
Abstract
Despite the availability of many treatment options, depressive disorders remain a global public health problem. Even in affluent nations, 70% of reported cases either do not receive the recommended level of treatment or do not get treated at all, and this percentage does not reflect cases of depression that go unreported due to lack of access to health care, stigma, or other reasons. In developing countries, the World Health Organization estimates that <10% receive proper depression care due to poverty, stigma, and lack of governmental mental health resources and providers. Current treatments do not work for everyone, and even people who achieve remission face a high risk of recurrence and residual disability. The development of low-cost effective interventions that can serve either as initial therapy for mild symptoms or as adjunctive therapy for partial responders to medication is an immense unmet need. Positive activity interventions (PAIs) teach individuals ways to increase their positive thinking, positive affect, and positive behaviors. The majority of such interventions, which have obtained medium-size effect sizes, have been conducted with nondepressed individuals, but two randomized controlled studies in patients with mild clinical depression have reported promising initial findings. In this article, the authors review the relevant literature on the effectiveness of various types of PAIs, draw on social psychology, affective neuroscience and psychophamacology research to propose neural models for how PAIs might relieve depression, and discuss the steps needed to translate the potential promise of PAIs as clinical treatments for individuals with major and minor depressive disorders.
Introduction
Even more alarming are the current rates of treatment. From 2001 to 2003, only 30% of adults in the United States reporting mood, anxiety, or impulse control disorders received “minimally adequate treatment.” 7 This means that, even in affluent nations, 70% of reported cases either do not receive the recommended level of treatment or do not get treated at all, and this percentage does not reflect cases of depression that go unreported due to lack of access to health care, stigma, or other reasons. In developing countries, the WHO estimates that less than 10% receive proper depression care due to poverty, stigma, and lack of governmental mental health resources and providers. 1
High Costs of Depression Treatment
Therapeutic interventions are costly, due to the need for a trained or licensed therapist to direct therapy. Treatment costs for depression in the United States can range from $200 for three psychotherapy sessions to over $1,200 for the American Psychological Association's recommended course of treatment of 10 psychotherapy sessions combined with antidepressant medication for optimal care of moderate to severe depression. 8 In addition, individuals at relatively high risk of developing depressive disorders, such as those with low education or financial duress, may be the least able to afford treatment. 9 Even in developing countries where generic antidepressants are widely available, their cost remains high relative to per capita income.
Critiques of Drug Therapy
Depression is a heterogeneous condition with molecular and biochemical origins that are still not fully understood. Hence, it is not surprising that current drug therapy is suboptimal. Response rates to a single antidepressant are generally considered to be 60%–70%, 10 with over 80% of the drug effect accounted for by placebo effects. 11 Even with this relatively high percentage of “responders” to drug treatment, initial pharmacotherapy produces remission in only 30%–40% of the depressed population. Furthermore, a substantial delay exists in onset of treatment action, leading both patients and clinicians to wait several weeks before determining whether augmentation or modification is needed. Practice guidelines suggest that, when either drugs or therapy are not yielding symptomatic relief within 4–8 weeks, clinicians should switch or add a complementary treatment (i.e., add drugs to therapy or therapy to drugs). 12 Unfortunately, however, the response rates diminish with additional strategies, and about one third will not remit even after two to four pharmacotherapy treatment trials. 13 Finally, although drugs can be very helpful for many patients, they can be associated with adverse effects (such as sexual side-effects) that patients often must endure to obtain the benefits. 12
Even when successful, drug therapy has been criticized for not arming patients with personalized tools they can use to prevent relapse and remission. Many, but not all, studies have shown that patients treated to remission with behavioral activation or cognitive therapies are less likely to relapse after treatment termination than patients treated to remission with medication. 14 –16 Although cognitive and behavioral approaches to treating depression have their own limitations, they appear to teach patients strategies that enable them to avoid falling back into negative thought patterns and behaviors.
