
Abstract
Background:
Sixty percent (60%) to 80% of patients who visit chiropractic, osteopathic, or Chinese medicine practitioners are seeking pain relief.
Objectives:
This article aimed to identify the amount, quality, and type of complementary and alternative medicine (CAM) pain research in Australia by systematically and critically reviewing the literature.
Methods:
PubMed, Scopus, Australasian Medical Index, and Cochrane library were searched from their inception to July 2009. Australian and New Zealand Clinical Trial Registration and National Health and Medical Research Council databases were searched for human studies yet to be completed. Predefined search terms and selection criteria were used for data identification.
Results:
Of 204 studies selected, 54% were on chiropractic, 27% on Chinese medicine, 15% about multitherapy, and 4% on osteopathy. Chronic spinal pain was the most studied condition, with visceral pain being the least studied. Half of the articles in Chinese medicine or multitherapy were systematic reviews or randomized control trials. In comparison, only 5% of chiropractic and none of osteopathy studies were in these categories. Government funding was rare, and most studies were self-funded or internally funded. All chiropractic, osteopathic, and Chinese herbal medicine studies were conducted by the researchers of the professions. In contrast, half of the acupuncture studies and all t'ai chi studies were conducted by medical doctors or physiotherapists. Multidisciplinary collaboration was uncommon.
Conclusions:
The quantity and the quality of CAM pain research in Australia are inconsistent with the high utilization of the relevant CAM therapies by Australians. A substantial increase in government funding is required. Collaborative research examining the multimodality or multidisciplinary approach is needed.
Introduction
Given the wide use of CAM for pain relief, and the importance of clinical evidence in guiding the population in the use of CAM, in policy-making, and in identifying research direction, it is essential that the level of pain research activities in CAM in Australia be identified.
CAM is referred to as “medical and health care systems, practices, and products that are not generally considered part of conventional medicine,” 7 and consists of a wide range of therapies. The definition of CAM is evolving and fluid. For instance, in Australia, acupuncture is considered a form of CAM, but many medical doctors provide acupuncture treatment and to them it is mainstream even though the National Health and Medical Research Council (NHMRC) considers acupuncture a form of CAM. Spinal manipulation is a key therapy provided by practitioners in physiotherapy, chiropractic, and osteopathy. The former is a form of allied health, whereas the latter two are CAMs.
This review focused on the commonly used CAM for pain relief and the professions that are and will be nationally registered by 2012, namely chiropractic, osteopathy, and Chinese medicine, including Chinese herbal medicine, acupuncture and t'ai chi. These professions have 4–5-year bachelor or master programs at public universities, including RMIT University (RMIT), Victoria University (VU; this program closed at the end of 2009), University of Western Sydney (UWS), University Technology of Sydney (UTS), Macquarie University (Macquarie), and Murdoch University (Murdoch).
Through systematically reviewing existing data, the aim was to identify the types of CAM research in pain in Australia, the background of the researchers, and the funding sources. This review intended neither to assess efficacy or effectiveness of various CAM therapies, nor to examine other areas of CAM research in this country, such as hay fever, cancer or women's health.
Methods
Search methods
PubMed, Scopus, Australasian Medical Index, and Cochrane library were searched from their inception to July 2009 to identify CAM research in pain carried out by Australian researchers. Search terms used were pain, acupuncture, electroacupuncture, dry needling, laser acupuncture, laser therapy, t'ai chi, chiropractic, osteopathy, spinal manipulation, joint mobilization, and herbal medicine. Medical Subject Headings (MeSH) terms were used when possible. Affiliation of the authors was limited to “Australia.” A sample search strategy is included in Appendix 1.
Databases of the Australian and New Zealand Clinical Trial Registration (ANZCTR) and NHMRC were searched for human studies yet to be completed.
Study selection
Included studies had to meet all of the following criteria: (1) one of the authors had to be affiliated with an Australian institution; (2) the study population had to be humans; (3) at least one of the interested professions or interventions was assessed as the main or a component of a combined therapy; (4) the study condition had to be pain or pain related, such as musculoskeletal conditions; and (5) the studies must have been published in a peer-reviewed journal.
