
Abstract
Objectives:
The objectives of this study were to evaluate the efficacy and interaction of Keigai-rengyo-to extract (KRTE) and acupuncture in male patients with acne and the feasibility of a large clinical trial.
Design:
A randomized, assessor single-blinded, 2×2 factorial trial was conducted. The trial is registered with the Clinical Research Information Service, Republic of Korea: KCT0000071.
Subjects:
Forty-four (44) participants with acne vulgaris were randomized into one of four groups: waiting list group (WL), KRTE only group (KO), acupuncture only group (AO), and KRTE and acupuncture combined treatment group (KA).
Intervention:
After randomization, patients in the AO and KA groups underwent eight sessions of acupuncture treatment, twice per week. Patients in the KO and KA groups were prescribed KRTE 3 times daily, 7.4 g each dose, after meals, for 4 weeks.
Outcome measures:
The following outcome measurements were used in examination of subjects: mean percentage change and the count change of inflammatory and noninflammatory acne lesions, Skindex 29, investigator global assessment from baseline to end of trial, and proportion of dropouts and compliance with KRTE.
Results:
A significant interaction of KRTE and acupuncture was evident according to mean percent change of inflammatory acne lesions, but not of noninflammatory acne lesions from baseline to the end of the study. Statistically significant differences were observed in the primary effect on mean percent change of noninflammatory acne lesions, not by acupuncture, but by KRTE. Adjusted Skindex 29 score changes indicated no statistically significant reduction within groups and between groups. The improvement rate in patients with KRTE and acupuncture treatment was not significant, compared to patients with no KRTE and acupuncture treatment. The proportion of dropouts was 22.7% and rate of compliance with KRTE was 92.3%.
Conclusions:
For treatment of acne vulgaris, use of KRTE combined with acupuncture is recommended for inflammatory lesions and KRTE only is recommended for noninflammatory lesions. Further large-scale trials assuming a higher dropout rate and aimed at confirming the ability of KRTE and acupuncture to improve inflammatory and noninflammatory lesions in patients with acne are needed.
Introduction
Despite the use of well-established guidelines for acne vulgaris care, a substantial number of patients with acne use Oriental medicine (OM) due to dissatisfaction and frustration with Western medical treatments and concern regarding their side-effects, such as skin pigmentation, facial edema, cheilitis, and ocular sicca, among others. 8 –11 Herbal medicine and acupuncture are two of the major tools of OM therapy, and have frequently been administered for treatment of acne symptoms in clinical practice worldwide, especially in East Asia. In South Korea, Japan, and China, the evidence-based potentiality of the use of herbal medicine and acupuncture with safety and efficacy in treatment of acne vulgaris has been suggested. 12 –24 However, current evidence concerning the efficacy of herbal medicine and acupuncture for treatment of acne does not sufficiently support its effect in clinical practice. Recent studies have shown the limitations of randomized controlled trials of herbal medicine and acupuncture: They may have been of poor quality in terms of their randomization method, patient and/or assessor blinding, or sample size. Also, these studies rarely demonstrated an interaction between herbal medicine and acupuncture, despite use of a combination of herbal medicine and acupuncture in clinical practice, and have rarely used a waiting list or Western medical treatment group as a control group.
In consideration of these methodological flaws, a trial was conducted to evaluate the efficacy and interaction effect of Keigai-rengyo-to extract (KRTE) and acupuncture using the 2×2 factorial design and the feasibility of a large clinical trial. KRTE is an herbal medicine that is often used for treatment of acne vulgaris in clinical practice, and is approved for treatment of acne, sinusitis, and otitis media by the Korea Food and Drug Administration. Because females can easily be affected by the level of sex hormones, including estrogen and androgen, relevant to increased sebum production through the menstrual cycle, 25,26 the participants were restricted to male patients with acne vulgaris.
Materials and Methods
Study design
This study was a single blinded (assessor), randomized, 2×2 factorial trial conducted from June 2009 to February 2011 at the Oriental Medical Hospital of the Kyung Hee Medical Center. This study was approved by the hospital's institutional review board (IRB) (KOMC IRB 2009-06). The 2×2 factorial design was selected for examination of the efficacy and interaction of KRTE and acupuncture on acne vulgaris.