Augmenting Treatment by Moving Beyond a Focus on Reducing Symptoms
Cognitive, behavioral, and interpersonal approaches to treating depression are effective in reducing acute distress in depressed patients and compare favorably to medication among all but the most depressed individuals. 12 In theory and in practice, all of these approaches, including cognitive therapy, behavioral activation, and interpersonal therapy, focus on alleviating the symptoms of depression (for example, by modifying maladaptive beliefs, 16 recognizing avoidant behaviors, 17 or focusing on interpersonal problems that may be causing the patient distress). 18 Although all of these approaches to treating depression have met with success, no technique works for everyone. Accordingly, the use of positive activity interventions (PAIs, described in the next section) is proposed to complement current drug and psychotherapeutic treatment. The authors also suggest the neural mechanisms through which PAIs might serve to ameliorate symptoms of depression.
The Benefits of Positive Activity Interventions
In the last half-century, the field of psychology has witnessed tremendous progress by focusing on the worthy pursuit of mitigating individual suffering. Researchers in the area of positive psychologic science believe theorists can now learn even more about the human condition by studying what is “right” in flourishing individuals. 10 The body of work already compiled not only advances researchers' understanding of why some people are happy, grateful, and optimistic, 19,20 but also suggests how people can learn to practice intentional activities to increase their levels of these positive attributes. These ideas have broad relevance to the treatment of depression, as a singular focus on ameliorating depressive symptoms, the main thrust of most therapeutic and drug approaches to depression treatment, could leave patients in a languishing state in which they do not suffer from depression but still have a low sense of well-being. 21 It is argued that PAIs, which aim to help patients experience positive thoughts, affect, and behaviors, can galvanize them to move past the point of simply “not feeling depressed” to the point of flourishing.
Common positive exercises that have been tested in randomized controlled interventions include writing letters of gratitude, 22 –24 counting one's blessings, 25 –27 practicing optimism, 22,23,28,29 performing acts of kindness, 30,31 meditating on positive feelings toward others, 32 and using one's signature strengths. 24 Because PAIs teach patients ways to increase their positive cognitions, emotions, and behaviors without professional help, they may serve as vital tools to prevent relapse in response to potential depression triggers, like stress. Because they are cost-effective and convenient to deliver, PAIs can also help lessen the gap between the treated and untreated in the depressed population. Finally, because PAIs are self-administered, patients will attribute improvements in their moods and symptoms to their own doing, and not to an external agent (i.e., an antidepressant or a therapist). Patient empowerment is especially important, considering that autonomy is a core psychologic need, 33 and an internal locus of control negatively correlates with depression. 34 Although the number of empirically validated PAIs may seem small, scientists know a great deal about the general psychologic mechanisms that make PAIs effective, including boosting positive emotions and facilitating experiences that meet people's core needs for autonomy, relatedness, and connectedness. In sum, the authors believe that treatments should strive to cultivate an individual's well-being, as well as other areas of his or her life (e.g., work, relationships, health), rather than only ameliorating depressive symptoms. 35,36
