
Abstract
Objectives:
Current psychotropic medications for childhood bipolar spectrum disorders (BPSD) are associated with significant adverse events. As nutrients play an important role in physical and mental health, they may be useful in treating mood disorders with few side-effects. This open-label study explored the feasibility of testing therapeutic effects of a multinutrient supplement, EMPowerplus™ (EMP+), for pediatric BPSD.
Design:
EMP+ was started at one capsule t.i.d. and escalated to a goal of four capsules t.i.d., which eight children attained. Four (4) of these increased to the maximum dose, five capsules t.i.d. Mood symptoms were assessed seven times over 8 weeks.
Subjects:
Ten (10) children, age 6–12 with BPSD, were enrolled in 6.5 months. Seven (7) participants completed the full trial. Three (3) dropped out due to palatability and/or adherence issues.
Results:
Mean medication adherence was 91%. With one-tailed nonparametric Fisher's randomization tests, intent-to-treat analyses demonstrated a 37% decrease in depression scores (p<0.06) and a 45% decrease in mania scores (p<0.01) from the start of treatment through final visit, suggesting improvement and possible treatment response. Study completers demonstrated significant decreasing trends in both depression and mania scores from baseline to final visit (p<0.05). Side-effects were minor and transient, mostly temporary gastric discomfort.
Conclusions:
Future randomized, placebo-controlled trials of EMP+ are warranted and feasible.
Introduction
Childhood BPSD are associated with impairing symptoms of labile mood, chronic irritability, high reactivity, hyperarousal, and aggressive behavior. 3 Research suggests that children who display clinically elevated levels of attention problems, aggression, and anxious–depressed symptoms on the Child Behavior Checklist may be considered at high risk for a bipolar spectrum disorder and chronic, severe mood dysregulation symptoms as well as psychosocial impairment. 4 Children with BPSD may show high recurrence rates and mood fluctuations resistant to treatment. Those diagnosed at earlier ages tend to have greater psychosocial impairment and less response to treatment. In addition, children with BPSD are often diagnosed with more than one comorbid condition that may further impair global functioning. 3
Treatment literature is lacking for children with BP-II, BP-NOS, and cyclothymia, despite the functional impairment inherent to these diagnoses. Pharmacologic interventions have focused on BP-I, 1 and those found efficacious are often associated with adverse events. 5 Recent research on aripiprazole, olanzapine, quetiapine, and risperidone in youth showed significant weight gain for each medication after 12 weeks compared to no treatment, significant increases in mean levels of total cholesterol, triglycerides, non-high-density lipoprotein (non-HDL) cholesterol, and triglyceride-to-HDL-cholesterol ratio with olanzapine and quetiapine, and significantly higher triglyceride levels with risperidone treatment. 6 In another study monitoring side-effects of clozapine, olanzapine, and risperidone in 51 adolescent inpatients with various psychiatric diagnoses, all three atypical neuroleptics caused drowsiness and hypoactivity, 30%–60% of adolescents taking clozapine experienced constipation, increased salivation, orthostatic hypotension, and nasal congestion, and 5%–15% of participants taking olanzapine or risperidone suffered from rigidity, tremor, and dystonia. Participants in all three atypical neuroleptic conditions gained weight during the study; those in the olanzapine group gained significantly more than those in the other two treatment groups (4.6±1.9 kg). 7 Additionally, a recent study of an anticonvulsant mood stabilizer in children failed to show any superiority to placebo, 8 and recent clinical trials of mood disorders in youth show that approximately 20%–25% of participants dropped out of psychotropic medication treatment. 9,10 BPSD in children represent a significant public health concern, yet relatively few clinical trials have been conducted and treatments with demonstrated safety and efficacy are lacking.
