotherapy agents; 16 (4) were prescribed standard antiemetics with their CTX; and (5) had not previously received any acupuncture or acupressure treatments in the previous 3 months. The number of days in a round of CTX varied from 1 to 5 days. Each course had a 2- to 4-week interval. The standard emetics prescribed by the physicians included 5-hydroxytryptamine 3 (5-HT3) receptor antagonists such as ondansetron (Zofran), granisetron (Kytril), or a corticosteroid (dexamethasone).
Intervention
During the application of the seeds (usually less than 5 minutes) patients were asked to stay silent, sitting in comfortable chairs/bed. The outer ear including the earlobe was cleaned with 75% alcohol before the small pieces of adhesive tape with two seeds were taped onto each selected auricular point. The auricular (outer ear) points selection for the AAP group were those specific for nausea and vomiting according to Dr. Huang's ear reflex theory. 13,15 Five (5) reflex points (shenmen, sympathetic, cardia, stomach, digestive subcortex) (digestive subcortex was used to treat diseases of digestive systems, located at the center of the lower half of the interior antitragus) (p. 196) 15 were used in intervention (Fig. 1). The placebo group received acupressure treatment on the following auricular (outer ear) acupoints (which refer to the external knee point, vision, shoulder joint, and eye), 15 which are not related to CINV (Fig. 1). The auricular electrical finder was used to locate the acupoints with disorder. The sounds of the positive reaction from the auricular electrical finder, the change color, and shape of the acupoints were used to determine the auricular location. After the acupoints were found, the therapist confirmed the acupoints of the corresponding part of the body with the patient. The tapes with the seeds were carefully placed on the right acupoints. Then, the auricular therapist demonstrated the pressing technique to patients and parents before asking them to do a return demonstration. They were instructed to apply moderate stimulation by pressing slightly to more firmly until