The Value of Positive Emotions
Why should boosting well-being be a priority – or even relevant – for those who treat depression? The answer rests in studies supporting the value of positive emotions, which are the hallmark of well-being. Positive emotions do not just make people feel good; they have been found to foster successful outcomes in numerous life domains, including superior job performance, higher creativity, greater marital satisfaction, enhanced social relationships, and better physical health. 36 The benefits of positive emotions are especially relevant to those suffering from depression, as positive emotions have been shown to speed recovery from the cardiovascular effects of negative emotions, 37,38 improve broad-minded coping skills, 39 and buffer against relapses. 40
Even momentary positive feelings can produce durable resources (e.g., new ideas, new relationships), as positive emotions have been shown to broaden thinking and attention. 41 Broadened mindsets bring about novel ideas and actions (e.g., the urge to play and explore) and lead to the building of long-term social, psychologic, intellectual, and physical skills and reserves. For example, if a person gets 15 minutes of positive emotions from counting her blessings, she may muster the energy to attend the art class she always considered attending, and, while in class, might meet a friend who becomes a companion and confidant for years to come. Among individuals with depression, higher levels of approach-oriented motivation are associated with less severe depression and a greater likelihood of recovery. 42 In contrast to the narrowing of attention 43 and behavioral inhibition 42 characteristic of negative states, positive emotions trigger upward spirals toward greater flourishing, resilience, and psychologic well-being. 39
Positive Activity Interventions
Positive activities such as the regular practice of gratitude, optimism, kindness, and meditation are similar in that they are all relatively brief, self-administered, and nonstigmatizing exercises that promote positive feelings, positive thoughts, and/or positive behaviors, rather than directly aiming to fix negative or pathological feelings, thoughts, and behaviors. Randomized controlled longitudinal experiments have validated the effectiveness of these intentional activities in raising well-being and reducing depressive symptoms. 44
Psychologic Mechanisms Underlying the Effectiveness of Positive Activities
Although positive psychology is still a developing field, the relatively small but growing number of studies on PAIs are beginning to identify important mechanisms underlying the benefits of such interventions. Previous studies by Lyubomirsky and colleagues, for example, have found evidence that the relation between a positive cognitive intervention and subsequent decreases in depressive symptoms is mediated by increases in positive affect. 45 Similarly, a study with Anglo-Americans and Asian-Americans found positive experiences, as well as feelings of control and connectedness, to mediate the relationship between the PAI and subsequent increases in well-being. 22 It is believed that assessing potential mediating variables—such as positive thoughts, positive behaviors, and positive feelings (see Fig. 1 for a proposed theoretical model)—will advance understanding of the psychologic mechanisms or “key ingredients” underlying why PAIs work, thus helping refine current positive interventions and design new ones.
