
Abstract
Objectives:
The majority of individuals who survive a stroke are disabled because of persisting neurological impairments. The objective of this study was to evaluate the efficacy of subcutaneous electrical stimulation of the scalp in spontaneous functional recovery of patients with chronic ischemic stroke, by evaluating clinical, neurological, and functional findings.
Subjects and methods:
Sixty-two (62) subjects who were at least 18 months postdiagnosis of ischemic stroke were randomized to receive 10 sessions of placebo or active low-frequency electrical stimulation (2/100 Hz) using subcutaneous acupuncture needles over the scalp. Functional and neurological evaluations were indexed by the Barthel, Rankin, and National Institutes of Health Stroke Scale (NIHSS).
Results:
Results show that there was a significant difference in functional improvement between the sham and active group as indexed by NIHSS scale. The active group had a larger functional improvement after 10 sessions of scalp electrical acupuncture. The other two functional scales (Rankin and Barthel) failed to show significant differences between the two treatment groups.
Conclusions:
These results support further testing of scalp electrical acupuncture for the treatment of stroke as well further mechanistic studies to understand mechanisms associated with the observed improvement. Further studies need to consider longer follow-up assessments to investigate potential functional changes associated with electrical acupuncture.
Introduction
Aside from traditional forms of physical therapy, alternative forms of rehabilitation, such as acupuncture, may be beneficial in promoting long-term spontaneous recovery in patients who have had a stroke. Scalp acupuncture appears to be an innovative therapeutic method capable of treating cerebral or visceral diseases related to the cerebral cortex. This method consists of the introduction of needles in the subcutaneous tissue of the scalp at corresponding functional areas of the cerebral cortex. 2
Various studies have shown the possibility of clinical and functional improvement in ischemic stroke using nonscalp acupuncture techniques, 3,4 though evidence is mixed and a recent review concluded that there was not enough evidence supporting the effects of acupuncture for acute and subacute stroke. 5 On the other hand, other authors have evaluated the efficacy of electroacupuncture for treatment of stroke sequelae and showed some beneficial results. 6 Naeser et al. (1994) compared manual acupuncture's effect associated with electroacupuncture with a control group for the treatment of paralysis in patients who have had an acute stroke and who are undergoing physiotherapy. 6
As results are still mixed and there are no definite answers on the effects of electroacupuncture for chronic stroke, a sham-controlled randomized trial was conducted to evaluate the clinical effect of subcutaneous electrical stimulation of the scalp in patients with chronic ischemic stroke in a relatively large trial in 62 patients with chronic stroke.
Materials and Methods
Study population
Sixty two (62) subjects, 44 male and 18 female, with ages ranging from 24 to 65 years (mean=51.27±8.96), with definite diagnosis of ischemic stroke with at least 18 months of duration, from 1.5 to 16 years from the ictus (mean=7.88±4.35), 38 with right and 24 with left hemiplegia were studied. Patients with unstable or severe clinical conditions, significant perceptual and cognitive disturbances, including memory deficits and deficits that inhibit understanding of the proposed treatment, were excluded. Therefore, patients with a score of 21 or higher on the National Institutes of Health Stroke Scale (NIHSS) scale were excluded. Subjects were allowed to participate in the study only after signing the informed consent, and all study procedures were approved by the local ethics committee board and were compliant with the Declaration of Helsinki. After consent, subjects were randomly allocated into two groups. Group analysis at baseline shows that both groups were matched for age, duration postictus, gender, and baseline functional and neurological assessments.
Intervention: Scalp electrical acupuncture stimulation
Patients received 10 sessions of low-frequency electrical stimulation (2/100 Hz) applied through subcutaneous needles at the projection of the motor, sensory, frontal, and temporal associative areas of Penfield homunculus in the scalp, for 30 minutes, twice a week for 5 weeks. Electrical stimulation intensity was discriminative but bearable to the subject. Needles of 0.3-mm diameter and 40-mm long were applied to the subcutaneous tissues of the scalp in the projection of motor and sensitive areas of Penfield homunculus as well as frontal and temporal associative areas.
For sham stimulation, patients received 10 sessions of placebo electrical stimulation, through disconnected cables applied to the scalp, using the same parameters of treatment (duration of sessions and location of stimulation). During placebo stimulation, audiovisual feedback was evident to patients. See additional details regarding acupuncture in Table 1 using STRICTA guidelines and Figure 1 and Figure 2 for additional details on location of needles.
