
Abstract
Background:
Over the past decade, interest in complementary therapies and alternative medicine has escalated among midwives and the general public in response to increased demand from expectant mothers for more choice, control, and continuity in labor.
Objective:
The aim of this study was to explore if an aromatherapy and massage intrapartum service (AMIS) reduced the need for analgesia during labor. This article reports results related to the effects of an AMIS on type of analgesia chosen by women in labor, and on rates of anesthesia—one aspect of the full study.
Setting/location:
The study was conducted in a general maternity unit in southwest England, UK.
Design:
A quantitative research approach was taken, whereby contemporaneously completed service evaluation forms of 1079 women (601 nulliparous women and 478 multiparous women; AMIS group) were retrospectively analyzed in comparison with the birth records of an equal number of similar women (comparison group). Data analysis was achieved by entering data from the forms and comparison sample into an SPSS package and running statistical tests.
Results:
In the AMIS group, overall analgesia usage was higher for transcutaneous electrical stimulation at 34%, compared with 15.9% (p<0.001 allowing for parity), and for nitrous oxide and oxygen at 87.6%, compared with 80.8% (p<0.001). Pethidine use did not differ after adjustment for parity at 30.1%, compared with 24.2% (p=0.27) in the AMIS and comparison groups, respectively. Rates were lower in the AMIS group for epidural anesthesia at 29.7%, compared with 33.8% (p=0.004 allowing for parity) in the comparison group; spinal anesthesia at 6%; compared with 12.1% (p<0.001) in the comparison group; and general anesthesia at 0.8%, compared with 2.3% (p=0.033) in the comparison group.
Conclusions:
Having an AMIS appears to have a positive impact on reducing rates of all types of intrapartum anesthesia. The Service is a beneficial addition to conventional midwifery practice that may influence mode of delivery and reduce general anesthesia rates.
Introduction
Bodecker et al. 4 have identified how, over the past decade, interest in complementary and alternative medicine (CAM) has escalated among midwives and the general public. Incorporating CAM into health care settings provides a more holistic approach that not only cares for the body but also tends to the mind, spirit, and the environment the person is in. After reviewing literature regarding the use of CAM within the maternity arena, it became evident that an increasing number of maternity units in the United Kingdom are developing CAM services for women during pregnancy and labor in order to offer a wider provision of care with a more naturalistic, individualized option. Conventional care in the United Kingdom offers analgesia such as transcutaneous electrical nerve stimulation (TENS) entonox, pethidine or diamorphine, and epidural anesthesia.
There is a dearth of credible experimental research about the effectiveness of CAM use in pregnancy and labor. However, according to anecdotal evidence, the benefits are thought to include increased choice of coping mechanisms in labor with a more naturalistic option 5 ; improved continuity of care as the midwife spends longer with the woman, which is known to be a critical component for achieving improved birth outcomes 6,7 ; and a possible reduction in medical intervention as well as possible reductions in labor duration and perception of pain. 8 –11 There may also be fewer episodes of nausea and vomiting, headaches, hypertension, and pyrexia. 8
It has been 3 years since the AMIS was launched at the study site, and comprehensive documentation forms for all women who have used the Service have been maintained. These forms were used to record each women's personal details, medical history, intrapartum events, and delivery outcomes.
This article reports on the part of the study concerned with the impact of the AMIS upon analgesia types and rates given to women in labor.
Methods
The full study was performed to identify comparisons between two samples of women who had given birth in one maternity unit since 2007.
The feasibility of conducting a randomized controlled trial was considered, with the intention of examining the effects of the AMIS and making comparisons with a control group. However it was recognised that pregnant women and women in labor are particularly vulnerable (with diminished autonomy who deserve greater protection of their rights) for subjects of research, 12 –14 and to randomize such women to an intervention group could be considered unethical. Therefore, data were collected contemporaneously, using evaluation forms from the AMIS group. The form requested clinical information including name, hospital number, age, ethnicity, parity, gestation, preexisting medical conditions, and pregnancy complications. The clinical details and labor outcomes following the intervention of aromatherapy and massage, were examined. Details about which essential oils were used and how they were administered were also included on the form as were labor and delivery details and outcomes. These were all dependent variables that were identified in a literature review as possibly being affected by use of aromatherapy and massage in labor.