Studies about spinal manipulation were only included if the intervention was delivered by a chiropractor or an osteopath practitioner, and were excluded if the therapy was delivered by physiotherapists.
Also excluded were studies examining public usage or opinion about the interested professions, comments, book reviews, letters to the editors, and animal research.
Data extraction and analysis
Data including the author, affiliation, type of research or publication, types of pain, number of participants, source of funding, and journal titles were extracted, and were summarized quantitatively and qualitatively as appropriate. Descriptive data are presented.
Results
A summary of published studies
The search results are illustrated in Figure 1. Two hundred and four (204) out of 716 articles identified met the selection criteria. Nearly one third of studies were identified from PubMed search, one third from the Australasian Medical Index, and the remaining one third from Scopus search.
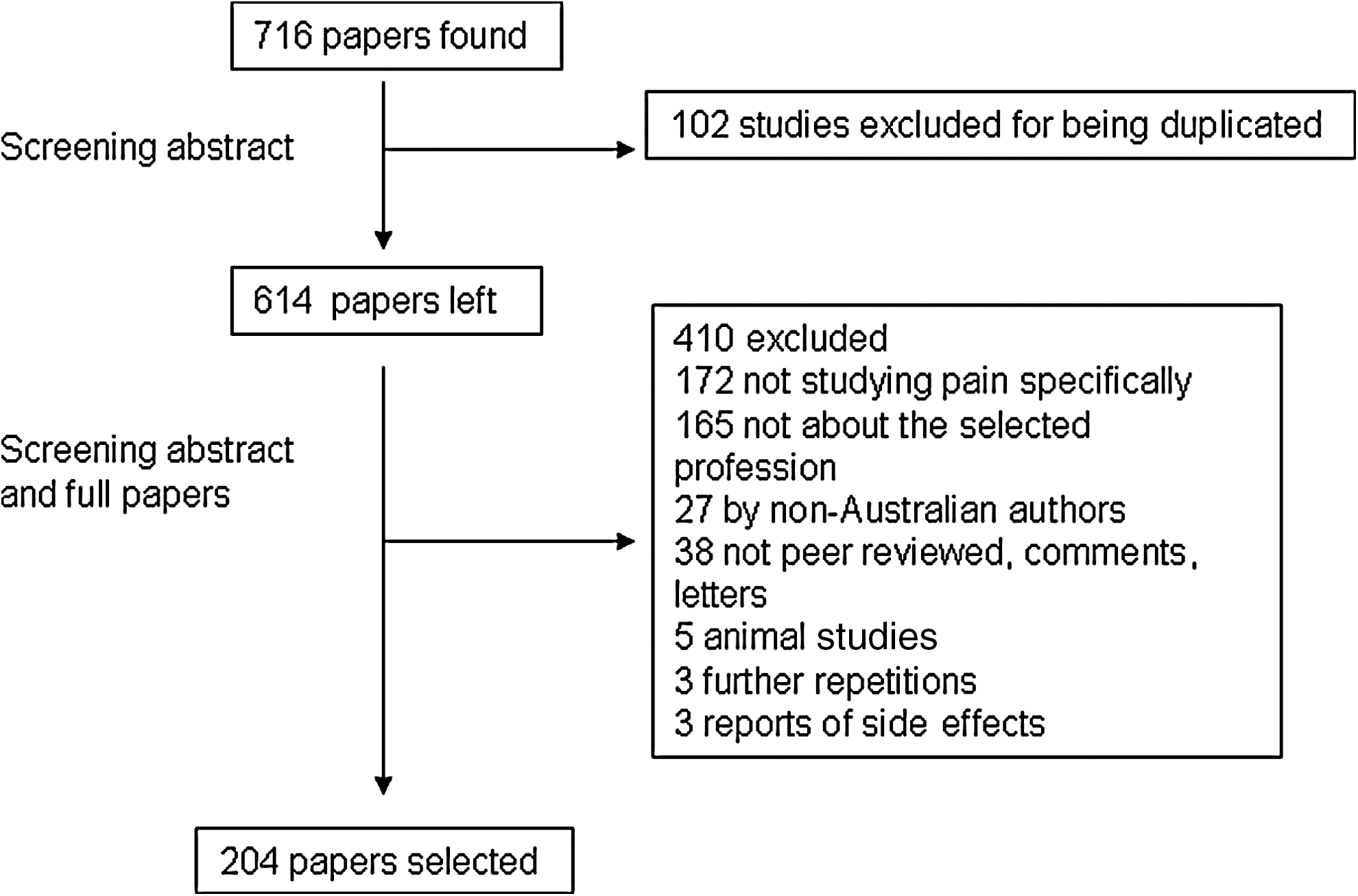
A flowchart of the study selection.