Study population
From June 2009 to February 2011, 45 applicants were screened and 44 male participants were enrolled who met the following criteria: (1) 13–35 years of age; (2) >10 papules and <20 nodules on the face (Korean Acne Grading System grade 2–4; Table 1); and (3) occurrence of acne for >3 months (chronic stage). Participants were excluded if (1) they had received Western medical treatment (i.e., retinoids, antibiotics, chemical peeling, intense pulsed light, or laser treatment) or OM treatment (i.e., acupuncture, moxibustion, or herbal medicine) for acne within 1 month before entry; (2) after screening via blood test, they did not meet the normal range (normal range: hemoglobin 13–17 g/dL, platelet 150,000–350,000/mm3, aspartate transaminase [AST] 0–40 IU/L, alanine transaminase [ALT] 0–40 IU/L, blood urea nitrogen [BUN] 8–23 mg/dL, and creatinine 0.6–1.2 mg/dL); (3) they had papules or nodules mainly located on the chest or back; (4) they had keloid acne, corticosteroid acne, or other infectious skin diseases; (5) they had an internal disease that required treatment without delay; or (6) they were unable to comply with the study guidelines. During the trial, no concomitant acne treatments were permitted, and patients were advised to avoid use of comedogenic makeup or sunscreen.
Papule: acne <5 mm.
Nodule: acne >5 mm.
Participants were recruited via an Internet advertisement posted on the website of the Kyung Hee Medical Center and via ad posters. Each participant was notified of the study procedures, and written informed consent was received.
Because this trial was designed to be of short duration, lasting 4 weeks, with the intention of decreasing the dropout rate, the desired sample size for this pilot study was 44 patients, with 11 for each group, assuming a dropout rate of 10%.
Study flow and intervention
After recruitment, participants were randomly assigned to one of four groups: waiting list (WL), KRTE only (KO), acupuncture only (AO), and KRTE/acupuncture combined treatment (KA) group (Table 2). Randomization was performed at a site remote from the trial location. Random numbers were generated by a computerized random-number generator through the block-randomization method of a software program (Excel, Microsoft Office 2007) for sequence generation, and two separate databases were created: a “patients” database, which lists basic information, including patient name, contact details, and so on, and a “randomization” database, which holds data on which patients have been registered on trial along with their allocations. The “patients” database was accessible to any researcher, whereas the “randomization” database was password protected, so that it was accessible only by the principal investigator and a nominated statistician. 27 The assessor, who was the acupuncture practitioner and KRTE supplier, and who was blinded to the allocation results until the end of study, performed the outcome assessment.
KA, Keigai-rengyo-to (KRTE) extract/acupuncture combined treatment; AO, acupuncture only; KO, KRTE only; WL, waiting list group.
After randomization, patients in the AO and KA groups underwent eight sessions of acupuncture treatment twice per week for 4 weeks. Patients in the KO and KA groups were prescribed KRTE 3 times a day after meals for 4 weeks. Patients who were allocated to the WL group did not receive acupuncture or KRTE throughout the 4-week postrandomization period. After 4 weeks, if participants elected to try the acupuncture treatment, it was provided twice weekly for 4 weeks.
Acupuncture was performed by a licensed Oriental medical doctor with 3 years of clinical experience obtained after a 6-year Oriental medical college course. Disposable stainless-steel acupuncture needles (0.25×30 mm; Dongbang Acupuncture, Korea) were used. No specific needle stimulation techniques were used and no specific response was obtained, such as de qi. In order to minimize pain, needles were inserted at a vertical or oblique angle to a depth of 3±2 mm at each acupuncture point in the AO and KA patient groups, and were retained in place for 15 minutes. Papules and nodules were not artificially extruded. Patients received acupuncture at 22 classical acupuncture points and/or ah shi points that were randomly selected at papules and nodules on the face by the acupuncture practitioner. The following 22 classical acupuncture points were treated bilaterally: ST2 (Sibai), ST6 (Jiache), ST36 (Zusanli), LI20 (Yingxiang), LI11 (Quchi), PC6 (Neiguan), HT8 (Shaofu), SP3 (Taibai), SP6 (Sanyinjiao), SP10 (Xuehai), and LR3 (Taichong). These points were selected based on previous studies of acupuncture treatment of acne vulgaris 20 –22 and from the attending doctor's clinical experience. Especially, LI11, LI20, SP6, ST36 and LR3 have been reported as being the most commonly used points in the treatment of facial acne. 20 –22 Participants remained in a supine position throughout each session.