patients felt either mild discomfort or tingling. Bilateral auricular (both earlobes) points were used for treatment. Each patient was asked to press the acupoints by themselves at least 3 times a day for at least 3 periods of 3-minute duration each day, even if they did not have symptoms. They were also instructed to press the seeds as soon as they felt nausea, preferably before they were going to vomit. Seeds were kept on auricular points for 7 days. Patients and parents were instructed to remove them after the treatment ended. All of the treatments were conducted by the same therapist.
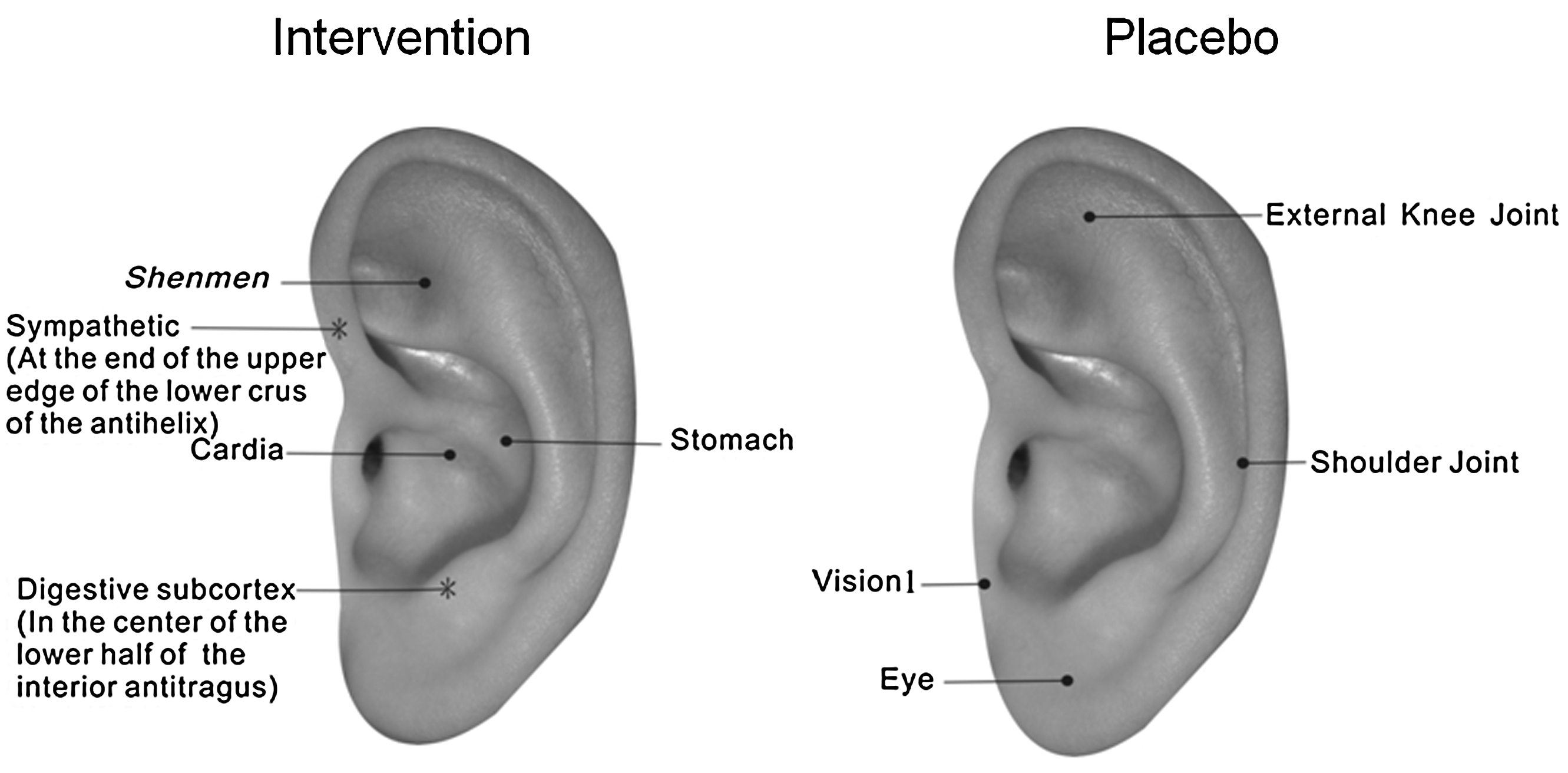
Auricular acupoints for chemotherapy-induced nausea and vomiting treatment.
Measures
Morrow Assessment of Nausea and Emetics 17
Morrow Assessment of Nausea and Emetics, a self-report questionnaire, was developed in adults used to measure occurrence (yes or no), duration (how many hours), and severity (score 1–6) after the beginning of chemotherapy, as well as the use of antiemetic and the effects. The duration of nausea and vomiting that was present could thus be quantified. It was a 17-item questionnaire with good internal consistency, test–retest reliability, and concurrent validity. 17 It was modified and adapted for use by children. In this study, the score of severity was recorded as “slight,” “moderate,” and “severe,” and the score of antiemetics effects was recorded as “did not help” and “provided relief.”
Demographic information
Demographic and relevant data were collected from medical records and included age, gender, cancer diagnosis, and treatment information. Chemotherapeutic agents, and the antiemetics used during data collection were also recorded.
Study booklet
Each child subject and their parent received a booklet including information about the acupressure technique (including intensity and duration). Patients/parents were asked to keep a diary of stimulation times (frequency), the number of acupoints stimulated and stimulation duration at each of the acupoints, and whether or not the child felt relief from the symptoms they were experiencing.