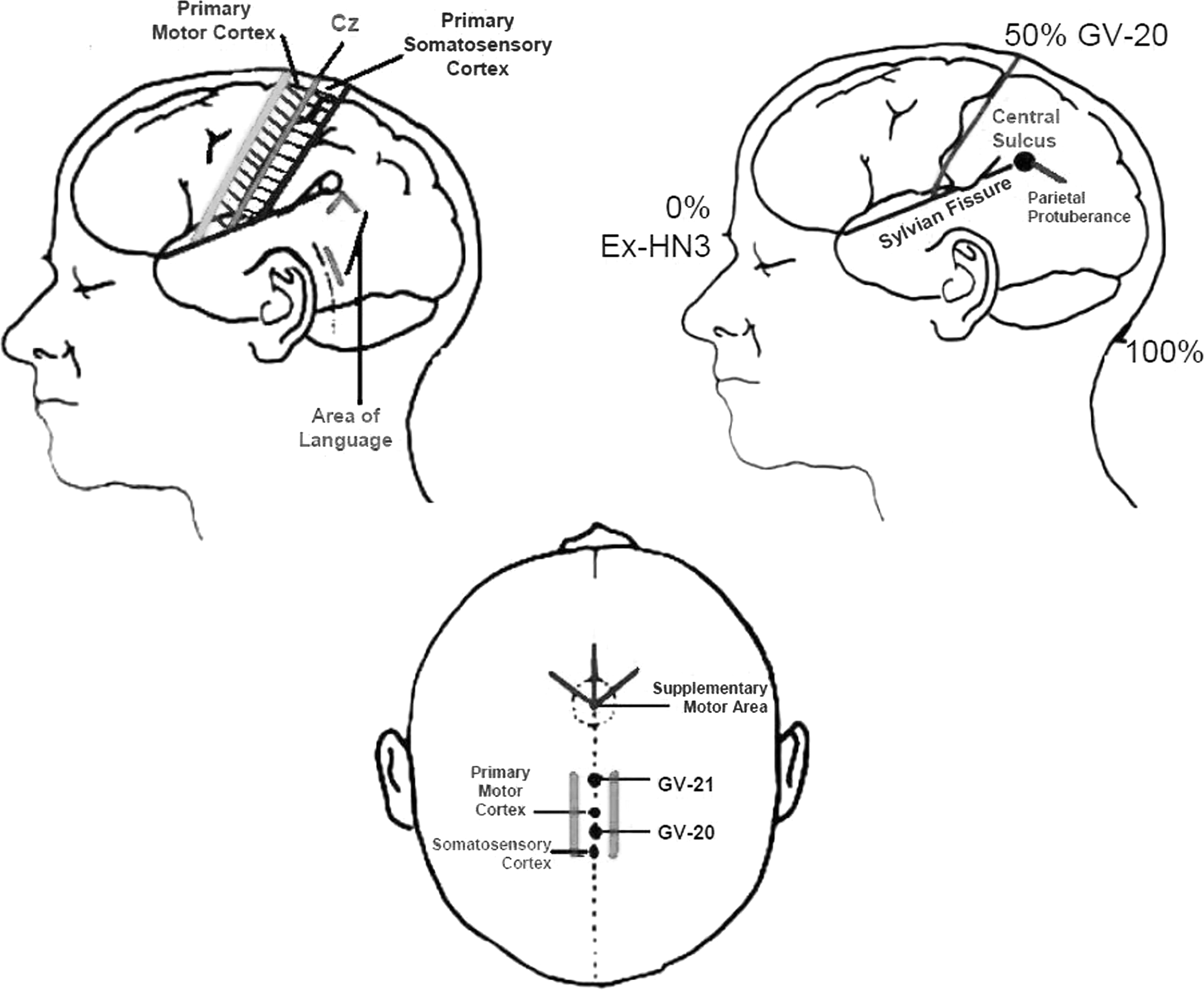
Diagram showing localization of acupuncture points using scalp landmarks such as Cz (GV20). Using these landmarks, it is possible to localize the primary motor and sensory cortex as well as supplementary and language areas.