The AMIS sample comprised 1079 records, 601 of which were from nulliparous women and 478 multiparous women. These records were taken from the first women who received the AMIS since the service was launched in July 2007.
Clinical data of women who had not used the AMIS were accessed via mandatory computerized data that represented a comparison group. This enabled comparisons between the clinical details and labor outcomes of the AMIS and comparison groups.
Every woman who gives birth in the local maternity unit has comprehensive pregnancy, labor, and delivery records entered onto a computer system. This computer system enables labor and delivery statistics to be retrieved and filtered. Anonymized data of all women who had given birth between July 2007 and July 2010, and who had not used the AMIS were retrieved (5500 records). This was the period of data collection for both intervention and control groups.
To obtain a similar size sample to the AMIS group, the records of every fifth person in the computerized data were obtained. Women were excluded from both sample groups if they had preexisting medical conditions, previous uterine surgery, or contraindications to certain essential oils.
The sample size for the AMIS and comparison groups was 1079 each, with a total sample size 2158. Stratification was use to ensure that both groups contained the same proportions of nulliparous and multiparous women; the goal of stratification was to achieve a greater degree of comparability, as it is widely recognized that labor and delivery outcomes of nulliparous and multiparous women vary greatly. 11 The parity breakdown of these samples was 56% (n=601) nulliparous women and 44% (n=478) multiparous women.
Data of particular aromatherapy oils used by the 1079 women, included in the AMIS sample, were collected to explore which oils were most popular and to ascertain if any specific oil appeared to be particularly effective or was viewed as being helpful by the women or midwives. The seven aromatherapy oils available and their uses are listed in Table 1.
Latin binomials are: bergamot Monarda didyma; clary sage, Salvia sclarea; frankincense, Boswellia spp.; jasmine;
Statistical software (SPSS) was used to analyze the data. SPSS requires a codebook approach, whereby defining and labeling each variable and assigning numbers to each possible response are performed. 15 All 2158 records were inputted by the first author of this article to ensure consistency in the approach used. Maimon and Rokach 16 explain how data entry and acquisition is prone to errors; therefore, after all data had been inputted, a process of data cleansing took place. 17,18
The aim was to gather data from the AMIS and comparison groups and identify the differences between these samples. Independent sample t-tests between the groups were conducted for numerical variables, and chi-square tests were undertaken for categorical variables. Logistic regression was used to estimate the effects of AMIS versus no AMIS on use of analgesia and anesthesia, and on mode of delivery, while allowing for the effects of parity, which are known to influence these variables.
Motulsky 19 advises setting a threshold p-value before conducting research based on the relative consequences of missing a true difference or falsely finding a difference. The threshold value was set to p=0.05.
Approval was obtained from a National Health Service (NHS) research ethics committee, which concluded that the study was evaluative in nature and posed no risks to women, as only their anonymized data were required. Approval for the study to proceed was also obtained from the NHS Trust's Head of Midwifery and Medical Director.
One of the prime ethical considerations for this study was that data were taken from a clinical record documentation form and an NHS birth database. Both contain confidential information regarding individual women's ages, parities, medical and pregnancy histories, labor and delivery information, usage of the service, and personal comments. The forms and the extracted records from the computerized birth database were anonymized prior to entry into SPSS.
Results
The mean age of women in the AMIS group was 30.43 with a standard deviation (SD) of 6.05, compared with a mean age of 29.86 in the comparison group and an SD of 6.08. The mean gestational age of women included in the AMIS sample was 40.04 weeks with an SD of 2.15. This was compared with a mean gestational age of 39.72 weeks in the comparison group with an SD of 1.65. Classification of ethnicity for this study was in accordance with the U.K. National Statistics Classification for Ethnic Groups developed by the Office for National Statistics in 2001. The majority of women in both the AMIS and the comparison Groups were in the White British or Mixed British category (AMIS: 91.8% [n=967]; comparison group: 93.2% [n=988]).