Procedures
The study began after receiving approval from the Human Subjects Review Committee for the study setting. Subjects were recruited from a large children's hospital in Taiwan. The hospital's established procedures for protecting confidentiality were strictly followed. Following the institutional review board's guidelines, potential subjects and their parent(s) were approached by a familiar member of the clinical team to provide introductory information about the study and determine their willingness to meet with a member of the research team. After consent and assent forms were signed, baseline data were collected during the next new round of chemotherapy as the standard care data (SC). Then, patients were randomized to one of the two groups: AAP or SAP, using a computer-generated randomization table, as outlined in the study flow chart in Figure 2. After the completion of the first intervention, patients were switched to AAP or SAP. The duration for two interventions ranged from 2 weeks to 1 month, depending on the chemotherapy protocol. For the first treatment, it took 20–30 minutes to complete the study, and 5–10 minutes for the follow-up treatment. Patients received standard antiemetic medications as prescribed by their clinical team. For each round, data were collected prior to chemotherapy administration and then daily for 7 days after the tapes had been placed onto the earlobes.

Flow chart of patient recruitment.
Statistical Analyses
Descriptive statistics were estimated for the demographic characteristics of the participants. The intervention effect of treatments during the seven-time postchemotherapy assessment points were analyzed using the generalized linear model 18 with the generalized estimated equation for longitudinal categorical measurements 19 (i.e., occurrence, severity, and effects of medication), and a mixed-effects model 20 was used for longitudinal continuous measurements (i.e., duration of nausea and vomiting). The model included fixed effects for group (i.e., AAP, SAP, and SC) and time. Model effects were tested at a significance level of 0.05. The post-hoc test was used to do multiple comparisons among SC, AAP, and SAP groups. All of the data analyses were performed using SAS software, version 9.2. 21
Results
Demographic findings
Patients (n=10) who enrolled in the study were all able to complete the study for baseline assessment and postchemotherapy test points. Patients included 6 boys and 4 girls; 4 had been diagnosed within the last 3 months, 2 were in remission but continuing on-treatment; and 4 had relapsed and were on-treatment. The mean age of the patients was 13.29 years (range 6–18, standard deviation [SD]=3.31 years). The mean duration of their illness since diagnosis for the on-treatment group was 2.36 months (range=0.60–5.43, SD=1.64 months) and for the relapse group was 29.9 months (range=24.60–37.40, SD=5.75). The diagnoses included leukemia (n=3, 30%) and other solid tumors (n=7, 70%). The average number of children including the patients per household was 3 (range 2–4, SD=0.94). No patient had ever used acupressure or acupuncture prior to study enrollment. None of the patients reported nausea or vomiting during the day prior to the chemotherapy being administered.
Specific Aims
Aim 1: To examine the feasibility of recruiting children with cancer into the larger study
Twenty-two (22) patients were approached for their willingness to participate. Five (5) parents refused due to time constraints. Seventeen (17) patients agreed to participate. Of the 17 who agreed, 2 patients received bone-marrow transplantation (BMT) and became ineligible. The treatment protocol was changed for 4 other children during data collection, and thus they also became ineligible to continue the study. One (1) patient refused to complete the study because she thought the intervention was useless and dropped out of the study. Thus, 10 patients completed the intervention.
Aim 2: To assess the feasibility of successfully completing each of the three protocols
During the two intervention trials, the patients were asked to keep the taped seeds on their ears for 7 days following the beginning of both rounds of chemotherapy. Thus, the possible total number of days the 10 children would keep the seeds on their ear was 140. The possible number was determined by multiplying 10 (children) times 2 (treatment conditions) times 7 days. During the treatment, 1 patient on day 2, 1 patient on day 5, and 1 patient on day 6 took off the tapes due to itching. These patients continued to complete the study assessment and were included in the final analysis. For the rest of the patients, the tape on the seeds fell off at different time points (i.e., from day 1 to day 7), and was replaced by the therapist as soon as it was noted. Therefore, the actual total number of days that the tapes were on the patients' ears was 123 or 88% of the possible days. This suggests that the intervention is acceptable to the children and their families and is therefore feasible.