KRTE was purchased from the Han Kook Sin Yak Pharmaceutical Co., which is a Korean good manufacturing practice facility. KRTE is approved by the Korea Food and Drug Administration and is used routinely in clinical practice for treatment of acne, sinusitis, and otitis media. The components of KRTE are shown in Table 3.
KRTE remaining after each session was quantified for enhancement of medication compliance. Participants whose compliance with KTRE was <80% of total dose or who received fewer than six acupuncture sessions were considered to have dropped out.
Outcome measures
Primary outcome was defined as the mean percentage change of inflammatory lesions from baseline to the end of the trial. 25,26 Secondary outcomes included the mean percentage change of noninflammatory lesions from baseline to the end of the trial, count of inflammatory and noninflammatory lesions, quality-of-life scale (Skindex-29), and the investigator global assessment ([IGA]; after evaluation from a score of 1 [very good] to 5 [very poor] every session, outcomes were divided into “improvement” or “nonimprovement” between baseline and the end of the study). Skindex 29 was checked at weeks 0 (baseline) and 4 (end of trial). IGA was checked at every visit, from baseline (just before randomization) through 4 weeks after randomization. A Lumix DMC-LX2 digital camera (Panasonic, Osaka, Japan) was used to photograph each patient's face, so that inflammatory and noninflammatory lesions could be counted at weeks 0 (baseline) and 4 (end of trial).
Monitoring safety
Safety was assessed by the reporting of clinical laboratory tests, vital sign measurements, and adverse events. Clinical laboratory tests, including AST/ALT, BUN/creatinine, red blood cell count, white blood cell count, hemoglobin, hematocrit, mean cell volume, mean cell hemoglobin, mean cell hemoglobin concentration, number of platelets, and number of differentiated cells were determined at weeks 0 (baseline) and 4 (end of trial). An adverse event was defined as any negative event that a patient experienced during the study, including a treatment-emergent adverse event, a new intercurrent illness, or a clinically important abnormal laboratory finding. A treatment-emergent adverse event was defined conservatively as an adverse event not present on the day the study was started or an event present at that time that worsened during treatment. Vital signs of each participant were checked at every session with monitoring of adverse events (pain on the acne lesion or other sites, nausea/vomiting, fatigue, allergic reaction, and any adverse events related to KRTE and acupuncture) after each visit.
Statistical analyses
Analyses were performed using SPSS version 12.0 for Windows based on each of the following principles: (1) an intention-to-treat (ITT) analysis that considered all randomized participants with at least one measurable outcome value during the study, and (2) a per-protocol analysis that included only participants without major protocol deviations. All main analyses were based on the ITT population. End-of-study analyses were performed using the last observation carried forward for patients who did not complete the study. Data are presented as mean±standard deviation. A two-way analysis of covariance (ANCOVA) test was used for examination of the mean percentage change of inflammatory and noninflammatory lesions between baseline and the end of the trial, controlling for age and body mass index (BMI). A repeated measured ANCOVA test, controlling for age and BMI, was used for evaluation of any significant difference in count of inflammatory and noninflammatory lesions, Skindex 29 score, and Visual Analogue Scale score between baseline and the end of the trial. If no statistically significant differences in interaction of KRTE and acupuncture treatment were observed between groups, their main effect was analyzed. According to “improvement” or “no-improvement” of IGA score between baseline and the end of the trial, the difference among the groups was evaluated using a χ 2 test. All differences were considered significant at p<0.05.
Results
Patient disposition and dropout rate
Forty-five (45) participants were recruited and 44 participants were enrolled after screening tests that included a blood test. One (1) participant was excluded for failure to achieve normal AST/ALT blood levels. Of the 44 patients, 34 completed the study protocol. The ratio of group allocation was 1:1:1:1. In the WL, KO, AO, and KA groups, 3, 1, 2, and 4 participants, respectively, dropped out during the study (Fig. 1). The total dropout rate was 22.7%, and higher than a dropout rate of 10%. The two most common reasons for discontinuation were “lost to follow-up” or “personal reason.” More patients dropped out in the WL and KA groups.