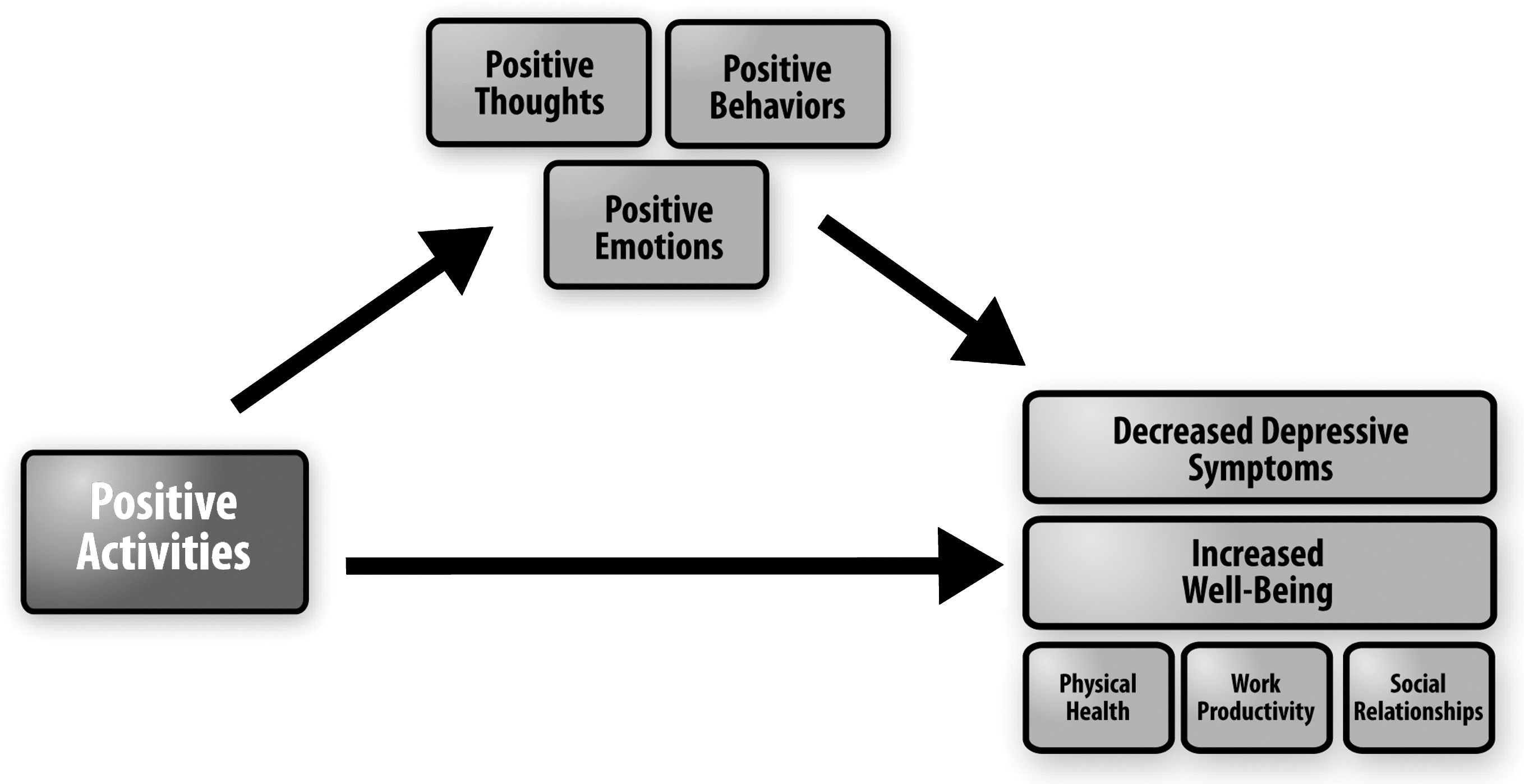
Schematic diagram of the proposed theoretical model of the psychologic mechanisms by which positive activities decrease depressive symptoms, increase well-being, and foster positive outcomes in relationships, work, and health. The critical mediating variables are increases in positive thoughts, positive emotions, and positive behaviors.
Studies with Depressed Individuals
Sin and Lyubomirsky's recent meta-analysis of 51 positive psychology interventions with both depressed and nondepressed participants revealed that PAIs are effective for enhancing well-being and ameliorating depressive symptoms. 46 The magnitude of these effects was medium-sized (mean r=0.29 for well-being and 0.31 for depression)—an impressive finding, considering that many of these interventions were very brief, self-administered positive activities rather than therapy (see Table 1 for individual, self-administered, PAI study effect sizes). To compare, a classic meta-analysis of 375 psychotherapy studies found that psychotherapy demonstrated an average effect size r of 0.32 for outcomes such as self-esteem and adjustment. 47
Note: Positive effect sizes indicate superiority of Positive Activity Interventions (PAIs) over comparison group for increasing well-being (WB). Negative effect sizes indicate superiority of comparison group over PAI for increasing WB. For age category: C/A, Child/Adolescent (up to 17 years old); YA, Young Adult (18–35 years old); MA, Middle Adult (35–59 years old); OA; Older Adult (60 years old and up). For comparison group type: TAU, treatment as usual. Participants in the Seligman et al. (2005) study (in bold type in the table) were deemed mildly depressed as groups had mean levels of depression scores between 14 and 15 on the Center for Epidemiological Studies Depression Scale. The Seligman (2002) study is not included in the table as there was insufficient information to calculate an effect size. However, the mean difference in depression scores from pre- to post-test indicated that the PAI decreased depression scores from the severe to the mild-to-moderate range.
Given that many previous trials of PAIs have been conducted with young and healthy participants, an important question is whether the practice of positive exercises yields similar benefits for depressed populations. Although the Sin and Lyubomirsky meta-analysis demonstrated that depressed individuals can actually benefit more from positive psychology interventions than nondepressed ones, many of the studies that used clinically depressed populations were conducted in the context of individual or group therapy. 44 Based on the significant body of research showing that clinician-administered PAIs increase well-being, we believe that self-administered PAIs will be successful as well. Presumably, depressed individuals are relatively eager to feel better and may put more effort into the positive activities; greater incentives and effort have been shown to increase the treatment effect in past studies. 23,28 Furthermore, PAIs have a lower barrier of entry for those lacking motivation, energy, or enthusiasm. A depressed person should be much more likely to complete a positive activity at home than locate a therapist, arrange an appointment, and drive to a therapist's office. Finally, although happiness and depression are theoretically distinct constructs, low levels of happiness are highly correlated with depression scores, 48 –50 thus further supporting the prediction that PAIs shown to increase well-being will also serve to decrease depressive symptoms in clinically depressed individuals.