Dietary Supplementation and Mental Health
There is great need for pediatric BPSD treatments that demonstrate efficacy without the potentially serious side-effects related to many contemporary psychotropic treatments. Increasing evidence suggests that nutrition affects the structure and functioning of the brain due to the high percentage of human metabolic activity accounted for by this organ. 11 One (1) longitudinal study shows that children with signs of malnutrition at age 3 grow up to be more aggressive, hyperactive, and have more externalizing problems at age 11 as well as excessive motor activity and higher rates of conduct disorder by age 17. 12 These researchers found that a greater degree of malnutrition at age 3 led to a greater degree of externalizing problems at ages 8 and 17. This relationship was mediated by low IQ, suggesting that malnutrition creates a vulnerability to neurocognitive deficits, leading to externalizing behavior problems in youth. The authors suggest that improving early childhood nutrition may help reduce behavioral problems in later years. 12
Other research on diet and nutrition suggests the possibility that micronutrient supplements may have a beneficial effect on mood, which might provide either a primary or adjunctive treatment with a more favorable risk–benefit ratio for children suffering from BPSD than currently available pharmacologic interventions. 13 In particular, multi-ingredient supplements need further scientific study based on the theory that if one nutrient is deficient, a grouping of nutrients is likely deficient, and the level of one nutrient can affect the adequacy of others. 11,13
The micronutrient supplement used in this pilot study is EMPowerplus™ (EMP+; Truehope Nutritional Support Ltd., Raymond, Alberta, Canada;
Materials and Methods
This open-label study explored the feasibility of a randomized clinical trial testing possible therapeutic effects of EMP+ in 10 children with BPSD. Hypotheses were as follows: (1) the sample can be recruited in 5 months; (2) children aged 6–12 can swallow the supplement with >80% adherence; (3) depression scores will show a decreasing trend over the course of supplement treatment; and (4) mania scores will show a decreasing trend over the course of supplement treatment.
Participants
Eleven (11) children were screened and 10 children aged 6–12 years old with BPSD participated in this open-label trial. One (1) child screened did not meet symptom criteria to participate, resulting in a sample size of 10 children. Participants were recruited through continuous enrollment over a 6.5-month period during the school year. Seven (7) inclusion criteria were required: (1) be aged 6–12 years; (2) have a diagnosis of DSM-IV-TR 2 BPSD or LAMS subthreshold BP-NOS, as previous defined; (3) have a full-scale IQ >70; (4) be able to, along with at least one parent, complete all assessments; (5) be able to swallow multiple capsules or their powdered contents (training in swallowing was offered); (6) appear able to tolerate being off psychotropic medication(s) for a minimum of 11 weeks (3-week washout + 8-week trial); and (7) be off psychotropic medication(s) for at least 3 weeks prior to starting treatment. Exclusion criteria were as follows: (1) major medical disorders (e.g., diabetes, epilepsy, other metabolic disorders); (2) current psychotropic medication within 3 weeks prior to beginning study treatment; (3) inability to communicate in English; (4) lack of access via phone contact; (5) intellectual disability or autism; (6) psychotic symptoms; (7) active suicidal concern (i.e., the child might endorse passive suicidal ideation, such as “The world would be a better place without me” or “I wish I were dead” but may not have serious active suicidal ideation, e.g., “I want to die,” a plan for suicide, or an attempt in the past month).
Participants were allowed to continue any psychosocial interventions that were ongoing at the time of study enrollment and were asked not to make treatment changes until study completion. They were not allowed to receive psychotropic intervention during the washout period (other than the medication from which they were still weaning). Three (3) participants (30%) were taking psychotropic medications at the time of enrollment and completed the minimum 3-week washout period of these medications. Of these participants, number 6 was taking 0.5 mg clonazepam and 100 mg carbamazepine, number 7 was taking 15 mg aripiprazole and 300 mg oxcarbazepine, and number 10 was taking 1200 mg lithium carbonate and 25 mg dexmethylphenidate hydrochloride extended release. A fourth participant, number 4, had been taking 0.625 mL risperidone and 0.625 mL fluoxetine but tapered off prior to enrollment in anticipation of study participation (Table 1). All participants were receiving psychologic services throughout the study, though 1 participant, number 6, switched providers at the beginning of study participation and did not begin working with his new provider until the end of the study. Participant number 10 continued taking omega-3 fatty acids, and participant number 7 took omega-3 fatty acids plus melatonin throughout the study. These were allowed, but participants were asked not to make changes to these supplements from the time they were enrolled in the study until completion. Participant number 10 also began taking dexmethylphenidate, 10 mg, between study visits 5 and 6 and continued through the remainder of the study because of inattention and impulsivity that was impairing his school functioning (Table 1). This addition of a low level of dexmethylphenidate (10 mg per day compared to the 25 mg per day he took prior to beginning this trial) was well tolerated without any reported side-effects or worsening of mood symptoms.
