
Abstract
Objectives:
The study objectives were to examine the effect of a 12-week 30-minute-a-day Ping Shuai Qigong exercise program on climacteric symptoms and sleep quality in perimenopausal women.
Design:
This was a prospective observational study.
Settings/location:
The subjects (N=70) from two communities were women aged 45 years and above who were experiencing menopausal symptoms.
Subjects:
Thirty-five (35) women from one community were assigned to a Ping Shuai Qigong intervention group, while 35 women from the other community were assigned to the control group.
Interventions:
This was a 12-week, 30-minute-a-day Ping Shuai Qigong program.
Outcome measures:
The Greene Climacteric Symptom scale and the Pittsburgh Sleep Quality Index were the outcome measures.
Methods:
Descriptive analysis and repeated-measures analysis of variance were used.
Results:
Pretest scores at baseline found no significant group differences in climacteric symptoms or sleep quality. Significant improvements in climacteric symptoms were found at 6 weeks and 12 weeks (t=4.07, p<0.001 and t=11.83, p<0.001) in the intervention group. They were also found to have significant improvements in sleep quality in those times (t=5.93, p<0.001 and t=10.58, p<0.001, respectively).
Conclusions:
Ping Shuai Qigong improved climacteric symptoms and sleep quality in perimenopausal women at 6 weeks and 12 weeks. The longer a person practiced this form of meditative exercise, the greater the improvement in sleeping quality and climacteric symptoms.
Introduction
Exercise is one alternative method that might relieve the symptoms of menopause, but its effectiveness is unclear. 9,10 In India, one study of the effect of an 8-week yoga program on the climacteric symptoms of 120 women aged 40–55 years found that yoga caused significantly greater improvements in vasomotor symptoms and psychologic factors in the yoga group than in the control group. 11 However, several studies have found no effect of exercise on menopause symptoms. 9,12,13 For example, using a questionnaire and interviewing, Boraz et al. found no difference in symptoms between the intervention (behavioral lifestyle intervention) and control groups and no difference between controls and intervention with MHT use. 12 Wilbur et al. randomly assigned 173 white and African American women aged 45–65 years who were not on MHT and had no major signs or symptoms of cardiovascular disease to either a moderate-intensity walking group or a no-exercise control group. After 24 weeks, no differences were observed between the groups in symptoms (vasomotor, urogenital/sexual, psychologic, and cognitive functions). 10 Another study of 173 overweight postmenopausal women who had not received MHT for 6 months assigned 87 women to an experimental group, which participated in a moderately intense exercise intervention program, and 86 women to a control nonexercise group. A significant increase in hot flash severity and decreased risk of memory problems was observed in the exercise group compared to the controls over 12 months. 14
A growing body of research suggests that traditional mind–body practices, such as yoga, t'ai chi, and qigong, may offer safe and cost-effective strategies for reducing the risk of cardiovascular disease, improving mood, well-being, and sleep. 15,16 For example, a cluster randomized trial by Chen et al. examined the effects of 6 months of silver yoga exercises (defined as warmup, hatha yoga gentle stretching, relaxation, and guided-imagery meditation) in promoting sleep quality for 62 experimental groups and 66 controls for community-dwelling older adults aged 60 years and over and found that sleep quality (including sleep duration, subjective sleep quality, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction) of all those in the experimental group were improved compared to the controls. 17 Vera and colleagues studied 16 experimental and 10 control subjects to examine the effect of yoga on sleep quality and found that long-term yoga practitioners (defined as a minimum of 3 years of practice) were associated with better sleep quality. 18
In summary, the effects of various types of exercise on climacteric symptoms in menopausal women have been inconclusive. Although yoga has successfully improved sleep quality, most of the studies included elders and may not have included perimenopausal women. The aims of the present study therefore were to examine the effect of Ping Shuai Qigong on climacteric symptoms and quality of sleep. It was hypothesized that menopausal women assigned to the practice Ping Shuai Qigong would have improvement in climacteric symptoms and subjective sleep quality at 6 and 12 weeks as compared to women in the control group.