As one example, Seligman and colleagues conducted an online experiment in which they randomly assigned 411 volunteers—who were mildly depressed, on average, with a mean score of 14.1 on the Center for Epidemiologic Studies Depression scale (CES-D)—to engage for 1 week in one of five well-being–enhancing activities (involving practicing gratitude, positive thinking, and one's strengths) versus a placebo control activity (involving writing one's early experiences). 24 Participants in the placebo condition experienced a short-term boost, but returned to their baseline after a week. By contrast, those who completed the positive exercises experienced a boost in well-being and a decline in depressive symptoms, and these benefits were maintained after the intervention ended. Two (2) of the activities—writing about three good things in one's life and using one's signature strengths in a new way—resulted in lasting improvements in depression and well-being for 6 months. This study demonstrates that even simple, self-guided exercises can bring long-term benefits to mildly depressed or dysphoric individuals. Unfortunately, however, remission rates and clinician ratings of depression change over treatment were unavailable for this online study. Indeed, to date, no large randomized trials of PAIs as adjunctive acute therapy to medication in patients with depressive disorders and no trials examining its effects on long-term functional recovery and disability have been conducted. The authors propose that a randomized clinical trial including PAIs as a treatment condition is needed to directly compare these simple, self-administered positive activities to treatment as usual.
Rapid Response
Notably, every treatment group in the abovementioned study showed significant decreases in depressive symptoms after just 1 week or less of participation.* These results indicate that not only can PAIs be effective in reducing depressive symptoms, but that they can also work quickly. In another study, Seligman instructed severely depressed individuals (CES-D mean of 33.9) to engage in the “three good things” PAI every day. Within 15 days, participants' CES-D scores decreased by 16.7 points (from severe to mild-to-moderate depression) and 94% experienced relief. 51 Thus, although the development, research, and implementation of positive psychology interventions are in their early stages, such interventions show promise for improving the lives of many, and doing so at a relatively rapid pace.
Potential Neural Mechanisms Underlying the Effectiveness of Positive Activities as Treatment for Depression
If PAIs can successfully alleviate subjective reports of depressive symptoms, how might they impact mood-relevant or reward-relevant neural circuits? Although work addressing this question is still largely limited and indirect, it can draw on 2 decades of research into the cognitive and affective neuroscience of mood disorders. Functional neuroimaging studies have led to a hypothetical neural model in which major depressive disorder (MDD) is a result of a lack of coordination between the dorsal attention–cognitive control system and ventral limbic–affective systems. 52,53 Evidence using positron emission tomography 54,55 has shown decreased dorsal cortical activity and increased ventral limbic activity associated with negative mood. Although the results have not always been consistent due to differences in tasks or patients' clinical profiles, fMRI studies 56,57 have also revealed a hypofunctioning dorsal cognitive control system and a hyperfunctioning emotional system. Furthermore, case–control studies in depressed patients without medication 58 have found elevated activation in response to negative stimuli in the amygdala, as well as either decreased or increased activation in the dorsolateral–prefrontal cortex (dlPFC) and dorsal anterior cingulate cortex, depending on task load. 59 Pilot studies of patients on antidepressants have found a reversal of this pattern as a result of mood improvement. 53,58,60 Whereas antidepressants have been hypothesized to target the amygdala and other limbic regions directly and affect a bottom-up pathway, cognitive behavioral therapy (CBT) has been proposed to operate on the dorsal cognitive control system and to affect a top-down control pathway. 52,55,61 Antidepressants appear to increase the activity of the dlPFC, 60,62 whereas CBT may decrease dlPFC activity and increase activity in the hippocampus and the dorsal cingulate. 63
Alterations in the Reward-Related Neural System in Depression