BP-NOS, Bipolar Disorder-Not Otherwise Specified; ADHD, Attention Deficit Hyperactivity Disorder; ODD, Oppositional Defiant Disorder; subBP-NOS, subthreshold Bipolar Disorder-Not Otherwise Specified; MDD, Major Depressive Disorder; SAD, Separation Anxiety Disorder; SpPh, Specific Phobia; SocPh, Social Phobia; GAD, Generalized Anxiety Disorder; CD, Conduct Disorder; BP-I, Bipolar I Disorder; OCD, Obsessive Compulsive Disorder; DO, Dropped Out; n-3, Omega-3 Fatty Acids.
Participants were between the ages of 6 and 12 at study entry (mean [M]=8.9, standard deviation [SD]=2.02). Nine (9) children were white/non-Hispanic (90%) and 1 was white/Hispanic (10%). A majority (60%) were male. Participants' IQ, assessed by the two-subscale estimation from the Wechsler Abbreviated Scales of Intelligence (WASI), 25 ranged from 86 to 117 (M=98.7, SD=9.53). Family income of the sample ranged from $20,000 to over $100,000. Diagnoses included BP-I (10%), BP-NOS (30%), and subthreshold BP-NOS (60%). Of the 6 participants diagnosed with subthreshold BP-NOS, 2 met DSM-IV 2 diagnostic criteria for major depressive disorder (20%) and 1 met diagnostic criteria for dysthymic disorder (10%). All participants had one or more comorbid behavior disorders (9 had ADHD, 5 had oppositional defiant disorder, and 4 had conduct disorder), and 6 (60%) were diagnosed with one or more comorbid anxiety disorders (4 had a specific phobia, 1 had social phobia, 2 had separation anxiety disorder, 2 had generalized anxiety disorder, and 1 had obsessive-compulsive disorder). One (1) participant met diagnostic criteria for enuresis.
Procedures
Participants were recruited first using letters and flyers sent to a previously developed referral network, which included local psychiatrists, psychologists, pediatricians, family physicians, school psychologists, and other mental health professionals. Recruitment flyers were also distributed to families who potentially fit study criteria; these families were located from the LAMS (R01 MH073801) study, for which OSU is a data collection site. Third, one of the co-principal investigators (co-PIs) maintains a lengthy list of families who initiate contact for clinical services and agree to be called if future studies become available; these families were contacted regarding the current investigation. Lastly, an announcement was posted regarding study information on the Child and Adolescent Bipolar Foundation (CABF) website (
Upon being contacted by the parent/caregiver, prescreening interviews were conducted by phone to determine potential study eligibility/interest. If this prescreening interview indicated possible interest in and eligibility to participate in the study, the child and parent(s)/caregiver(s) were invited to the screening appointment, at which time informed assent, parental permission, and consent were obtained and the screening assessment was completed. Parents of children not eligible for study participation were offered referral information to seek other mental health services as appropriate.
Each enrolled parent–child pair completed seven assessments over 8 weeks. Children unable to swallow pills proceeded with a pill-swallowing protocol. 26 Three (3) of the 11 children who attended the screen visit had difficulty swallowing all capsules after completing the protocol and were given the option to mix the supplement into their food (participants number 2, 4, and 8). Although the manufacturer of EMP+ markets a flavored powder version of the active supplement, there is no powder placebo available. Therefore, to be able to determine the feasibility of consuming this supplement for a future placebo-controlled trial, participants were not given an option other than consuming the capsules that were distributed despite the less-than-optimal taste of the capsule powder. While using the flavored powder would likely have been helpful in this trial, it would not have been possible to use in a future placebo-controlled trial.
Medical and psychologic diagnostic and treatment history was gathered at the screen visit in addition to a cognitive and psychologic screen using the WASI 25 and Children's Interview for Psychiatric Syndromes–Child and Parent Forms (ChIPS/P-ChIPS), 27,28 respectively, to determine an estimate of cognitive functioning and DSM-IV 2 diagnoses. Mood symptoms and vital signs were collected at each visit. All vital signs were within normal limits. Blood draws and dietary monitoring were completed at visits 2 and 7 using Food Frequency Questionnaires (FFQ) and a 24-hour dietary recall interview (24hr). FFQs were completed by parents to determine dietary intake on an average week. The 24hr was completed with the child and parent to determine everything the participant ate the day prior to each blood draw. There were no significant differences in dietary intake on FFQ or 24hr pre- to postsupplementation. Brief physical examinations were also conducted at the first and final visits to monitor physical health.