Definition of Ping Shuai Qigong
Ping Shuai Qigong, an easily taught, conveniently practiced, form of exercise, was used in this patient group. Ping Shuai Qigong is a Chinese meditative psychosomatic exercise that integrates movement, breathing, and meditation into a single practice. While practicing, participants stand well balanced in one place with legs slightly bent. While paying attention to their breathing, they allow their arms to swing forward and backward in rhythm to a light repetitive squatting-rocking motion of the body. It is easily learned and can be practiced anywhere. The Ping Shuai Qigong can rebalance sympathetic/parasympathetic tone by integrating deep breathing and meditation. 19
Materials and Methods
Study design and sample
This study was approved by the Institutional Review Board of the National College of Nursing Hospital as well as by the Research Ethics Committee of the Taipei City Hospital Heping Branch in Taipei, Taiwan. All study participants were provided with a letter explaining the details of the study and informing them that they could withdraw from the study at any time. The informed consent was obtained before the study began. The Ping Shuai Qigong instructor and the community nurse signed agreements assuring that patient anonymity and confidentiality would be respected.
For this prospective observational study, a trained Ping Shuai Qigong teacher, who had practiced Ping Shuai Qigong for 10.5 years and is certified by the Association of Ping Shuai Qigong, was invited to lead the intervention group. Women aged 45 years and above were solicited who were willing to participate in the study from two different communities when they gathered together for a community activity. Based on Pass 11.0, the required sample size was 43 for each group (power=0.80; α=0.05; effect size in 0.31). However, after the inclusion criteria applied (inclusion criteria were described in the section of Intervention and Control Groups), 90 women were eligible from each community, but only 36 of them were willing to participate in the study. The two communities located in the Taipei area were 4 km apart. Then, the principal investigator of this study assigned one community as the intervention group and the other as the control group. None of the participants had learned how to practice qigong (including other types of qigong, t'ai chi, or yoga) before. Two (2) dropped out of the study due to the inconvenience of personal schedules; the resulting sample thus contained 35 each for the intervention and control group and a completion rate of 97%. The nurse administered a questionnaire at 6 weeks and 12 weeks after baseline to collect demographic information and administer the Greene Climacteric Scale and The Pittsburgh Sleep Quality Index (Fig. 1).

Flow diagram of data collection.
Intervention and control groups
The instructor demonstrated and led the intervention group in a session of Ping Shuai qigong. All members of the intervention group practiced Ping Shuai qigong in group for 30 minutes per day for 12 weeks, led by the qigong instructor. The participants in the control group were visited by the same community nurse at community health examination counseling and did not practice Ping Shuai qigong. They were also followed up at 6 and 12 weeks using the same measures. None of them practiced Ping Shuai qigong by themselves during the study period.
Criteria for inclusion of patients from the study included having clear consciousness (defined as being awake and responsive to one's environment as well as no signs or symptoms of memory problems/dementia), being able to walk, having no neuromuscular disease, and being able to communicate in Chinese or Taiwanese. One trained community was recruited nurse to screen whether the participants had irregular menstrual patterns, hot flashes (a sudden warm feeling with blushing), night sweating, mood swing, fluctuations in sexual desire, and trouble sleeping. If the participants complained of these symptoms, they were approached to be enrolled in the study. The nurse was blinded to the intervention/control status of participants. Those with the following were excluded: (1) disease history such as cancer, heart disease, and hypertension; (2) physical disability; (3) previous experience with other forms of qigong (including yoga and t'ai chi); and (4) previous history of use of MHT, steroid use, or regular consumption of health foods containing Ganoderma lucidum, ginseng, or ginkgo within the past half year.
Primary outcome measures
These measures were used to compare the menopause symptoms and quality of sleep among baseline, 6 weeks during the study, and 12 weeks later. 1. Greene Climacteric Scale (GCS) The GCS was administered at three different points: pretest, post-test I (6 weeks during), and post-test II (12 weeks later). The GCS was used to measure a total of 21 symptoms.
20
The severity of each symptom was rated using a 4-point scale: not-at-all (0), a little (1), quite a bit (2), and extremely (3). As can be seen in the Appendix, Symptoms are for anxiety (items 1–6), depression (7–11), somatic symptoms (12–18), vasomotor symptoms (19–20), and sexual dysfunction (item 21). While there are 21 different items on the GCS, the total symptom disturbance ranged between 0 and 63. Internal consistency of the scale was acceptable (Cronbach α=0.85 and 0.83 for psychologic, 0.66 and 0.66 for somatic, 0.80 and 0.84 for vasomotor symptoms, for baseline and follow-up assessments, respectively).