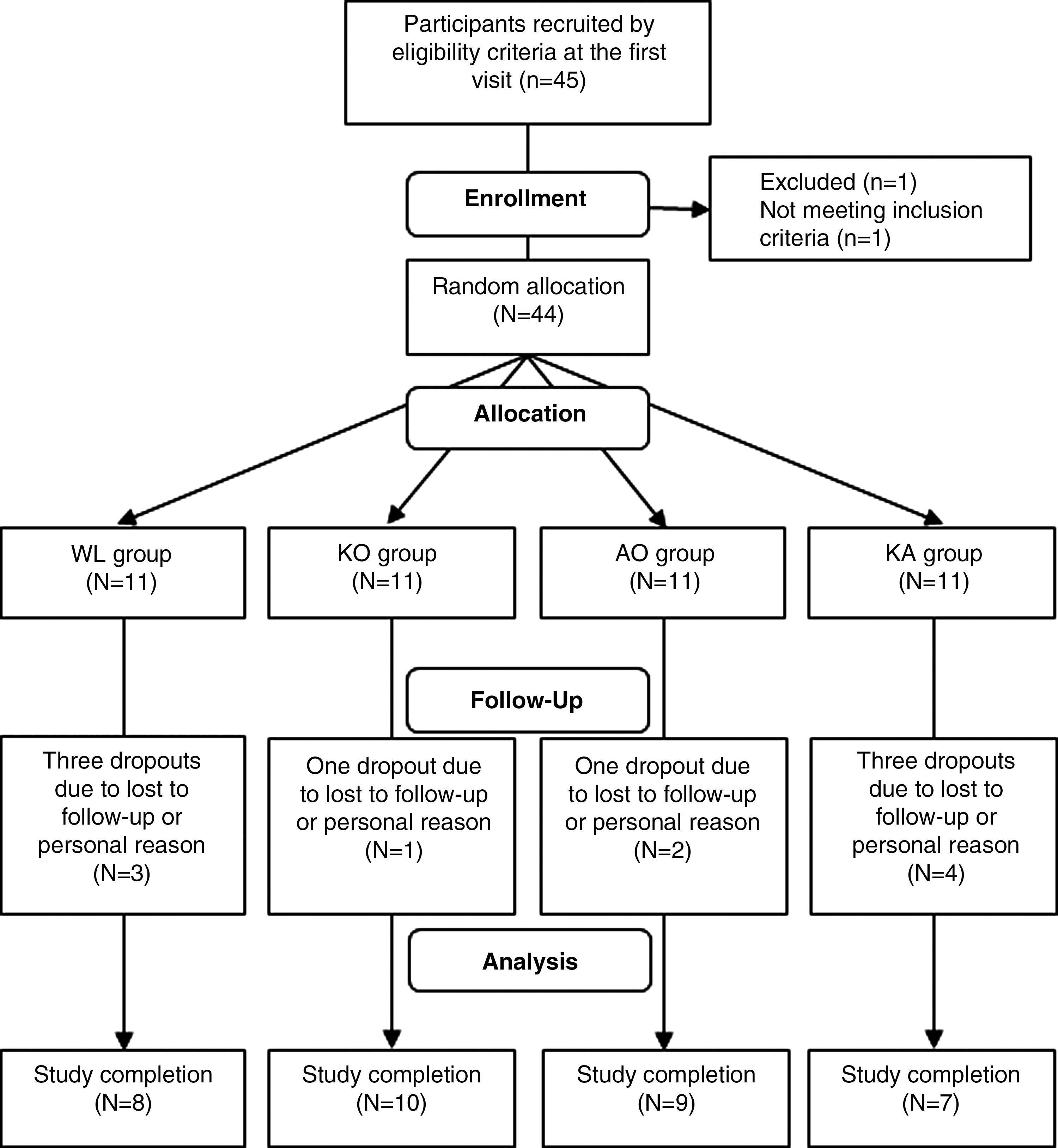
Flow chart of study. WL, waiting-list group; KO, Keigai-rengyo-to only group; AO, acupuncture group; KA, Keigai-rengyo-to plus acupuncture group.