Up to three aromatherapy oils could be blended and used together. Bergamot (Monarda didyma) and frankincense (Boswellia spp.) oil were the most used oils and rose (Rosa spp.) oil was the least used. Figure 1 represents a breakdown of popularity of individual aromatherapy oils and the number of women in the AMIS sample who used each oil.
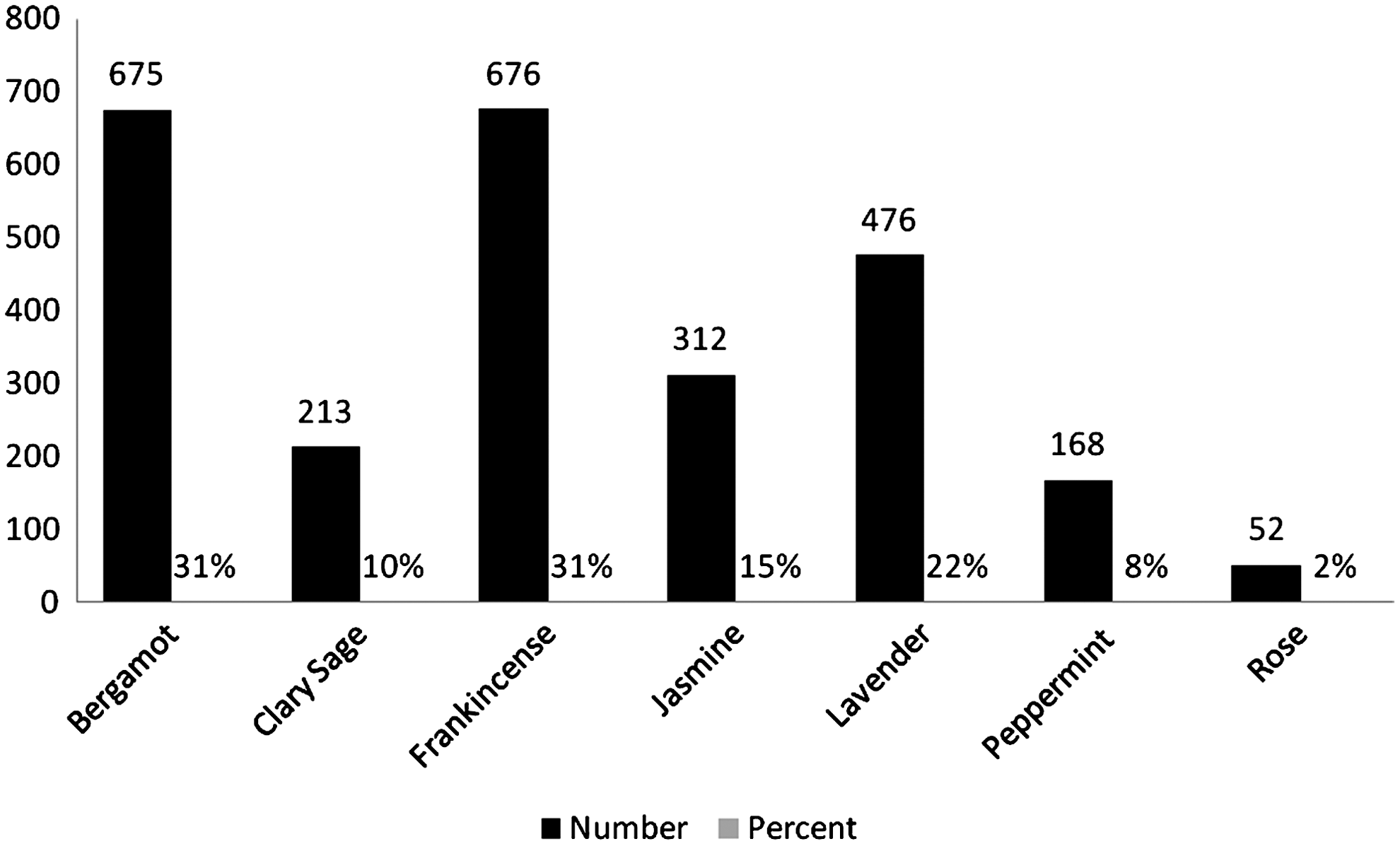
Number of women who used each aromatherapy oil. Latin binomials are: bergamot Monarda didyma; clary sage, Salvia sclarea; frankincense, Boswellia spp.; jasmine; Jasminum sambac; lavender, Lavendula spp.; peppermint; Mentha×piperita; and rose, Rosa spp.