21
The scale reliability has been reported to be 0.83 for a Spanish population,
22
0.87 for a German population,
21
and 0.91 for an Indian population, respectively.
11
The translation and back-translation techniques were employed to improve the reliability and validity of research. The quality of a translation was verified by an independent translator translating back into the original language. Original and back-translated GCS were then compared. 2. Pittsburgh Sleep Quality Index (PSQI) The PSQI measures seven categories: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction.
23
The client self-rates each of these seven areas of sleep. A 4-point Likert scale 0–3 was used to measure sleep disturbances (10 items) with 0 indicating not during the past month, 1 indicating less than once a week, 2 indicating once or twice a week, and 3 indicating 3 or more times a week. Subjective sleep quality was also measured using a 4-point Likert scale ranging from 0 (very good) to 3 (very bad). A global sum of “5” or greater indicated a “poor” sleeper. The total range was 0–21, with higher scores indicating worse sleep quality. The PSQI has internal consistency and a reliability coefficient (Cronbach α) of 0.80 for the global PSQI and 0.83 for its seven components.
24
The Chinese version has been found to have a reliability coefficient of 0.82–0.83 (Tsai et al., 2005).
25
The test–retest reliability has been reported to be 0.87.
26
Statistical analyses
Data were summarized descriptively. For categorical variables (education, occupation, and menstruation cycle), the χ2 test was used to examine the association between the two groups. Independent t-tests were used to detect any significant group differences in age. Two tools were used to investigate the effects of the interventions on subjects' climacteric symptoms and PSQI scores after interventions. First, it was examined whether there were differences in climacteric symptoms and PSQI between intervention and control groups. Second, paired t-tests were used to compare in the baseline scores with 6-week scores as well as the baseline scores with 12-week scores in intervention and control groups, respectively. Repeated-measures analysis of variance was used to determine whether or not there were significant differences in climacteric symptoms and PSQI at baseline, 6 weeks, and 12 weeks, while controlling for age. All values are presented as mean±standard error. A p<0.05 was considered significant. All statistical operations were performed using SPSS-PC (version 15.0 for Windows). Power analysis was above 0.80 by PASS 2008.
Results
Descriptive analyses
No differences by groups were observed in age (intervention 48.60±1.94 versus control 48.69±2.04), marital status (80% for intervention versus 88.6% for control), or high school education (51.4% versus 48.6%). While most of the intervention group were housewives (57.1%), most the controls had full-time jobs (54.3%), although these differences were not statistically significant (χ2=0.915, p=0.339) (data not shown).
No significant baseline differences were observed in symptoms (intervention=18.66; control=18.74; t=−0.142, p=0.888) and PSQI scores between the groups (intervention=9.97; control=9.60; t=1.126, p=0.264). Further examining each subscale in the two tools, it was also found that there were no discernible group differences at pretest scores (data not shown). The intervention group was found to have greater improvements than the control group in symptoms (four subscales) and sleep quality (seven subscales) at 6 weeks and at 12 weeks, especially at 12 weeks (Table 1). However, no difference was found in loss of interest in sex and the use of sleeping medication between the two groups at these two times (Table 1). In paired pre–post tests, the intervention group had significantly reduced symptoms at both 6 weeks (mean=17.97; t=4.07, p<0.001) and 12 weeks (mean=14.03; t=11.830, p<0.001), compared to pretest scores (mean=18.67) (Tables 2 and 3). We found similar results for PSQI at 6 and 12 weeks (t=5.925, p<0.001 and t=10.585, p<0.001). For the control group, only a few differences were found between the pre- and post-test symptom scores, though their overall scores were nonsignificantly lower than the pre-test scores at 6 weeks and 12 weeks (t=3.217, p<0.01and t=2.315, p<0.05). Somatic (physical) scores remained similar (Table 3). No difference was observed in the controls' PSQI scores and subscales at baseline, 6-week, or 12-week scores.
SD, standard deviation; PSQI, Pittsburgh Sleep Quality Index.