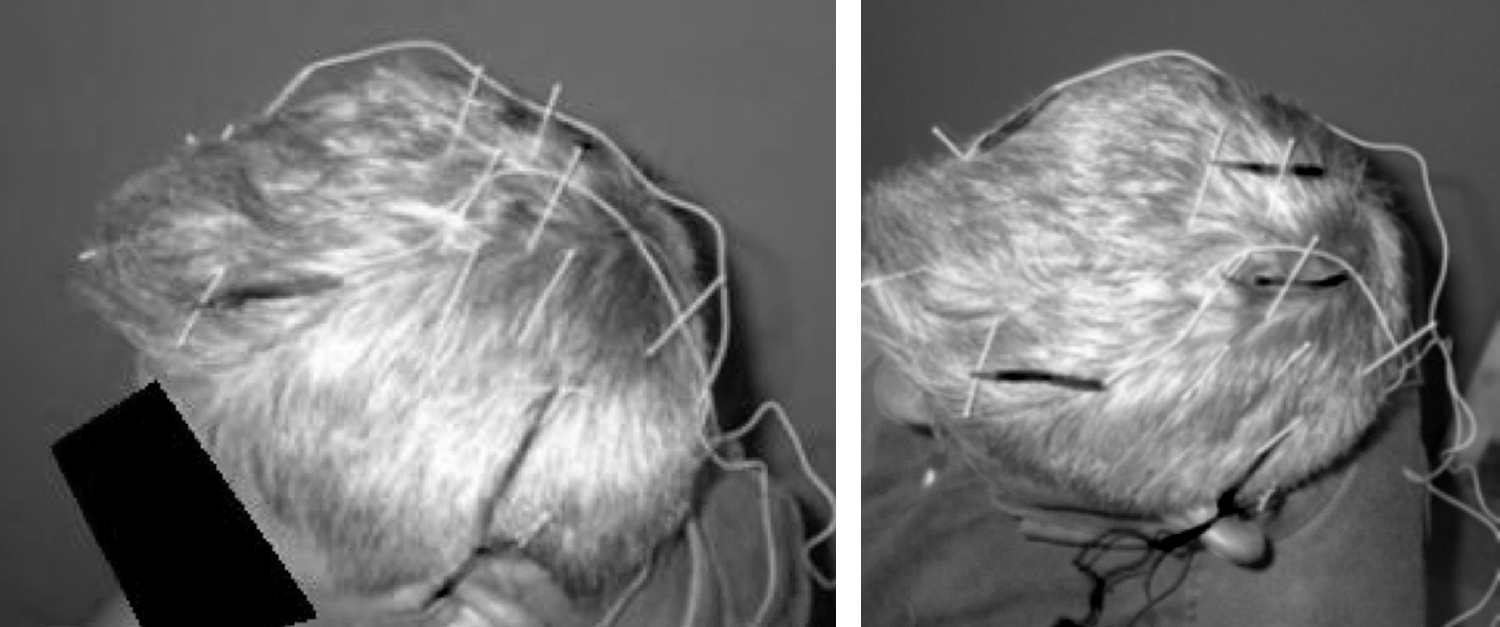
Patient receiving scalp electrical acupuncture as used in the trial. Six cables were attached to electrodes. In this case because it was a left-sided stroke, two electrodes were attached at the motor area, two electrodes were attached at the supplementary motor area, and two electrodes were attached at the language area.
Hu HH, Chung C, Liu TJ, et al. A randomized controlled trial on the treatment for acute partial ischemic stroke with acupuncture. Neuroepidemiology 1993;12:106–113.
Sällström S, Kjendahl, A, Osten PE, et al. Acupuncture in the treatment of stroke patients in the subacute stage: A randomized, controlled study. Compl Ther Med 1996;4:193–197.
Assessments
Subjects were evaluated before and immediately after 10 treatment sessions by examiners blinded to treatment group. Because there was interest in assessing clinical effects, blinded examiners evaluated neurological and functional outcomes including Barthel index, modified Rankin scale, and the NIHSS (for more information on NIHSS, go to:
Statistical analysis
For statistical analysis, STATA was used (StataCorp., College Station, TX). For the NIH and Barthel scales, mixed analysis of variance (ANOVA) models were conducted to assess whether there was a differential improvement when comparing active versus sham group. For Rankin scale, Fisher's exact test was used for this analysis. A significance level of 5% was adopted (α=0.05).
Results
Subjects tolerated treatment well, and there were no adverse effects reported. There were no dropouts during the trial. There were 62 patients enrolled who were randomized to the two treatment groups. At baseline, the two treatment groups were similar regarding demographic and clinical characteristics. Table 2 shows a summary of these data.
Measured in years.
M, mean; SD, standard deviation; MAX, maximum value; MIN, minimum value; N, number of cases.
Mixed ANOVA models were initially conducted so as to assess interaction effects between group and treatment for the Barthel and NIHSS scales. Significant interaction effects were found between group and time of stimulation for the NIHSS scale only (F1,60=4.92, p=0.03). For the Barthel scale, this analysis was not significant (F1,60=1.73, p=0.19). Results are shown in Table 3.