Aim 3: To analyze the longitudinal CINV data
Change patterns of nausea occurrence, duration, and severity
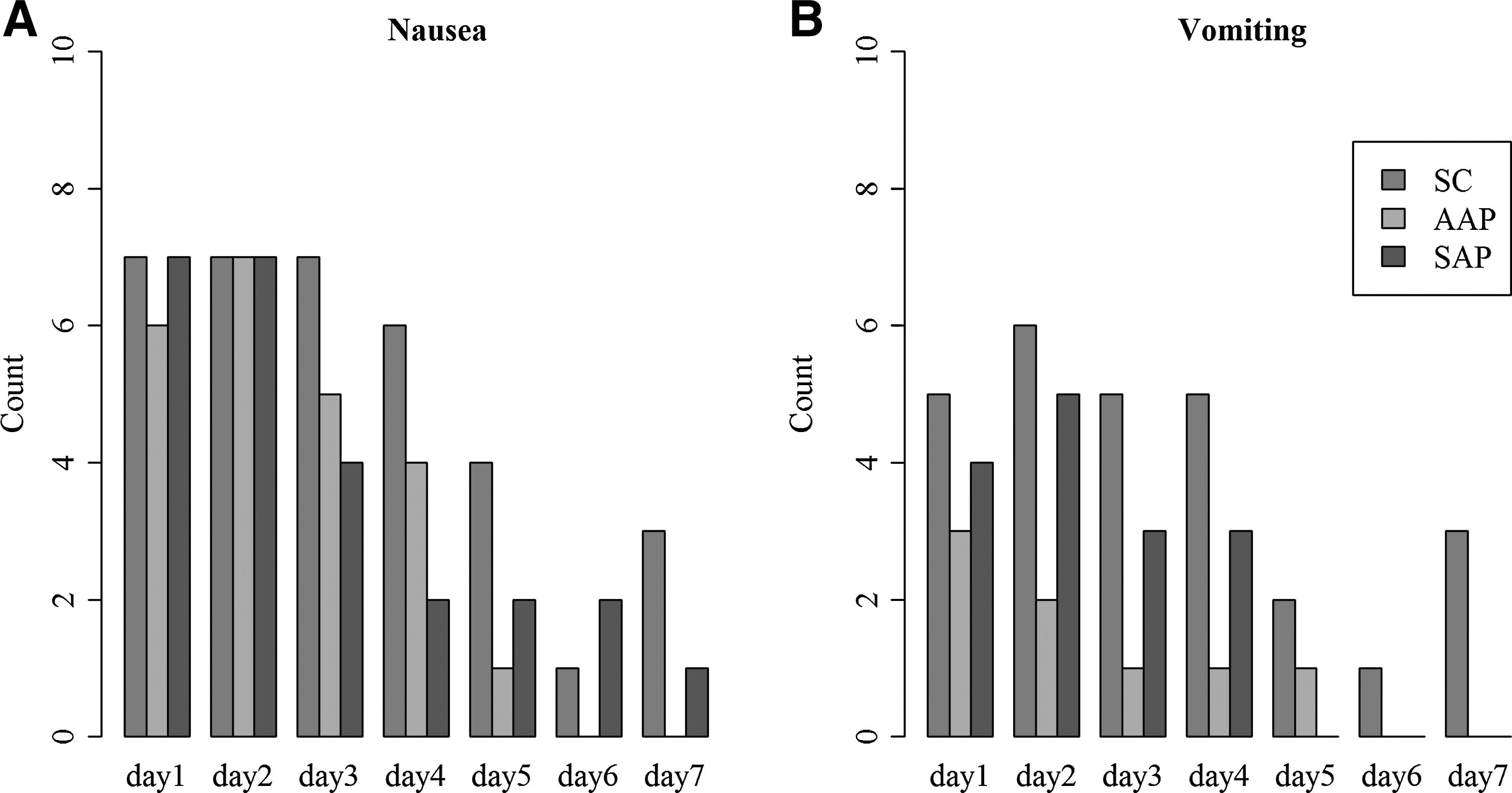
The graphic in Figure 3 shows the frequency of nausea and vomiting in the three groups. Because the actual day 1 data (the pretest data collection, prior to chemotherapy being administered, for all three groups) were reported as “none, or 0” for nausea and vomiting, the data for that day were eliminated and the day 2 data (first day after the chemotherapy) became day 1 for the purposes of analysis. The SC group reported more nausea overall than either the AAP or the SAP group (Fig. 3A). In the SC group, 3 children (30%) continued to report nausea even on the seventh day after the chemotherapy had been administered. The SAP group reported the same amount of nausea as the SC group for the first 2 days after the start of chemotherapy, but declined steadily after that with only 2 children (20%) still reporting any nausea on day 6 (Fig. 4). The AAP group reported slightly less nausea the first day, and the same as the other two groups on day 2, but declined until day 5, after which they reported no nausea. While the analysis did not show statistical significance, this trend seems clinically significant and suggests that a study with a larger sample should be conducted.