Comparison of two-difference standard error=0 is shown by “-”.
p<0.05; ** p<0.01; *** p<0.001.
SD, standard deviation.
p<0.05; ** p<0.01.
SD, standard deviation.
Effects of Ping Shuai Qigong on climacteric symptoms
After controlling for age, a significant improvement was observed in symptoms of participants in the intervention group (mean difference=−0.549; p<0.001) directly after the Ping Shuai Qigong. Because Mauchly's Test of Sphericity was not supported (Mauchly W=0.443, p<0.001), three different statistical tests were chosen (Greenhouse-Geisser, Huynh-Feldt, and Lower-bound test) to correct for the lack of sphericity. The age effect (as a covariate in the model) was significant (F=30.19, p<0.001; partial η2=0.317). The group significant effect also demonstrated the effect of Ping Shuai Qigong on symptoms (F=14.15, p<0.001; partial η2=0.179) (data not shown). A significant difference was observed among the three statistical tests (data not shown). Therefore, the pairwise comparisons were further examined and the symptom scales were found to be lower at 6 weeks than at baseline (mean difference=−0.549, p<0.001). In addition, the symptom scales were lower at 12 weeks than at 6 weeks (mean difference=−1.929, p<0.001) and baseline (mean difference=−2.477, p<0.001), respectively (Table 4). The stronger effect of the intervention was on symptom at 12 weeks (Table 2, Fig. 2).

Difference in the effect of Ping Shuai Qigong on climacteric scale between the intervention and the control groups.
Age was the covariate in the model.
SE, standard error; PSQI, Pittsburgh Sleep Quality Index.
Effects of Ping Shuai Qigong on PSQI
The participants in the Ping Shuai Qigong group had significant improvement in PSQI (mean difference=−0.586; p<0.001) at 6 weeks after the Ping Shuai Qigong. Because Mauchly's Test of Sphericity was not supported (Machly's W=0.734, p<0.001), three different statistical tests (Greenhouse-Geisser, Huynh-Feldt, and Lower-bound test) were used to correct for lack of sphericity. The age effect (as a covariate in the model) was not significant (F=0.011, p=0.915; partial η2=0.0002). However, the group effect also demonstrated the effect of Ping Shuai Qigong was found to have a significant impact on PSQI (F=12.39, p=0.001; partial η2=0.156) (data not shown). Upon further analysis, the interaction of intervention group-by-time on PSQI was statistically significant (Pillai's trace=0.587, F=46.97, p=0.001), and examination of pairwise comparisons revealed that the PSQI at 6 weeks was lower than it was at baseline, reflecting better sleep quality. In addition, their PSQI at 12 weeks was lower than it was at both 6 weeks and at baseline (Table 4, Fig. 3).