Demographic and Baseline Characteristics
The mean BMI of 44 participants with a mean age of 22.36 years (range: 14–35 years) was 21.53 (score range: 17.67–29.00). The mean duration was 6.22 years (range: 0.8–20.0). Detailed demographic and baseline characteristics of the ITT population are presented in Table 4.
Data are presented as mean±standard deviation.
KRTE, Keigai-rengyo-to extract; BMI, body–mass index; IL, inflammatory lesion; NIL, noninflammatory lesion.
Primary outcome
The primary outcome was the mean percent change of inflammatory acne lesions from baseline to the end of the study in the ITT population. A statistically significant interaction of KRTE and acupuncture was observed (Table 5, Fig. 2).
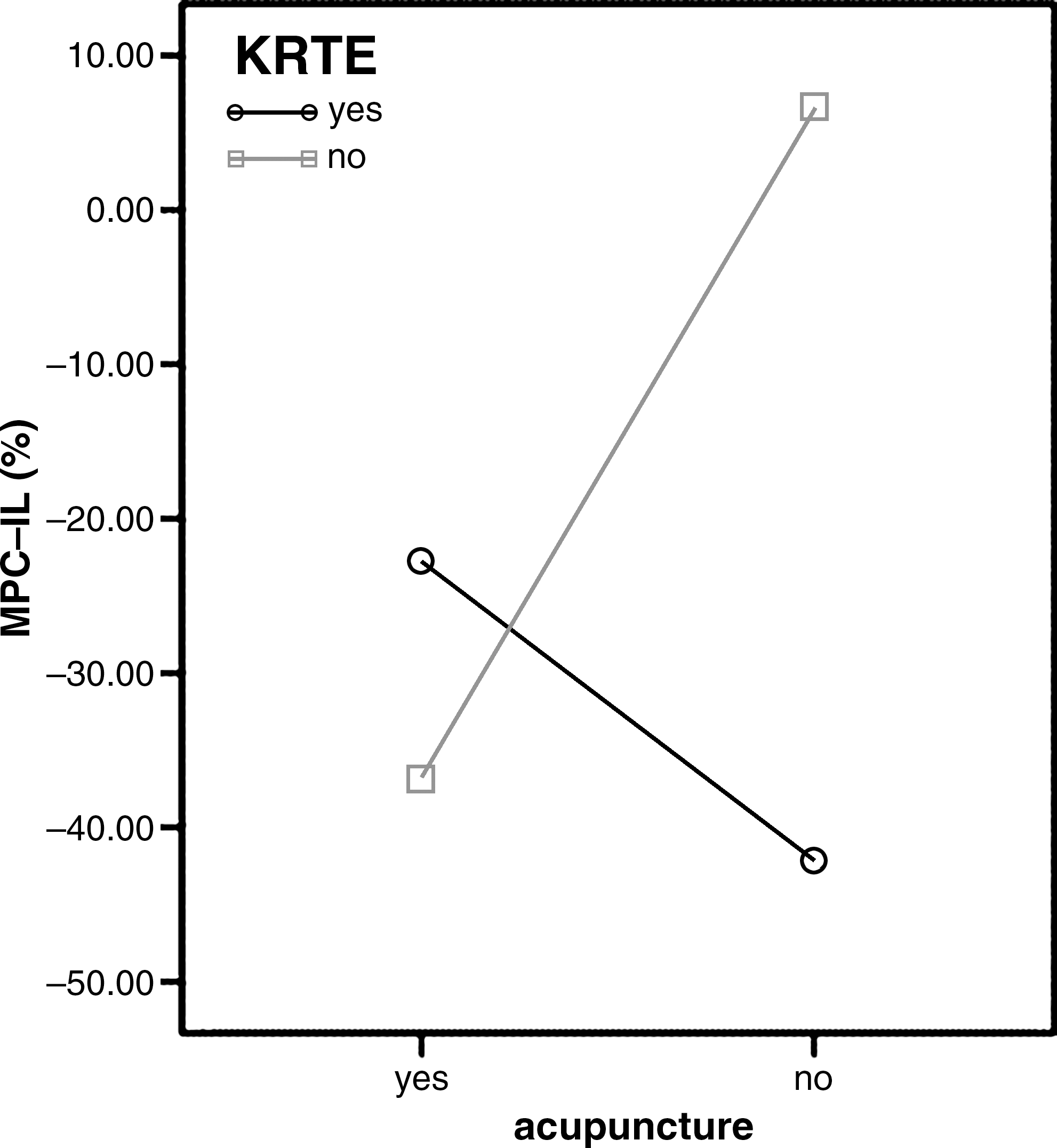
Interaction of mean percent change of inflammatory acne lesions (MPC-IL) from baseline to the end of the study. KRTE, Keigai-rengyo-to extract.