Mode of application was measured to ascertain how mothers and midwives preferred to use the oils and to identify if mode of application affected how helpful the oils were. The most popular method of administration was massage. Twenty six percent (26%; n=257) had massage alone and 24.3% (n=245) had massage as well as another form of application. Taper application (oil dropped onto an absorbent paper strip) was also very popular, with 36.4% (n=367) of the sample population having the aromatherapy oils administered by tapers. Figure 2 represents mode of application of the aromatherapy oils for the sample population. Fifty percent (50%) of women received aromatherapy oils via massage.
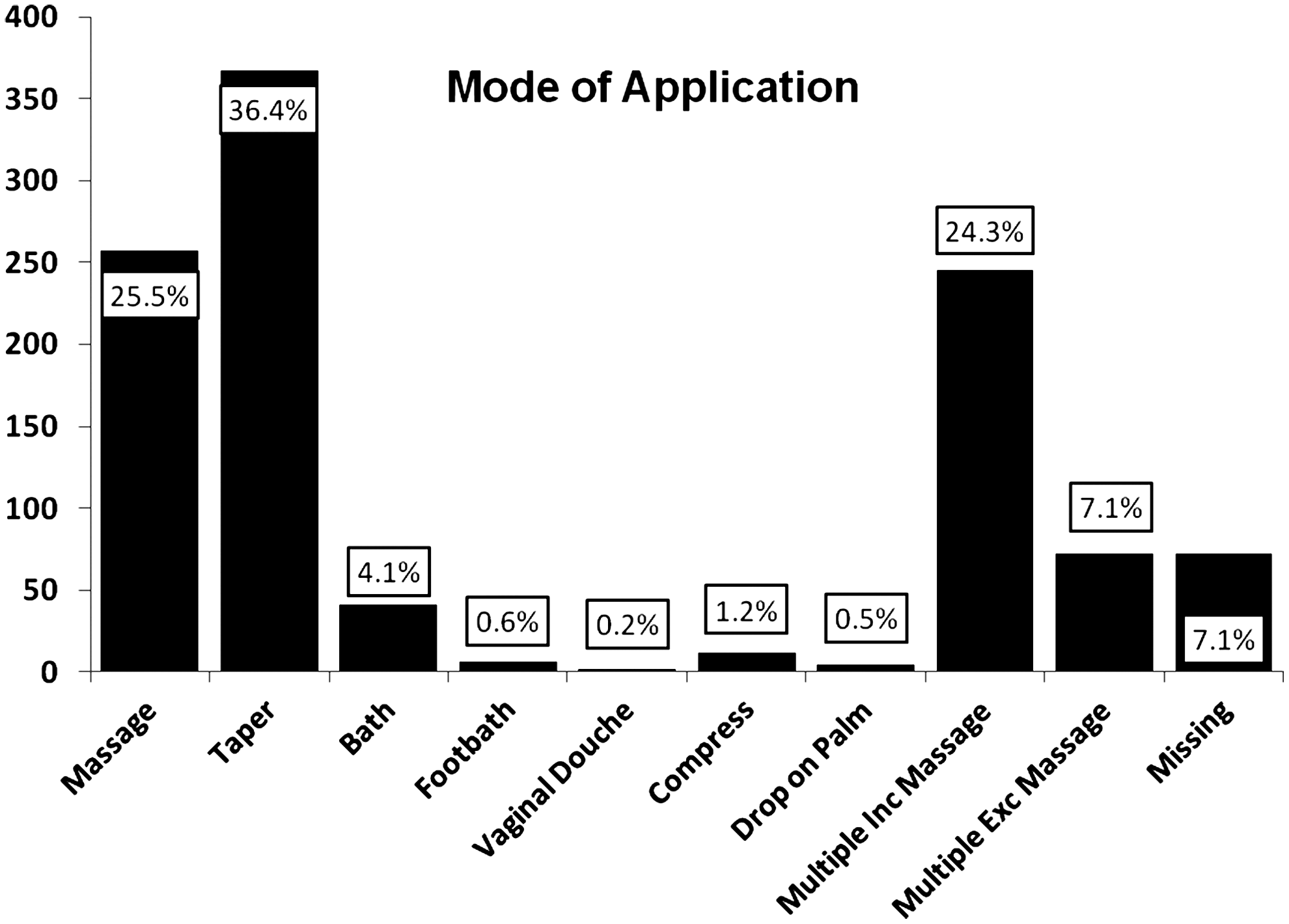
Mode of application of aromatherapy oils.