The supplement was started after visit 2. All participants were given EMP+ and remained on supplementation for an average of 46.4 days (SD=23.29, median=55). Participants took the daily dosage of EMP+ recommended by the manufacturer and were advised to always take the capsules with food to reduce the likelihood of gastrointestinal upset. They began by taking 1 capsule 3 times a day for 2 days and increased up to 4 capsules 3 times a day (the target dose). Participants returned to the clinic for re-evaluation after an average of 9.8 days. If side-effects were minimal to nonexistent and more treatment response was desired, their dosage was increased to 5 capsules 3 times per day. If desirable treatment response was reached as determined by consensus between parent and interviewer, the dose was not increased. Dosage could be reduced at any time (or titration slowed) by phone for side-effects. Participant adherence was checked by standard capsule counts of returned unused dosage forms.
A clinical child psychology doctoral student supervised by a clinical child psychologist conducted all assessments. To maintain reliability, interviews were videotaped throughout the 8-week trial and 10% were randomly selected for independent raters to view and score symptoms after the open trial was complete. Intraclass correlations were calculated using ratings on each question in the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present Episode-Depression Rating Scale (KDRS) and Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present Episode-Mania Rating Scale (KMRS) that correspond to DSM-IV-TR 2 criteria for depression and mania. This included 12 depression items from the KDRS and 13 mania items from the KMRS. Study reliability for KDRS and KMRS ratings was 0.799 (p<0.001).
Measures
WASI 25 is a brief standardized intelligence test that provides estimates of verbal and nonverbal cognitive ability. The WASI was administered at baseline to determine an estimate of cognitive ability.
ChIPS/P-ChIPS 27,28 are structured psychiatric interviews designed to assess psychopathology according to DSM-IV 2 criteria in clinical and epidemiological research with children and adolescents ages 6–18 years using a “yes/no” question format. 29 –33 The ChIPS and P-ChIPS were administered at baseline to document the lifetime and current presence/absence of psychiatric symptoms and syndromes.
Depressive symptom severity was assessed using the KDRS. The KDRS is a 12-item semistructured interview with depression symptoms rated on a 6-point scale from none to severe. The KDRS was administered at each assessment.
KMRS 34 contains 21 items that assess the severity of manic symptoms in children and adolescents. The KMRS was administered at each assessment.
Data analysis
Study feasibility
Length of the sample recruitment period was used to determine recruitment feasibility. Treatment adherence was calculated by dividing the number of missed doses by the total number of doses since the last visit, subtracting this number from 1, and then multiplying by 100 to create an adherence percentage.
Trends in treatment response
KDRS and KMRS scores were graphed over time to inspect the time course of effect for intent-to-treat and study-completer analyses. Intent-to-treat analyses were completed for all participants, with the last observation carried forward for study dropouts. Two (2) one-tailed, nonparametric Fisher's randomization tests were completed to further examine trends in treatment response for depression and mania scores pre- and postsupplementation (visit 2 and visit 7) in the complete sample and then again in the 7 study completers.
Results
Study feasibility
Sample recruitment was hypothesized to be completed in 5 months. This estimate was based on recruitment rates for other research studies of youth with mood disorders in the Ohio State University Childhood Mood Disorder Research Lab. Institutional Review Board (IRB) approval was delayed such that summer recruitment did not occur, which anecdotally appeared to affect time to recruit, as numerous families who inquired about the study were willing for their child to taper off current medications during the summer months, but not during the school year and thus, they decided not to enroll in the study. Recruitment was actually completed in 6.5 months, being further delayed during the holiday season.
Seven (7) participants (70%) completed the entire open-label trial; 3 (30%) dropped out prior to completion. The 3 dropouts were the same 3 participants who had difficulty swallowing capsules (participants number 2, 4, and 8); although they completed swallowing training, they subsequently tried mixing the supplement contents with food. Participant number 4 refused to take the supplement and dropped out after visit 2. Participant number 2 was swallowing capsules well until her mother went out of town for a week, during which time she did not take the supplement. Upon her mother's return, the participant reported difficulty swallowing the capsules and dropped out following visit 3. Participant number 8 mixed his supplement in food until after visit 6, at which point he began taking an antidepressant and dropped out of the study (Table 1). Average adherence for the entire sample was 91.2% (SD=22.1%). Of those who completed the study, average adherence was 96.7% (SD=5.1%). See Table 2 for each participant's medication adherence across study visits.
Ss, subjects; M, mean; SD, standard deviation.