Table 1 summarizes the types of publications within each professional discipline. Data are organized according to whether monotherapy or multitherapy was studied. For instance, a trial comparing acupuncture with sham acupuncture was a monotherapy study. A trial comparing acupuncture with spinal manipulation or a review including all types of complementary therapies were multitherapy. All case reports were considered as monotherapy studies and were allocated to the professional category to which the author(s) belonged.
SR, systematic review; RCT, randomized controlled trial; CT, controlled trial.
Fifty-four percent (54%) of the included studies were about chiropractic, followed by Chinese medicine (27%), and multitherapy (15%). Only eight studies were about osteopathy (4%).
Systematic review (SR) and randomized controlled trials (RCTs) provide a higher level of evidence when compared with case reports and descriptive reviews. 8 Nearly half of the articles on Chinese medicine (47%) and multitherapy (53%) are in the former category. In contrast, only 7% of the studies on chiropractic are in this category, and none in osteopathy.
Within multitherapy studies, three RCTs in this category compared CAM therapies with standard medical treatment, and one compared spinal manipulation delivered by medical doctors or physiotherapists with that by chiropractors. SRs reviewed conservative therapies, noninvasive therapy, all forms of physical interventions and complementary therapies.
Types of pain studied
Table 2 summarizes the types of pain conditions studied. Over half of the studies were on spinal or trunk pain, including neck, thoracic, low back, and chest pain; 15% of location not specified, such as rheumatoid arthritis, widespread pain, fibromyalgia, or “musculoskeletal pain.” More than half of the studies (55%) reviewed did not specify the duration of pain; and nearly a third (31%) were on chronic pain. Visceral and acute pains were not commonly studied.
TTH, tension-type headache.
Details of the SRs and RCTs
SRs or RCTs were conducted by whom, about what, and when?
As illustrated in Table 3, nearly half of 22 SRs and RCTs of acupuncture were conducted by qualified researchers from RMIT, UTS, and VU, and the other half were by medical or physiotherapy researchers from the University of Melbourne (Melbourne), Monash University (Monash), and Queensland University (QU). All RCTs were sham procedure controlled. Two (2) pain studies with Chinese herbal medicine were by researchers from the professions, whereas two t'ai chi studies were by physiotherapists.
See Appendix 2 for references.
CAM, complementary and alternative medicine; RMIT, RMIT University; UTS, University Technology of Sydney; VU, Victoria University; UWS, University of Western Sydney.
Collaborative research was common in Chinese medicine, with 24 out of 26 being co-authored and 16 involved medical doctors, statisticians, physiotherapists, or other CAM professions.
In contrast, all eight SRs and RCTs of chiropractic were conducted by researchers in the field, and only two involved collaboration with other professions. It is interesting to note that the RCTs were not limited to therapies traditionally delivered by chiropractors; electro neuro adaptive regulator, trigger-point therapy, and neuro-emotional technique (NET) were also studied. Four out of six RCTs were sham procedure controlled.