Occurrence of nausea

Duration
Table 1 presents the results of the post-hoc tests of multiple comparisons among the three groups across time. It shows that the patients in the AAP group had 0.3 times fewer occurrences of nausea (95% confidence interval [CI]=0.10, 0.88; p=0.0289) than those in the SC group. No statistical differences were found between the occurrences of nausea in AAP and SAP groups. This analysis is consistent with and supports the findings in Figure 3.
OR, odds ratio; CI, confidence interval; AAP, auricular acupressure acupoints; SAP, sham auricular acupoints; SC, standard care.
Change patterns of vomiting occurrence, duration, and severity
In Figure 3B, patients in the SC group reported more overall vomiting than patients either in the AAP or the SAP group, and patients in the SAP group reported more vomiting problems than patients in the AAP group. Only patients in the SC group reported vomiting at day 6 and day 7. Patients in the AAP group had 0.17 times (95% CI=0.05–0.53, p=0.0024) of having vomiting than patients at SAP, and patients at SAP had 0.39 times (95% CI=0.18–0.85, p=0.0172) of having vomiting than patients in the SC group. There were no statistically significant differences of vomiting occurrence between patients in the AAP or SAP group (OR=0.44, 95% CI=0.13–1.46, p=0.1775).
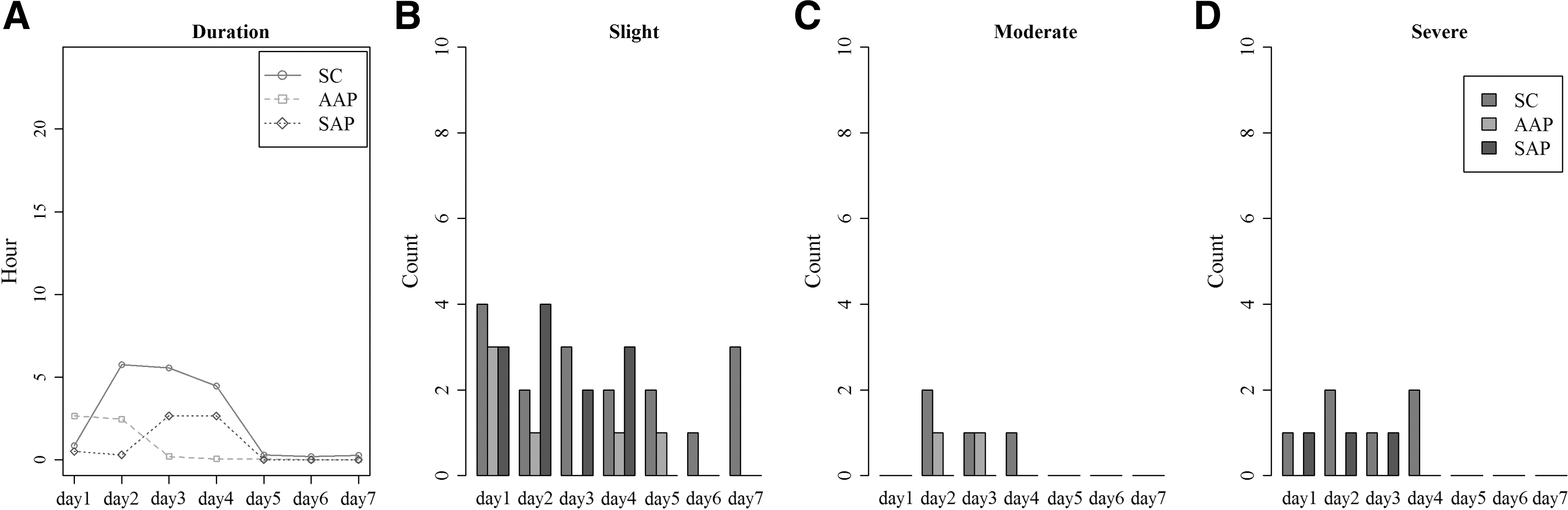
Except for acute vomiting, patients in SC group had experienced longer duration of vomiting (Fig. 5A) and higher severity (Fig. 5D) than patients in the AAP and SAP groups, but the differences were not statistically significant among the three groups (Table 2). The vomiting duration for AAP and SAP had mixed findings; for example, patients in the AAP group reported longer duration on the first 2 days, but a shorter duration from day 3 to day 5 than patients in the SAP group. Both the AAP group and SAP group had less severe level of vomiting occurrences, having 6.73 times (95% CI=2.25, 20.16, p=0.0007) and 3.02 times (95% CI=1.29–7.07, p=0.0111) significantly higher odds than the SC group, respectively. Even though the odds of the AAP group is 2.23 times higher than the odds of the SAP group, this is not significant (p=0.2346).