No participants experienced moderate or severe side-effects. Not including the 2 participants who dropped out of the study prior to reaching a full dose, 4 children took 12 capsules a day and 4 took the maximum 15 capsules a day. Four (4) participants reported mild nausea; 1 of them reported vomiting once, when taking the supplement without food. One (1) child reported mild difficulty falling asleep at one visit. Another child reported taking naps during the day and mild difficulty falling asleep twice. This child also reported slight increased appetite at one visit. A third child reported mild difficulty falling asleep and waking in the morning at one visit, but his mother believed this was due to the switch to Daylight Savings Time. One (1) child with no history of enuresis wet the bed 1 night during study participation, but her mother was confident this was unrelated to supplementation.
Trends in Treatment Response
Intent-to-treat analyses were completed, with the last observation carried forward for study dropouts, and outcome means were graphed over time to inspect the time course of effect for both the intent-to-treat sample and study completers (Figs. 1 and 2). It was hypothesized that depression (KDRS) and mania (KMRS) scores would decrease over time from pre to postsupplementation (visit 2 to visit 7). Results of intent-to-treat one-tailed, nonparametric Fisher randomization tests including all study participants showed a decreasing trend in depression scores approaching significance and a statistically significant decreasing trend in mania scores over the course of treatment (KDRS, p<0.06; KMRS, p<0.01). Based on intent-to-treat analyses, study participants experienced an average 37% decrease in depression scores and 45% decrease in mania scores from the start of EMP+ supplementation through the end of the study. Two (2) one-tailed nonparametric Fisher randomization tests were completed to examine trends in KDRS and KMRS scores over the course of treatment for study completers. Results showed a significant decreasing trend in depression (71%) and mania (58%) (KDRS, p<0.05; KMRS, p<0.05). As an exploratory analysis, the scores of the KDRS and KMRS were added to make a total mood score. Total mood score means are graphed across visits in Figure 3 as a global measure of outcome. Two, one-tailed, nonparametric Fisher randomization tests were completed to examine