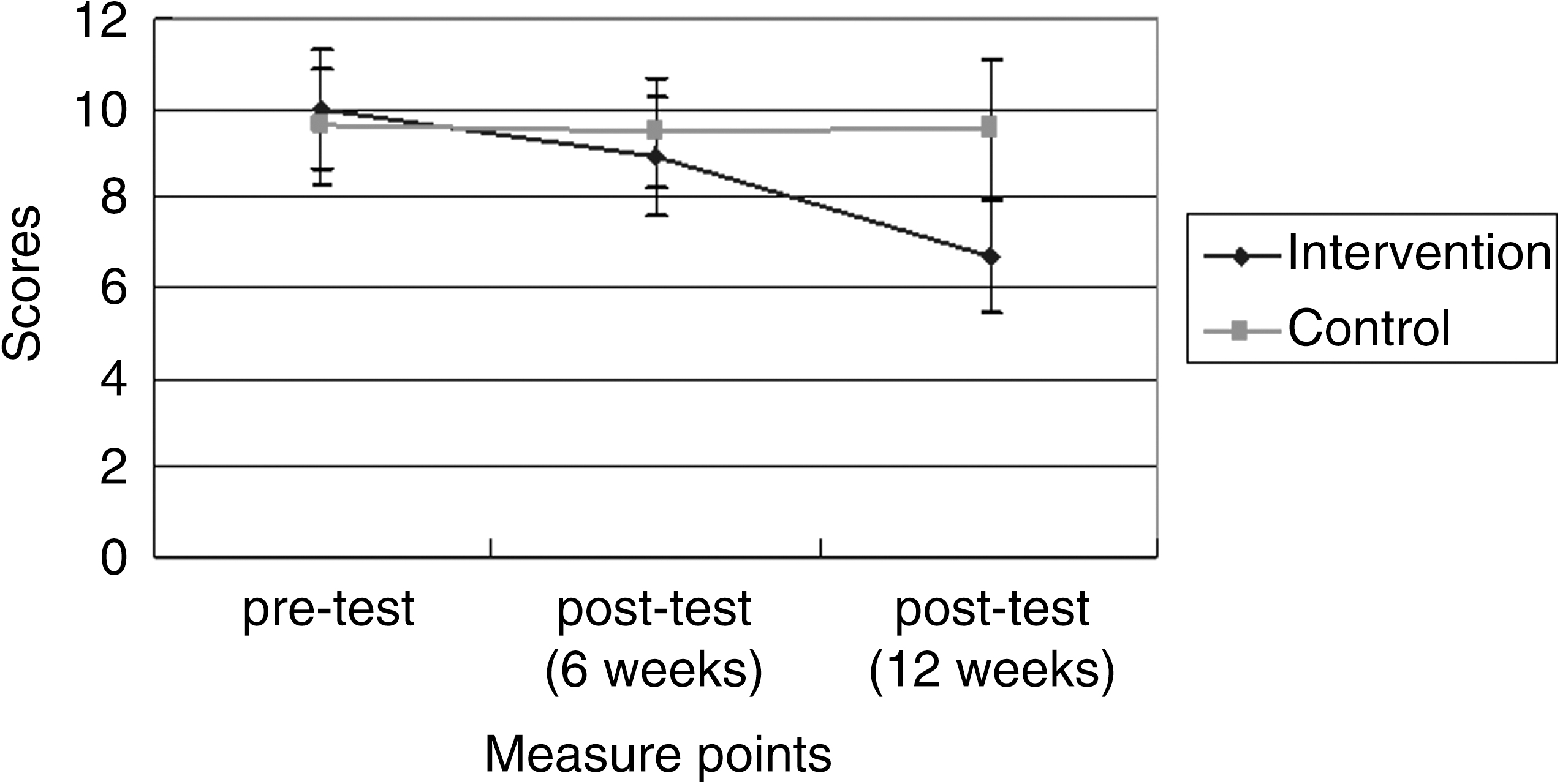
Difference in the effect of Ping Shuai Qigong on Pittsburgh Sleep Quality Index between the intervention and the control groups.
Discussion
This study found that Ping Shuai Qigong significantly improved symptoms and subjective quality of sleep in menopausal women at 6 weeks and 12 weeks. It appeared to have a greater effect on sleep latency, habitual sleep efficiency, and sleep disturbance than on the other three dimensions (subjective sleep quality, sleep duration, and daytime dysfunction). Several other studies have also reported other forms of qigong to have an effect on sleep quality. 16,27,28 The results of this study regarding this form of exercise and sleep differed from others in that the present study found that the intervention group had greater improvements than the control group in sleep quality (seven subscales) at 6 weeks and at 12 weeks, especially at 12 weeks.
The Ping Shuai Qigong group also had significant improvements in several symptoms, particularly psychologic, somatic, and vasomotor symptoms. The longer (12 weeks compared to 6 weeks) the women practiced the Ping Shuai Qigong, the greater their improvements. These results are similar to those of Chattha et al., 11 who reported that the practice of Indian yoga improved vasomotor and psychologic symptoms in a similar population, but different from Wilbur et al., who reported that 6 months of walking exercise did not improve vasomotor or psychologic symptoms in menopausal women. 10 Other studies using t'ai-chi chuan as the intervention report decreases in somatic symptoms (hot flashes) also. 29 However, a yearlong, randomized, clinical trial by Aiello and colleagues studying the effect moderate-intense exercise on menopause symptoms in overweight, postmenopausal women not taking MHT found that the exercise program increased the severity of some symptoms (such as hot flashes) in a small number of women. 14 While yoga, t'ai chi, qigong, and Ping Shuai Qigong are also meditative exercises, they may affect the participant differently than other forms of exercise, even though walking can be turned into a form of meditative exercise using Vipassana meditative techniques. 30 Ping Shuai Qigong did not improve the participants' interest in sex. Interest in sex can be related to interpersonal factors as well as physiologic 31 –33 and psychologic factors. 34 –36 These factors need more studies in the future.