There was no SR or RCT in osteopathy, but two n=1 trials for pain by Australian authors with no collaboration with other professions.
Half of 16 multitherapy studies were first authored by physiotherapists comparing different types of physical therapies. Six (6) were by CAM researchers, including three by chiropractors, two by acupuncturists, and one by osteopath researchers. Eleven (11) out of 16 studies were collaborative research. However, only two of the CAM training universities were involved in any of those studies.
Table 4 shows a surge in SRs and RCTs of CAM in the 2000s. Most of the Chinese medicine or multitherapy studies were published in medical or related journals, whereas studies of chiropractic or osteopathy were often published in their professional journals.
CAM, complementary and alternative medicine.
Overall, all completed RCTs were of relative small sample sizes, varying from 14 to 109 participants per trial, with none of the studies having over 50 participants per intervention group. Two RCT protocols estimated to recruit over 160 participants.
How were SRs or RCTs funded?
Table 5 outlines the types of financial support. A majority of trials did not report the funding sources. Within those reported, a combined internal and external funding was common. External funding sources included governments, commercial or non-commercial industrial, and philanthropic grants. Only three projects were supported by NHMRC grants.
NHMRC, National Health and Medical Research Council.
Registered trials
ANZCTR search resulted in 10 studies (Table 6). The protocols of two trials were published and included in the above-mentioned section. They were excluded from the statistics. Seven (7) out of eight remaining studies were monotherapy, and one was multitherapy examining combined acupuncture and cognitive behavioral therapy for tension headache. Seven (7) trials were registered by institutions offering CAM training. Similar to the published studies, most of the trials were internally or self-funded. No trial was supported by any government funding.
N/R, not rated; LBP, low-back pain; RCT, randomized controlled trial; RMIT, RMIT University; UWS, University of Western Sydney; NET, Neuro-emotional technique; TTH, tension-type headache.
NHMRC and Australian Research Council (ARC)
Available NHMRC data between 2000 and 2008 under “Pain” and “rehabilitation” were summarized. During the period, funding to CAM was below $170,000 until a major increase in 2008 to over $1.5 million. The percentage of funding on CAM of the total annual NHMRC budget improved from 0.003% to 0.27% in 2008. Funding to pain research varied from 1.35% to 2.3% of the total NHMRC annual budget. Within pain research, funding to CAM varied between 0 and 2.07% at best in 2008.
Table 7 lists NHMRC-funded CAM projects on pain starting from 2009. Four (4) out of six projects were on chronic pain, one on acute pain, and the remaining one on experimental pain in rats. In all of them, acupuncture was the study intervention. All projects were collaborative research.
CIA, chief investigator A; RMIT, RMIT University.
No ARC data were available online. The authors contacted the ARC for further data and did not receive any reply.
Discussion
Summary of findings
This article identified inconsistency between Australians' use of CAM for pain relief, the amount of research conducted, and the level of funding. While a high proportion of patients visit Chinese medicine, chiropractic, or osteopathic practitioners for pain relief, high-quality Australian CAM research in pain was not developed until the last decade. Multidisciplinary, collaborative research among CAM and conventional medical professions or allied health practitioners is not common. Furthermore, government funding to pain research in CAM is very small.
In the recently released National Pain Strategy, 9 the high-priority areas are enhancing research and education in all health professions and encouraging interdisciplinary knowledge exchange and multidisciplinary pain management. The findings of this article conform to the proposed priorities.
Possible reasons for a lack of quality CAM pain research in Australia
Internationally, the use of the three CAM in the United States, Germany, and United Kingdom is similar to or more than that in Australia. 10 Those countries produced a large amount of high-quality clinical research, and 185 acupuncture and 22 chiropractic trials on pain were identified through a PubMed search. Similarly, many Chinese herbal medicine studies have been published in China, Korea, and Japan. Results of trials conducted in Asian countries or other Western countries could be useful and relevant to the Australian setting, but need to be validated in this country because of the differences in climate, diet, population, and health care system.