There were three main reasons for using the AMIS: (1) To help relax and calm women in labor (2) To provide a naturalistic option to pain relief (3) To help enhance contractions.
These data are presented in Table 2. The aromatherapy oils may have been selected and combined to serve more than one purpose.
Three modes of analgesia and three modes of anesthesia were compared in this study. The analgesia modes were: TENS machine; nitrous oxide (NO) 50% and oxygen 50% (entonox); and pethidine. The anesthesia modes were: epidural; spinal anesthesia; and general anesthesia. Table 3 shows a comparison of analgesia and anesthesia used in labor for the AMIS and comparison croups. Results of the logistic regressions are shown in Table 4.
TENS, transcutaneous electrical stimulation; AMIS, aromatherapy and massage intrapartum service.
AMIS, aromatherapy and massage intrapartum service, TENS, transcutaneous electrical stimulation.
Use of a TENS machine in labor was higher in the AMIS Group (34%, compared with 15.9% in the comparison group); the difference in use was seen in both nulliparas (41%, compared with 19%) and multiparas (26%, compared with 13%). TENS use was statistically significantly more likely (p<0.001) in the AMIS than in the comparison group after adjustment for parity.
Use of NO and oxygen (entonox) was higher in the AMIS group (88%) than in the comparison group (81%) (nulliparas: 88% versus 80%; multiparas: 87% versus 82%). Entonox use was statistically significantly more likely (p<0.001) in the AMIS than in the comparison group after adjustment for parity.
For pethidine, overall comparison revealed that 30% of the AMIS group received pethidine during labor, compared to 24% in the CG (nulliparas: 34% versus 31%; multiparas: 26% versus 16%). After adjustment for parity, pethidine use did not differ significantly in the AMIS or comparison groups (p=0.27).
An overall comparison of epidural use between the AMIS and comparison groups revealed lower use in the AMIS group (30% versus 34% in the comparison group; nulliparous: 39% versus 48%; multiparous: 18% versus 16%). Epidural use was statistically significantly less likely (p=0.004) in the AMIS than in the comparison grou after adjustment for parity.
An overall comparison of spinal anesthesia use during labor revealed lower use of spinal anesthesia in the AMIS group (6% compared with 12% in the CG; nulliparas: 8% versus 15%; multiparas: 3% versus 8%). Spinal anesthesia use was statistically significantly less likely (p<0.001) in the AMIS than in the comparison group after adjustment for parity.
An overall comparison of general anesthesia intrapartum use revealed that general anesthia was used less in the AMIS group (0.8% compared with 2.3% in the CG; nulliparas: 1.2% versus 3.0%; multiparas; 0.4% versus 1.5%). General anesthesia use was statistically significantly less likely (p=0.033) in the AMIS than in the comparison group after adjustment for parity.
Onset of labor for the majority of women in the AMIS and comparison groups was spontaneous: AMIS 77% compared with comparison group 74% (nulliparas: 73% versus 75%; multiparas: 76% versus 79%). This difference was not statistically significant (p=0.30 after adjustment for parity).