Data are presented as mean±standard deviation of the percent change (95% confidence interval). “Interaction” indicates interaction of Keigai-rengyo-to extract (KRTE) and acupuncture.
Statistically significant interaction, p<0.05 using two-way analysis of covariance test controlling for age and body–mass index.
MPC-IL, mean percent change of inflammatory acne lesions from baseline to the end of the study.
Secondary outcomes
Analysis of the interaction of KRTE and acupuncture in the mean percent change of noninflammatory acne lesions from baseline to the end of the study for the ITT did not reveal a statistically significant interaction of KRTE and acupuncture. A statistically significant difference was evident between KRTE treatment and nontreatment groups. However, no statistically significant difference was observed among acupuncture treatment and nontreatment groups. These findings are summarized in Tables 6 and 7.
Data are presented as mean±standard deviation of the percent change (95% confidence interval). “Interaction” indicates interaction of Keigai-rengyo-to extract (KRTE) and acupuncture.
Statistically significant difference, p<0.05 using two-way analysis of covariance test controlling for age and body–mass index.
MPC-NIL, mean percent change of noninflammatory acne lesions from baseline to the end of the study.
Data are presented as mean±standard deviation. Results from two-way repeated measures analysis of covariance (ANCOVA) test controlling for age and body–mass index (BMI) among the groups. “Interaction” indicates interaction of Keigai-rengyo-to extract (KRTE) and acupuncture.
Statistically significant, as compared with the other groups, p<0.05 using repeated-measures ANCOVA controlling for age and BMI.
IL, inflammatory lesion; (B), baseline; (E), end of study; NIL, noninflammatory lesion.
With regard to the Skindex 29 and counts of inflammatory and noninflammatory acne lesions, no interaction of KRTE and acupuncture, and no statistically significant differences in the between-group analysis were evident. However, a statistical difference was apparent in within-group analysis according to time in the counts of inflammatory and noninflammatory acne lesions. Counts of inflammatory and noninflammatory acne lesions decreased after this trial, especially in patients receiving KRTE (Table 7).
Analysis of the improvement rate according to IGA at the end of the study after 4 weeks in patients with KRTE and acupuncture treatment, compared with patients who did not receive KRTE and acupuncture, demonstrated no significant differences (Table 8).
Based on χ2 test.
KRTE, Keigai-rengyo-to extract.
Safety evaluation
No adverse events were reported. Mean levels in systolic and diastolic blood pressure, respiratory rate, heart rate, and body temperature were similar at all measurement times. Also, clinical laboratory tests were similar between baseline and the end of the trial.
Proportion of compliance with KRTE
The mean rate of compliance with KRTE was 92.3% in the KO and KA groups.
Discussion
In this study, a significant interaction of KRTE and acupuncture according to mean percent change of inflammatory acne lesions was evident from baseline to the end of the study. On the other hand, no interaction of KRTE and acupuncture was apparent according to the mean percent change of noninflammatory acne lesions from baseline to the end of the study, and statistically significant differences were observed for KRTE, but not acupuncture.
KRTE has been officially approved by the Korea Food and Drug Administration for treatment of acne, sinusitis, and otitis media. KRTE is used frequently (usually given orally 3 times after meals, at 7.4 g each dose) due to its high clinical effect and low frequency of side-effects. 8 Previous studies have reported on the benefits of use of KRTE in mucociliary transport in chronic sinusitis, 28 analgesic and anti-inflammatory effect, inhibitory action on carageenin-induced circumscribed edema, and the inhibitory effect of hypersensitivity response. 29 These findings may be relevant to the current anti-inflammatory effect of KRTE in treatment of acne. The anti-inflammatory effectiveness of KTRE in treatment of acne may be due in part to its antioxidant action on infiltrated neutrophils. 23 However, the exact mechanism remains unknown. Finding sufficient evidence to account for the effectiveness of KRTE on noninflammatory acne lesions was difficult.