trends in total mood scores over the course of treatment for all participants and for study completers. The pre–post global improvement was 42% for the intent-to-treat sample (p<0.05) and 62% for study completers (p=0.01), showing a significant decreasing trend in total mood score.
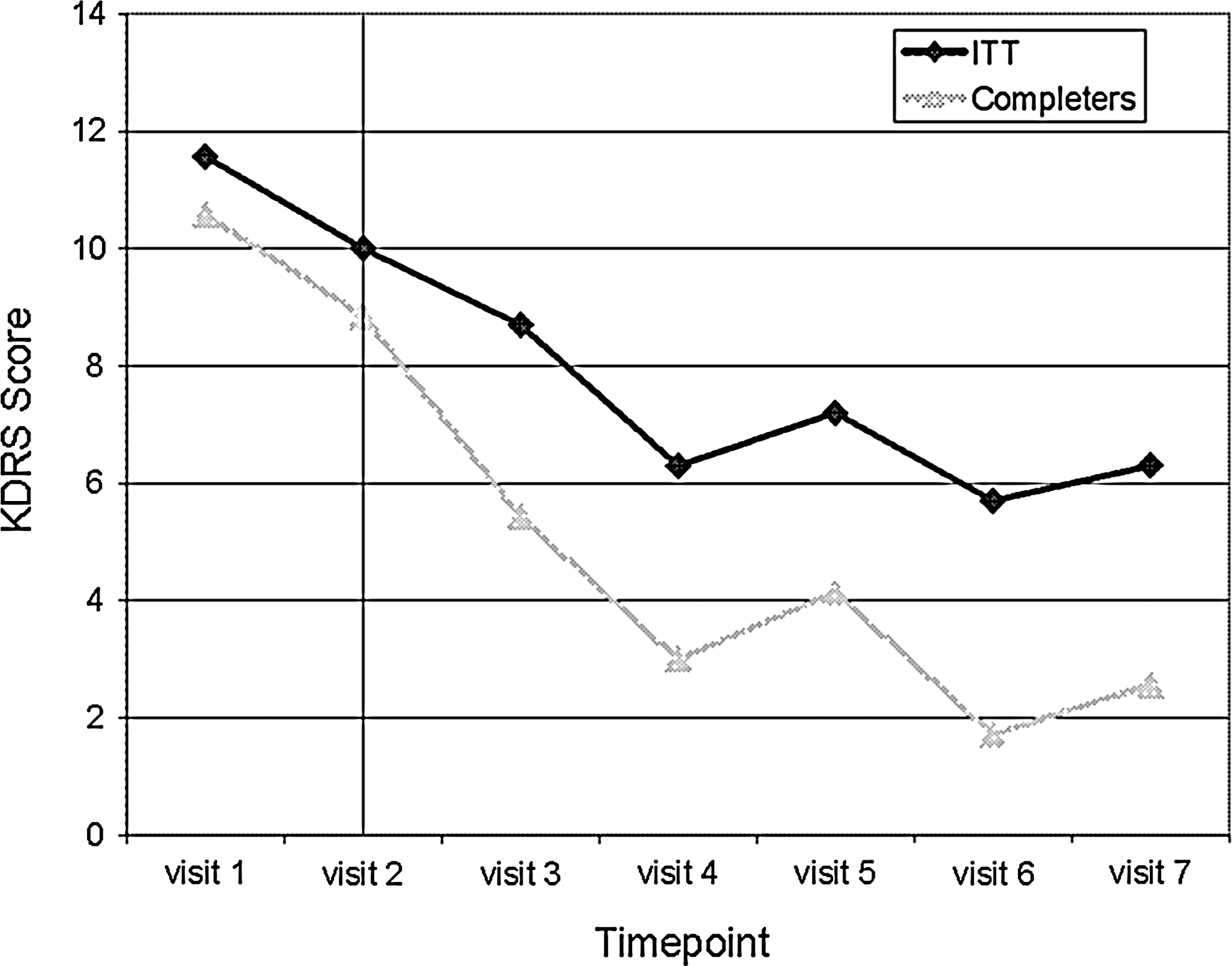
Mean depression ratings (KDRS) for all participants over time (Intent-to-Treat: ITT) and study completers. KDRS, Depression section of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present Episode-Depression Rating Scale.
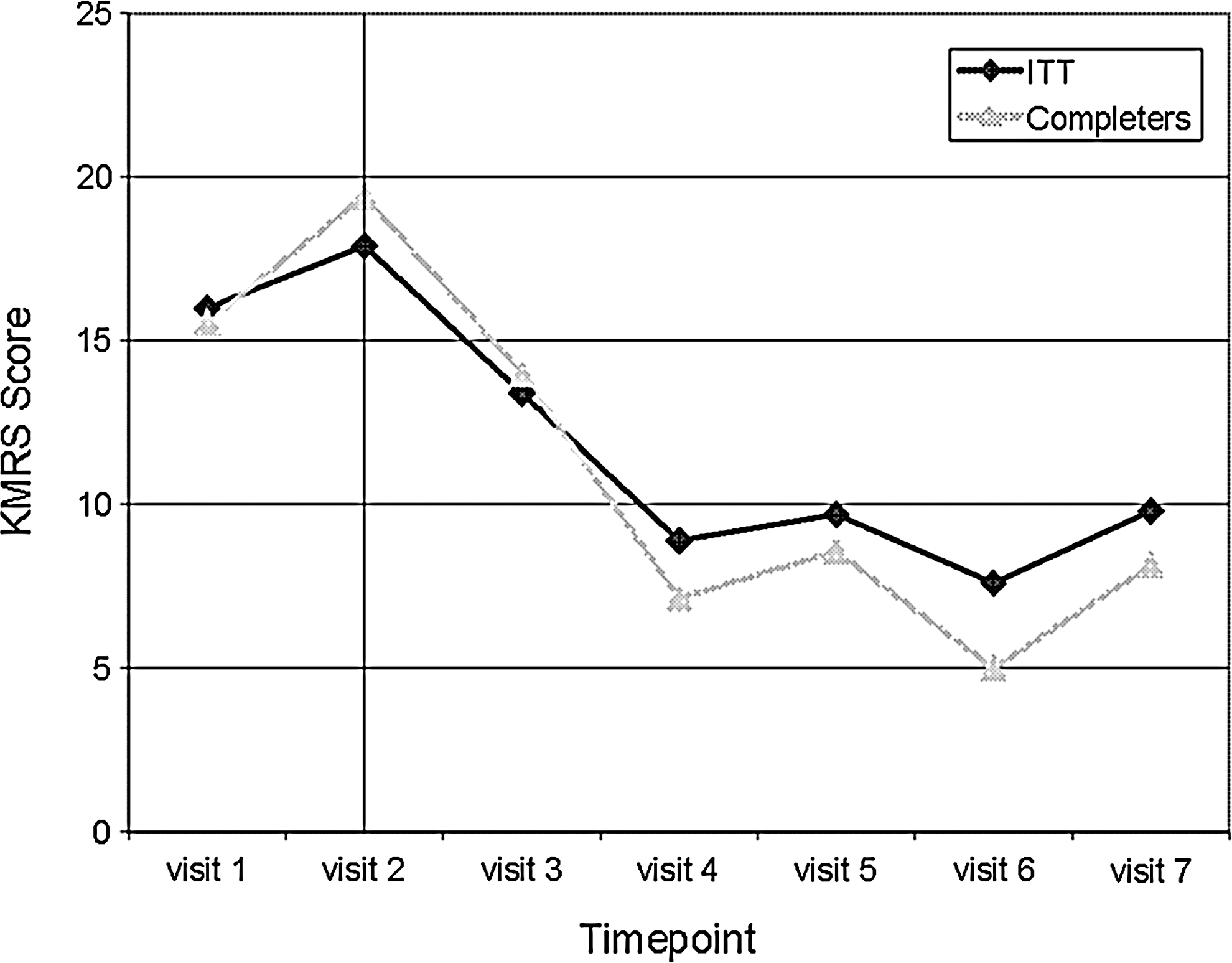
Mean mania ratings (KMRS) for all participants over time (Intent-to-Treat: ITT) and study completers. KMRS, Mania section of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present Episode-Depression Rating Scale.
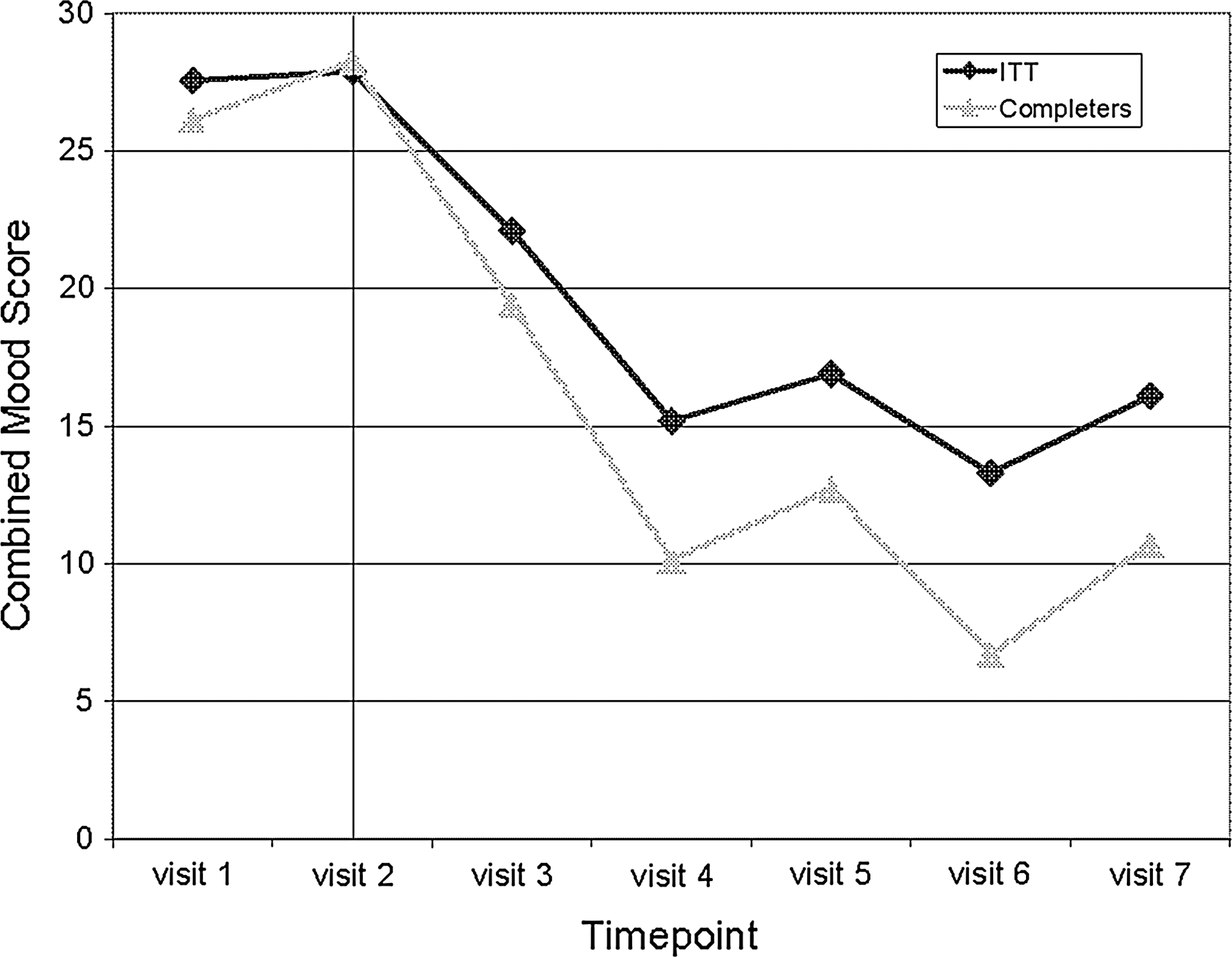
Mean combined mood ratings (KDRS + KMRS) for all participants over time (Intent-to-Treat: ITT) and study completers. KDRS, Depression section of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present Episode-Depression Rating Scale; KMRS, Mania section of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present Episode-Depression Rating Scale.