Anhedonia is a core symptom of depression, 12 and a number of functional magnetic resonance imaging (fMRI) studies have shown reduced activation in the reward system in patients with MDD. 64,65 This reduced activation has been correlated with self-reported low positive affect, suggesting that the activation of the reward circuit detected by fMRI is related to current emotional experience. 65 The regions traditionally implicated in reward-related processing, such as the expectation of reward 66 and the experience of pleasure 67 and social rewards, 68 include the ventromedial PFC, caudate, nucleus accumbens, and the midbrain (such as the ventral tegmental area). 69 –71 Studies using positive stimuli have revealed decreased activation in MDD versus normal subjects in the ventral striatum. 72 For example, researchers have found a negative correlation between anhedonia (but not depression severity) and ventral striatal responses to positive stimuli. 72 Research has also indicated that activation in the left frontal region is associated with greater levels of positive, approach-related emotions, while activation in the right frontal region is associated with negative, withdraw-related emotions. 73 –75 However, these reward-related brain regions have not been fully integrated into models of depressive disorders, an area worth studying further in the context of PAIs.
Possible Brain Mechanisms Underlying PAIs
In the absence of any fMRI studies of PAIs in major and minor depressive disorders, it can only be speculated how PAIs might affect the brain circuitry when administered as an adjunct to other depression therapies. Because nonresponders to pharmacotherapy continue to exhibit increased amygdala activation, one could postulate that improvement of core mood symptoms and anhedonia with PAIs in such individuals might be linked to downregulation of the hyperactivated amygdala response and upregulation of the reward system. If participants are able to improve their cognitive strategies (e.g., feelings of control or connectedness) through PAIs, then such effects might be linked to beneficial neural changes in the “top-down” dorsal cognitive control pathway (see Fig. 2 for a proposed model). fMRI-based studies of connectivity in the limbic and reward circuits in patients with depressive disorders before and after receiving PAI adjunctive therapy will be needed to answer such questions. A three-arm randomized study comparing PAIs to CBT and pharmacotherapy in a sample of partial responders with depressive disorders with fMRI outcomes would be the only way to examine empirically whether the relevant mechanisms differ and which mechanisms result in the best clinical and quality-of-life outcomes.

The three circles are a schematic illustration of the key affective–cognitive–hedonic neural dysfunctions observed in untreated or partially treated participants with major and minor depressive disorders. The arrows depict how a combination of medication or cognitive–behavioral therapy plus positive activity interventions might provide optimal recovery. Clearly this is an oversimplification of a complex syndrome, and individual treatments will act on more than one domain. Also, many molecular downstream targets might influence the outcomes. For these reasons, this should be viewed as a working model.
Need for Further Studies of PAIs in Depressive Disorders
Clearly much work needs to be done to directly test the efficacy of PAIs as a treatment for major and minor depressive disorders and investigate both the psychologic and neural mechanisms underlying their effectiveness. PAIs might be suitable as monotherapy for mild depressive or adjustment disorders, as well as adjunctive therapy for partial responders to medication. In both settings, the need exists for 8- to 12-week randomized controlled trials to test the efficacy of PAIs as acute therapy to examine response and remission rates in comparison to usual care. Given the attractiveness of PAIs for vulnerable populations such as children, elderly, and medically ill, trials will need to be representative of such populations. Longer-term studies (e.g., 6–12 months) to study the efficacy of PAIs for maintaining sustained remission and preventing recurrences will also be needed. Studies to better understand the mechanisms underlying potential benefits of PAIs could yield significant insights. Given the potentially high benefit–risk ratio of PAIs in improving depression outcomes, the authors believe such studies should be a priority for funding agencies focusing on alternative therapies.