Duration
OR, odds ratio; CI, confidence interval; AAP, auricular acupressure points; SAP, sham auricular acupoints; SC, standard care.
Medication Taken to Prevent Nausea and Vomiting
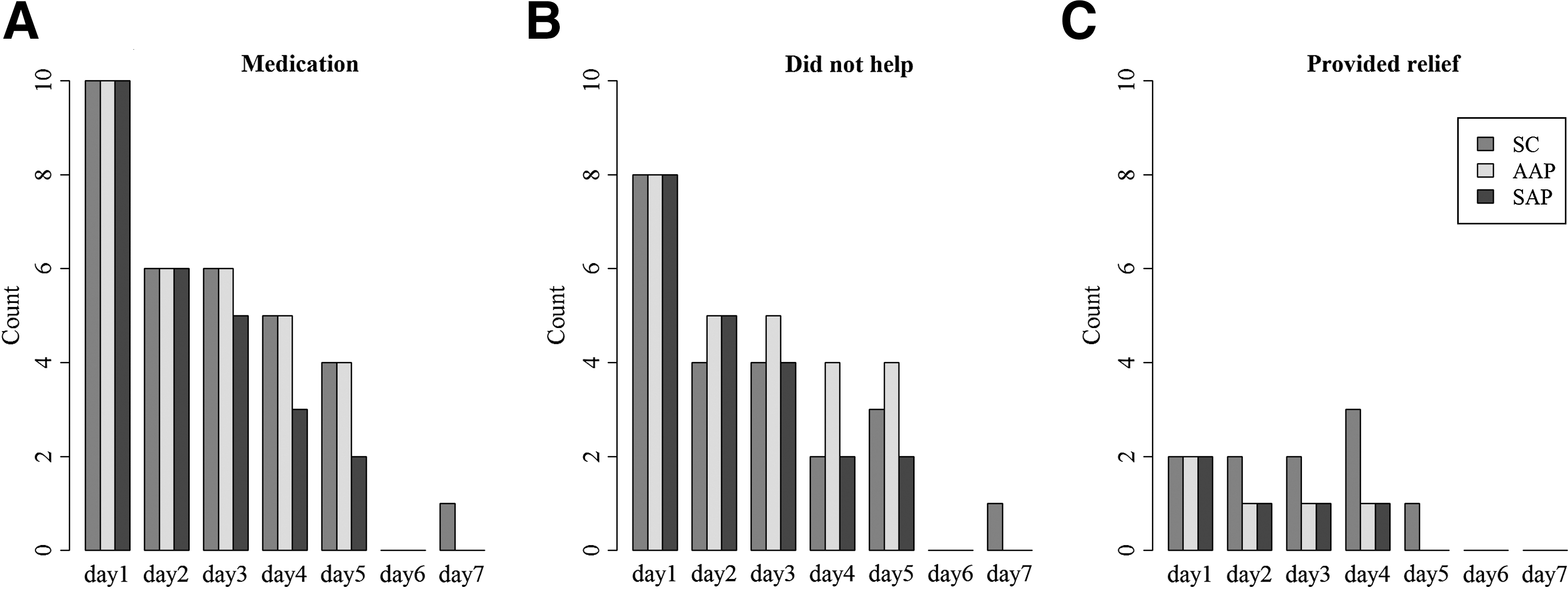
All of the patients in each of the three groups took medication to treat CINV on day 1 (on the day when CTX were administered) and gradually decreased the amount taken during the CTX. In Figure 6A, patients in the AAP group had a higher rate of using medication to prevent CINV than patients in the SAP or SC group, but there was no consistent finding about the medication taken to treat nausea and vomiting across time for three groups. Among the three groups (Fig 6B), about 80% of patients on day 1 and over 40% of patients on day 2 reported that the antiemetics did not help to treat CINV. The post-hoc analysis showed no significant differences among the three groups in either medication use or effectiveness of medication use (Table 2). The most use of antiemetics medication was Kytril (granisetron), followed by Zofran (ondansetron) (Fig. 7).
Medication use

Aim 4: To determine effect size for use in a future study of the efficacy of the intervention
In order to estimate the effect size, Cramér's φc was used. A total of 315 patients would be needed for three groups for a small effect size (Cramér's φc=0.2), 51 patients would be needed for a medium effect size (Cramér's φc=0.5), and 20 patients would be needed for a large effect size (Cramér's φc=0.8).
Discussion
This is the first feasibility study to assess auricular acupressure to prevent/treat CINV in children with cancer. The strength of this study was the inclusion of both an intervention and a placebo group to determine whether the AAP is effective due to treatment itself but not psychologic effects. This study has limitations due to small sample size, heterogeneous nature of the patients (including age, diagnosis), and the use of antiemetic regimens prescribed in the study setting.