The low number of high-quality CAM research studies in pain could be due to a relatively short history of CAM professions in Australia, research culture, and available funding. Degree courses in these CAM courses offered by Australian public universities only started in the 1980s and 1990s, although formal education had been taught in private colleges, 11 which had less incentive to invest in scientific research.
Within CAM professions, the concept of evidence-based medicine is yet to be embraced. In a qualitative study, none of 42 Australian acupuncturists interviewed used evidence from quality research to inform their decision-making. Some of them felt that efficacy trials did not inform clinical practice. 12 The many case reports, surveys, and reliability studies in chiropractic and osteopathy also indirectly reflect slow adoption of evidence-based medicine by the professions. In addition, not publishing the results of CAM research in mainstream medical journals further reduces the visibility and awareness of CAM studies.
Finally, a lack of funding is evident. In 1980, the Medical Advisory Committee of the NHMRC conducted a review into chiropractic. The report stated a “lack of an adequate body of scientific research” and recommended that “special attention should be given to supporting (chiropractic, osteopathy, homeopathy and naturopathy) research projects in the field of low back pain and other musculoskeletal disorders.” Musculoskeletal conditions incur the highest out-of-pocket expense and are the third most expensive health problem in Australia. 13 Between 1974 and 1991, a few NHMRC inquiries were also made into acupuncture in the area of education, training, practice, and efficacy. In 1975, the council recommended that “controlled clinical trials may be conducted to evaluate the use of acupuncture in…alleviation of pain…treatment of narcotic and alcohol withdrawal states.” 14 Little federal funding was given to pain and CAM research until 2008, 30 years after the initial inquiry.
In comparison, the funding to CAM therapies in the United States is correlated with the cost of illness. From 2000 to 2003 alone, the funding by the National Institute of Health (NIH) to CAM on arthritis and low-back pain, the second and sixth most expensive conditions in the United States, has increased from $3.6 million US dollars to nearly $10 million. 15
Emerging themes and future directions of CAM research in pain
Two (2) emerging themes were identified from this review. First, the boundaries between professions are less clear and new techniques are developed based on theories from other disciplines. Examples of the former are that researchers of some acupuncture and t'ai chi studies are medical doctors and physiotherapists. An example for the latter is NET, a new therapy combining some theory of Chinese medicine and knowledge of neuroanatomy. Such knowledge and practice transmigration will reshape health professions, and its impact on regulation and registration needs to be studied.
Second, multiple modalities are often used by one practitioner, reflecting the reality of pain management, in which multiple therapies and multidisciplinary collaboration are needed and encouraged. 16 Pain patients use a number of therapies. 17 The current study found very few Australian trials comparing therapies head to head and none examining the effect of the combined effect of CAM and other therapy on pain except for two yet-to-be-completed trials.
Multidisciplinary and multimodality pain research require collaboration. Participation of CAM researchers in multitherapy studies was low at 30%. This could lead to questions about content validity of the study intervention. Development of acupuncture research in NIH is a good example of the importance of collaboration. Before the 1990s, less than 10% of investigators of acupuncture projects were acupuncturists. This number has increased to over 90% in 2006, 18 which might lead to high-quality research.
Finally, to maximize the effective translation of clinical evidence of commonly used CAM therapies such as acupuncture, chiropractic, and osteopathy into clinical practice, international multicenter phase III trials with consistent research protocols are needed to ensure the comparability of findings from such studies.
Conclusions
In Australia, the use of CAM therapies for pain relief is high. Research quality in the CAM area needs to be improved considerably, and a substantial increase in government funding is required to assess the safety and efficacy of the CAM therapies. Future research needs to involve CAM researchers and practitioners as well as researchers from other health research backgrounds, and should examine the combined effect of multiple therapies. International multicenter phase III studies will facilitate the translation of research evidence into practice.
Footnotes
Acknowledgments
The preparation of this article is partially supported by a National Health and Medical Research Council project grant (No. 555411).
Disclosure Statement
No competing financial interests exist.