A number of observations from open studies and randomized trials on the anti-inflammatory actions of acupuncture have been published. Various anti-inflammatory actions of acupuncture based on neutral reflexes and the autonomic nervous system through improvement of local blood circulation, distribution, and bloodletting in inflammatory diseases have been proposed. 30 Assuming that local blood flow is actually stimulated by acupuncture, neurogenic formation of vasoactive mediators could regulate blood flow and blood distribution to affected organs and tissue after inflammation has been initiated. 31 Findings from a previous clinical study of the effect of acupuncture on acne showed an association of acupuncture treatment of moderate acne vulgaris using ah shi point with reduction of inflammatory lesions and improvement of the quality of life. 20 These findings were consistent with the results on the anti-inflammatory effect of acupuncture, but different from the findings in Skindex 29 score representing improvement of quality of life. Mean percentage change in KRTE and acupuncture treatment for 4 weeks was lower than that in western medical treatment with adapalen, benzoyl peroxide, and tazarotene for 12 weeks. 32 However, because these results may be relevant to different duration of each trial, it is difficult to conclude that Western medical treatment with adapalen, benzoyl peroxide, and tazarotene was more effective in acne treatment than Oriental medical treatment with KRTE and acupuncture.
The mean percent change of inflammatory lesions was used as a primary outcome for evaluation of the efficacy and interaction of KRTE and acupuncture in treatment of acne vulgaris in male patients. Classifications of outcome in acne vulgaris are broadly divided into “counts” and “grades,” although the general opinion is that two types of measure are needed by dermatologists: a quick and simple tool for use in the clinic, and a more sensitive measure for use in clinical trials. 33 Therefore, the Korean Acne Grading System was selected in the inclusion criteria of this study because it is a quick and simple tool for use in the clinic, and mean percent change of inflammatory lesions was used as the primary outcome, as a more sensitive measure for use in clinical trials.
Score changes of the adjusted Skindex 29 decreased between baseline and the end of the trial. However, no statistically significant difference was observed within and between groups. In addition, the improvement rate according to IGA at the end of the study after 4 weeks in patients with KRTE and acupuncture treatment, compared with patients who did not receive KRTE and acupuncture, showed no significant difference. These results may be relevant to the short period of this trial.
Participants in this pilot study complied well with taking KRTE. However, the dropout rate was higher than the expected dropout rate of 10% in the WL and KA groups. It is presumed that this result may be due to the fact that participants in the WL group did not receive any treatment during this clinical trial and that participants in the KA group had to undergo both KRTE and acupuncture.
There are several limitations to this study. First, participants were limited to males because females can easily be affected by the level of sex hormones relevant to increased sebum production during the menstrual cycle, which would have occurred during the duration of the trial. Second, because this study was a pilot trial, the sample size was small and the duration of the trial was short, compared with previous studies of acne vulgaris. Third, this study was conducted at a single hospital. Therefore, it is inappropriate to generalize from the results or confirm the efficacy and interaction of KRTE and acupuncture in treatment of acne vulgaris. However, because the data were analyzed using the 2×2 factorial design, an attempt was made to overcome the limitation of small sample size. Therefore, in spite of these limitations, this study could be helpful in providing clinicians with information concerning the efficacy and interaction of KRTE and acupuncture in treatment of acne vulgaris.
Conclusions
In conclusion, use of a combined treatment is recommended that includes both KRTE and acupuncture for inflammatory lesions and KRTE only for noninflammatory lesions for clinicians who want to use KRTE and acupuncture for treatment of acne vulgaris. Further large-scale trials lasting 8–12 weeks, assuming a dropout rate higher than 20%, and aimed at confirming the ability of KRTE and acupuncture to improve inflammatory and noninflammatory lesions in patients with acne are needed.
Footnotes
Acknowledgments
This trial was registered with the Clinical Research Information Service (CRiS), Republic of Korea: KCT0000071. The URL is
Disclosure Statement
No competing financial interests exist.