In this study, the enrollment rate of the AAP in this study was 77%. The reasons given for refusal to participate were due to parental time constraints and patient's not wanting to fill out the questionnaire of self-report data, which is often encountered in survey studies. 6, 22 During the AAP treatment, 3 patients complained about itching of the tapes on day 2, day 5, and day 6 and decided to take them off. The tape that was used for AAP treatment had contained latex (provided by Auricular Medicine International Research & Training Center, FL). A latex-free, hypoallergenic, and gentle tape will be used for further AAP application in the future study in order to decrease the skin irritation for patients. Overall, 88% patients during the intervention were able to continue wearing their tapes until the study was completed. Some parents actively asked the auricular therapist if they could continue to receive the treatment after their participation in the study had ended. Thus, the authors have confidence to conclude that patients and parents can accept AAP as an addition to the usual care to prevent/manage CINV.
Conclusions
Due to the small sample size, it is not possible to differentiate the efficacy between AAP intervention and placebo (SAP) in this study. However, patients in the AAP group did have a lower occurrence of acute and delayed nausea and shorter vomiting duration than patients in SAP and SC groups across time. At the present time, it is not possible to draw the conclusion that the AAP is more effective than SAP due to the small sample size. The effects of AAP and SAP for treating CINV were varied across time. It is not possible to differentiate the true effects of AAP because of the possible psychologic effects of more frequent visits by the auricular therapist. The strength of this study design is the inclusion of a placebo group. A larger study with more subjects using the same design as was used here may be able to determine the effects of AAP in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.