Discussion
The experience of labor pain differs among women, and the response to pain is highly individual. 20 It is interesting to consider why this might be. Alehagen et al. 21 explained how labor discomfort is thought to arise from the fear of the unknown, which leads to sympathetic arousal, producing tension in the circular fibers of the uterus and rigidity at the opening of the cervix. Field et al. 22 elaborated that this force acts against the expulsive muscle fibers in labor, producing tension within the uterine cavity, which is interpreted by the laboring mother as pain; therefore, it is suggested that women who are particularly fearful of labor may have increased pain. Zwelling 23 states that excessive anxiety in labor produces increased catecholamine secretion that may actually increase pain perception in the brain and decrease uterine contractions by blocking the release of oxytocin from the posterior pituitary. The current study showed that one of the main reasons for using the aromatherapy and massage was to reduce fear and anxiety; therefore; it is likely that, when midwives perceive a woman to be particularly anxious or frightened, they would have offered the AMIS. Such anxious and frightened women, who may struggle with the pain of labor, are therefore perhaps predisposed to being offered the AMIS, as the midwife will perceive the service will be of greatest benefit to these women. In addition, because of the chemical physiology of anxiety increasing pain, these women perhaps, subsequently would have increased pharmacologic requirements, increasing their need for pethidine.
One of the main aims of the current study was to explore if using the AMIS reduced use of pharmacologic analgesia and anesthesia. In addition to pharmacologic modes of analgesia are TENS machines, which are commonly used as a naturalistic, nonpharmaceutical option. 24
The Gate Control Theory suggests that stimulation of larger peripheral nerve fibers inhibits pain signals entering the central pain pathway, reducing perception of pain—TENS provides this stimulation; in additional, it is believed that the electrical stimulation also activates the release of the body's own endorphins. 24 As TENS is a nonpharmacologic analgesic that allows women to mobilize with no known side-effects to the mother and fetus, it is a popular choice. Women in the AMIS group had a significantly higher usage rate of TENS than women in the comparison group.
It may be that women who choose TENS are more likely to want a more natural birth and, therefore, would be more likely to use essential oils in preference to pharmacologic analgesia. This may also account for the epidural rate being significantly lower in the AMIS group. The midwife may also influence choice of analgesia, and those promoting aromatherapy and massage may be keen to avoid pharmacologic analgesia if possible.
Entonox acts as an effective analgesic when it is inhaled, can be used during all stages of labor, and has no known effects on the fetus. 24 Entonox is often a first-option analgesia offered to women in labor and is extremely fast-acting and easy to self-administer making it a popular choice for midwives to offer. 25 The use of entonox was significantly higher in the AMIS group, but our records do not account for the amount used, because this is not possible to assess. The increased use of entonox may have been a contributory factor to the reduction in the epidural rates in this group. In future, it would be interesting to record recommendations and dialogue between women and midwives about analgesia and the considerations upon which decisions are made.
Although entonox is a pharmacologic substance, it is not accumulative and has a short life in the body (excreted from the body after 2–5 minutes and does not cross the placenta), 26 this agent is considered a fairly naturalistic option for analgesia. 24 Etenox does not have the side-effects and long-term complications of other anxiolytic drugs used for labor. 27 Similar to the explanation for increased TENS usage, many women like to avoid pharmacologic or invasive methods of pain relief during labor, 28 and it may be that women who keen on avoiding pharmacologic drugs during labor (which can affect the baby) will, instead, opt for low-risk analgesia, such as entonox together with the AMIS. In a study conducted by Tate, 29 postoperative use of peppermint (Mentha×piperita) aromatherapy reduced the need for conventional antiemetics, and participants received and tolerated more opioid analgesia postoperatively (p=0.02). This explanation may also account for why entonox rates were higher in the AMIS group.
Pethidine is a synthetic phenylpiperdine derivative that is commonly administered intramuscularly during labor. 30 Pethidine is well known to cross the placenta and has been shown to make babies sleepier, less attentive, and less able to begin breastfeeding. Despite these well-documented effects, since 1947, pethidine has been the most widely systemically used opioid for relieving pain during childbirth. 31 Contrary to Burns et al.'s 8 finding that the use of systemic opioids was greatly reduced with the use of aromatherapy and massage in labor (6% in 1990 reduced to 0.4% in 1997), the current study found that the use of pethidine did not differ overall between the AMIS and comparison groups, and, in the multiparas, use was higher in the AMIS group.