Significant difference noted; p=0.03; α<0.05.
SD, standard deviation; NIH, National Institutes of Health.
The pre- versus post-treatment were then compared in the active and control group for NIH scale and it was found that functional improvement was observed in the active group (p=0.0023) but not in the control group (p=0.86). For the Rankin scale, group results were compared using a Fisher t test because this scale is categorical. No significant differences were found for either group or time effects (p>0.05 in all analyses).
Finally, correlations were performed to assess whether the significant functional improvements were correlated with age or duration of stroke, and no significant results were found (p>0.05 for all the analyses), showing that these variables are not correlated with the outcome.
Discussion
In this study, a differential effect of active versus sham electrical stimulation was found only for NIHSS. The other two functional scales—Rankin and Barthel scales—did not show differential results.
The first important point to discuss is the conflicting results between the clinical neurological scale (NIHSS) and the functional scales (Rankin and Barthel). The NIHSS is an assessment of neurological function as a result of the stroke (e.g., level of consciousness, motor strength, etc.). The Barthel and Rankin scales measure functional outcomes (level of assistance in activities of daily living [ADLs]) dependent on the level of stroke. In addition, the NIHSS has more scale items than the Rankin or Barthel scales, and may be more sensitive with respect to scoring. One potential explanation for the significant results in the NIHSS assessment only is that this scale measures changes that can be detected acutely (i.e., during short-term assessment), whereas the Rankin and Barthel scales can detect the level of assistance needed or competence in ADLs as a result of the neurological changes in a larger time-frame. As a result, there may be subtle changes detected in the NIHSS scale that might not be reflected in the Rankin or Barthel scales. Because assessments were performed only immediately after treatment, it is not clear whether the improvements seen in NIHSS would be detected in the Rankin and Barthel scales, had assessment been done at a later time.
Another important issue to be discussed is the potential mechanisms underlying the improvement detected in this study. Because the intervention was electrical acupuncture, it is possible that both components—acupuncture and electrical stimulation—were involved in the therapeutic improvement. In order to compare these results with previous studies, results were analyzed from the three randomized clinical trials on acupuncture in chronic stroke as selected by a recent review that included only trials with rigorous methods. 5 Interestingly, the study using acupuncture only showed no significant effect of real acupuncture for spasticity, 7 whereas the study assessing scalp electrical acupuncture for chronic stroke showed a significant positive correlation between clinical changes in the affected upper limb and cortical activity in the ipsilesional motor cortex. 8 Finally, body electrical acupuncture resulted in a smaller effect (only for patients who were compliant with the protocol) in chronic stroke. 9 These results, in addition to the current results, suggest that the electrical component might be critical during acupuncture treatment for chronic stroke. Future studies should compare in the same trial regular acupuncture versus electrical acupuncture versus regular peripheral electrical stimulation in order to detangle the effects of this treatment because electrical stimulation might be the main component to explain the significant clinical effects. 10
Some limitations should be discussed. Because the intention was to increase external generalizability in this study, the population of this study was heterogeneous. Although this study had a relatively large population, it is possible that by increasing the number of subjects studied, it may change the significance in the other scales, though the authors were interested in meaningful clinical changes. Additionally, it is emphasized that the functional rating evaluation scales—Rankin and Barthel—did not show enough sensitivity to detect short-term changes. Some patients already presented near maximum functional scores in all evaluations performed. Therefore, further improvements could not be detected in those patients. Asymptomatic and severely disabled patients were excluded from the study; therefore, major changes would not occur. It is also possible that the results from Rankin and Barthel scales may be due to a type II error. However, post-hoc power calculation shows that effect size (given power of 80% and α of 5% and 62 patients) is 0.035, which is a small effect size, therefore making less likely this hypothesis.
Further investigations should employ other scales capable of detecting minor improvements, including quality of life and patient's satisfaction level. The clinical observation in this study demonstrated that patients from the control group reported improvement in subjective issues such as dizziness. The therapeutic group, however, reported subjective improvement during activities such as range of motion, muscle strength, and mainly that movements were easier to perform. This phenomenon may suggest a reduction in spasticity, which was not directly evaluated through those scales. Further investigations should specifically evaluate spasticity, including gait analysis and surface electroneuromyographic studies, and also should study the neural mechanisms associated with this intervention so as to understand and optimize the effects of scalp electrical acupuncture for chronic stroke.
Footnotes
Disclosure Statement
No competing financial interests exist.