Self-Administered Treatment
Self-administered interventions, which can be delivered outside of a clinic, have several key advantages over solely clinical treatments. Self-administered treatments cost significantly less than therapeutic interventions and are more convenient to deliver. For example, for a relatively trivial cost, interventions can be delivered via the Internet, DVDs, workbooks, and, recently, mobile phone applications (such as the iPhone-based LiveHappy,™ grounded in Lyubomirsky's positive psychology research 35 ). Once implemented, a self-administered treatment can service a large number of patients, without the need to add more trained personnel. With the advent of social media, computer-based treatments do not have to be solitary activities, but can also facilitate interpersonal support from peers and therapists.
Admittedly, self-directed treatments are not without their disadvantages. The meta-analysis of PAIs found that individually delivered positive psychology interventions show the greatest benefits, followed by group-administered interventions. 46 This finding makes practical sense, as some populations may not benefit from self-administered treatment. For example, self-administered activities would not be ideal for those suffering from severe depression or for individuals with a bias against “self-help” who may perceive positive activities as “cheesy” or “hokey.” Nevertheless, the meta-analysis showed that, in addition to individual and group therapies, partaking in self-administered positive activities also significantly enhanced well-being. The authors argue that this approach strikes a compelling balance between effectiveness and the widest possible delivery. 76
Conclusions
While the efficacy of antidepressant medication and therapeutic interventions for alleviating depressive symptoms has been shown to be greater than that of placebo in many trials, the effect sizes remain small to medium and success rates may be diminishing. A recent publication analyzed 81 randomized, double-blind clinical trials, with 21,611 evaluable patients, that were submitted to the U.S. Food and Drug Administration as part of new drug applications for an antidepressant medication claim between 1983 and 2008. 77 The analyses were limited to completed, randomized, multicenter, double-blind, placebo-controlled clinical trials, both U.S. and global trials, in adult patients diagnosed with MDD according to Diagnostic and Statistical Manual of Mental Disorders, 3rd edition (DSM-III) or DSM-IV criteria. Only 53% of all these MDD trials in the last 25 years were found to be successful, implying that 47% failed to separate from placebo. Furthermore, these data showed that over the last 25 years, treatment effect size clearly diminished at a similar rate for both U.S. and non-U.S. trials, despite a marked increase in the sample size of the trials, and that placebo rates slightly increased. Such findings are consistent with the widely accepted notion that current medication treatments (1) are not successful for a sizable proportion of patients, (2) incur a heavy financial burden, (3) frequently take weeks to be effective, (4) may be stigmatizing for some, and (5) hold a risk of both minor and serious side-effects. The authors believe it is worthwhile to test a new category of depression interventions, PAIs, which (1) have the potential to benefit depressed individuals not responding to pharmacotherapy or not able or willing to obtain treatment, (2) are relatively less expensive to administer, (3) are relatively less time-consuming and promise to yield rapid improvement of mood symptoms, (4) hold little to no stigma, and (5) carry no side-effects.
Although positive psychologic science is only about a decade old, positive interventions have already gained considerable theoretical and practical support in the literature. Future research on PAIs in clinical settings would further the treatment of depression in two important ways. First, by cultivating positive thoughts, feelings, and experiences, rather than aiming solely to ameliorate depressive symptoms, PAIs represent a unique approach that may appeal to people who are not optimally served by cognitive–behavioral or interpersonal therapies, as well as patients who are already taking antidepressant medication, but have shown a small to moderate response. Both such groups of individuals are ideal candidates for complementary approaches. Second, the self-administered nature of PAIs allows for potentially wide and cost-effective distribution of the treatment.
Footnotes
Disclosure Statement
P.M.D. has received research grants (through Duke) and served as a paid speaker/advisor for several pharmaceutical companies, advocacy groups, and government agencies. He owns stock in DailyFeats, a company focusing on social wellness. No competing financial interests exist for other authors.
*
Even participants in the control condition improved after 1 week. Simply engaging in a presumably positive activity may confer temporary benefits. However the benefits of the “placebo” activity wore off quickly, while the benefits for PAIs persisted.