The possible reasons for this were explored with a group of midwives, and it was suggested that, if women had received pethidine during their first labor and liked the agent's effects, they might opt for it again. Nilsson and Lundgren 32 explained that previous birth experience is central to shaping subsequent labor and birth choices. The other significant feature between nulliparous and multiparous women's labor is that multiparas' labor and births are usually quicker and less complicated than those of nulliparas. 33 It, therefore, could be the case that pethidine usage was higher in multiparas with a subsequent lower epidural rate, as there was not enough time to get an epidural inserted.
It could be argued that, while pethidine has known effects, its method of administration is less-invasive than that of an epidural, still enables mobilization, and does not increase likelihood of instrumental delivery in the way that epidurals do. 24
Greulich and Tarrant 34 explained why both pethidine and aromatherapy are often used as relief measures during the latent phase of labor, when women have not yet met the criteria of being able to have entonox or an epidural.
Conclusions
Use of TENS, entonox and pethidine was higher in the AMIS group possibly because these women chose to have less-invasive modes of analgesia.
It should be acknowledged that the AMIS group had significantly lower incidences of epidural, spinal, and general anesthesia. However, when there are more normal deliveries and less instrumental and operative deliveries, inevitably, anesthesia rates will be lower.
Women who have epidurals during labor are more likely to have longer second stages of labor, have an increased need for syntocinon augmentation, experience hypotension, have an increased risk of an instrumental delivery, are unable to mobilize during labor or for a period of time after birth, and are more likely to have postnatal urinary concerns and fever. 35 The physiologic, psychologic, and financial benefits of reducing these risks are apparent.
When administering a general anesthetic to pregnant or laboring women, there are well-known increased difficulties in intubating and ventilating. 36 There is also an increased incidence of gastric aspiration for pregnant women having general anesthetics, and a risk of the anaesthetic drugs crossing the placenta to the baby and depressing breathing in the baby 37 and blood loss are also increased. In addition, if mother has a general anesthetic during birth she is consequently not able to enjoy the moment of birth 38 ; this has been associated with having a negative influence upon mother and baby bonding, and may affect the establishment of breastfeeding negatively. Therefore, any measure to reduce the likelihood of a mother needing a general anesthetic is beneficial.
The financial equability of having the AMIS service in place has been acknowledged by considering the approximate annual cost of running this service calculated from invoices for a financial year (April 2009 to April 2010; Table 5). To put this into context, a year's supply of aromatherapy and massage oils costs $519.53 the center in which this research was conducted and where there are 3000 births per year. TENS machines are not typically supplied by the NHS and, therefore, have no cost implication—women often bring in their own machines, so the cost is borne by the patients. The potential for reduction in general anesthesia and epidurals might, in the long term, reduce anesthetic workload. In addition, recovery time, nursing time, the cost of anesthetic agents, and the risk of adverse events might decrease.
Latin binomials for plants are: bergamot Monarda didyma; clary sage, Salvia sclarea; frankincense, Boswellia spp.; jasmine;
AMIS, aromatherapy and massage intrapartum service; UK, United Kingdom.
Based on this information, the use of the AMIS is inexpensive and may have the potential for significant savings.
Despite the methodological limitations of conducting a retrospective case analysis rather than a prospective trial, the current authors considered the sample size of women included in this study to be adequate to provide results providing a good indication that the AMIS is of benefit.
The analysis showed that having an AMIS appears to have a positive impact in reducing anesthesia during labor, which, in turn, has the potential to improve maternal and neonatal outcomes.
In future, research is needed to identify the impact of extraneous variables, such as the preferences and influences of midwives for pain relief choices made by women in labor.
Footnotes
Acknowledgments
The authors would like to thank Lesley Lockyer, PhD, BSc (Hons), RN, and Abby Sabey, MSc, BSc, PGCE, for their contribution to the statistical analyses in this study.
Disclosure Statement
No competing financial interests exist.