Although the improvement of somatic symptoms was not as big as those of the intervention group, the control group also had significant improvements in somatic symptoms, which led the authors to wonder whether the nurse gave any extra attention (compensatory equalization of treatments) to the control group. However, if this were the case, then psychologic symptoms should have been changed also, and it did not. In addition, it might be possible to alleviate symptoms without any particular treatment (i.e., MHT or an alternative medicine). 37 Another possibility was due to lacking randomization. These may need longer periods of time, another placebo control group, or randomization to prove it.
The present results add to the existing literature by illustrating the relationship between Ping Shuai Qigong and menopause symptoms and sleep quality. However, important limitations of the present work should be highlighted. First, during the study period, the participants may have had the opportunity to learn more about perimenopause and menopause from various sources, and this could have conceivably increase their own daily intake of isoflavone-enriched foods to alleviate their symptoms of menopause, such as hot flashes. 38,39 Second, it was possible that interventions were practiced more than 30 minutes daily due to personal difference in motivation. Third, although the trained community nurse screened the eligibility of our participants, it was still based on participants' self-evaluation. Fourth, the distinct advantage of repeated-measures designs, since the same subjects are being used repeatedly, is that far fewer subjects are required for the study. 40 However, the small sample size limited the power of this study at 6 weeks (around 0.71), although the power increased to 1.0 at 12 weeks. Fifth, the participants were not randomly assigned to each community. This may have an influence on the results of this study due to bias. Sixth, menopause is usually defined as the time when there has been no menstrual period for 12 consecutive months. However, based on the inclusion criteria of this study, perimenopausal women who may be menstruating regularly or irregularly were included. This may partially explain the improvement in somatic symptoms. Future research will need to include a stricter definition for menopause (i.e., no menstrual period for 12 consecutive months). Finally, “expectation” or “personal belief” may have a strong impact on the report of medical symptoms. 41,42 Women in the intervention group might have an expectation of improvement, while those in the control group did not. Thus, further studies should contemplate another placebo group, such as mild walking programs to control for the effect of expectation.
Conclusions
The findings in this prospective observational study provide initial evidence that the 12-week Ping Shuai Qigong program significantly improved the subjective sleep quality and most climacteric symptoms in the intervention group at 6 weeks and particularly at 12 weeks, compared to the controls for perimenopausal women. Ping Shuai Qigong seems to be an easy exercise and very economical; thus, 45–53 years women will benefit from it if they experience the symptoms and sleep problems studied here. However, since this study only lasted for 12 weeks and had only 72 participants, the authors strongly suggest that the future study should increase the sample size and be much longer, and follow-up may be necessary after the end of the study.
Footnotes
Acknowledgments
The authors are very grateful to all those who participated in this study. Dr. Huang Chia-Hsiung is thanked for his consultation on methodology issues. No financial support was provided for this study.
Disclosure Statement
No competing financial interests exist.
| Symptoms | Not at all | A little | Quite a bit | Extremely | |
|---|---|---|---|---|---|
| 1 | Heart beating quickly or strongly | ||||
| 2 | Feeling tense or nervous | ||||
| 3 | Difficulty in sleeping | ||||
| 4 | Sudden excitability | ||||
| 5 | Attacks of panic | ||||
| 6 | Difficulty in concentrating | ||||
| 7 | Feeling tired or lack in energy | ||||
| 8 | Loss of interest in most things | ||||
| 9 | Feeling unhappy or depressed | ||||
| 10 | Crying spells | ||||
| 11 | Irritability | ||||
| 12 | Feeling dizzy or faint | ||||
| 13 | Pressure or tightness in head or body | ||||
| 14 | Parts of body feeling numb or tingling | ||||
| 15 | Headaches | ||||
| 16 | Muscle and joint pains | ||||
| 17 | Loss of feeling in hands or feet | ||||
| 18 | Breathing difficulties | ||||
| 19 | Hot flushes | ||||
| 20 | Sweating at night | ||||
| 21 | Loss of interest in sex |