Discussion
Innovative treatments are sorely needed to treat the distressing symptoms associated with childhood BPSD. Unfortunately, clinical treatment trials in youth are sparse, and psychotropic medications found efficacious are often associated with adverse side-effects. 6,7 Research on nutritional supplements as treatment for childhood BPSD show potential benefit without these adverse side-effects. 15 –18,20,24 This open pilot study examined a micronutrient with intriguing preliminary data suggestive of mood regulatory properties.
Feasibility of sample recruitment and retention
Study recruitment took 1.5 months longer than hypothesized, given an IRB-related delay in starting the study that prevented recruitment during the summer. Multiple parents who inquired about the study were unwilling to have their child forego stimulant medications during the school year to complete the study. Notably, 1 study participant began a concomitant stimulant between study visits 5 and 6. He had a robust treatment response with no adverse events following this addition. Anecdotal poststudy reports indicated ongoing stabilization of ADHD and mood symptoms. Consideration of allowing stimulants as concomitant medications during a subsequent trial would be useful.
Supplement adherence
Three (3) participants dropped out of the study prior to completion due to adherence and tolerability issues. When these children attempted mixing supplement powder from the EMP+ capsules with food instead of swallowing the capsule whole, they continued to have palatability issues due to the taste of the powder. (Of note, the commercially available product has flavored powder; to maintain dosage rigor in this study, families were advised to open the capsules and ingest the powder within, which was not flavored.) This 30% dropout is not far from the average 20%–25% dropout rate noted previously for youth in psychotropic treatment studies of mood disorders. 9,10 Of the 7 participants who completed the study, all maintained high adherence rates. These results suggest that children who have difficulty swallowing EMP+ after completing the swallowing protocol are likely not good candidates for a study of EMP+, although they might find the flavored powder palatable enough for clinical treatment. Future studies should either require that children be able to swallow the capsules (for which placebo is available) or be offered the flavored powder supplement, for which a placebo is not currently available.
Trends in treatment response
Exploratory analyses of mood symptoms throughout this pilot trial suggest decreases in depression and mania symptoms over the course of EMP+ supplementation. Results must be interpreted with caution for several reasons. First, while this trial was similar in length to many mood disorders medication treatment trials, there are difficulties inherent in studying mood symptoms over a relatively short time period due to their natural waxing and waning. Second, this was an open-label study, so history, regression to the mean, and possible placebo effects could not be controlled. In fact, a recent review article on randomized placebo-controlled trials for acute bipolar mania in adults showed that although participants responded better to psychotropic interventions compared to placebo, there were also many placebo responders. 35 Placebo response ranges were reported from 18.7% to 33.6% in studies of haloperidol, olanzapine, quetiapine, risperidone, aripiprazole, lithium, valproate semisodium, and carbamazepine. 35 However, the magnitude of the decrease in depression and mania scores in this trial (37% and 45%, respectively) surpasses that reported for placebo and suggests that future randomized placebo-controlled trials are warranted.
Conclusions
In addition to concerns about the open-label study design and relatively short length of the trial, this study employed a small sample size (N=10), further limiting the types of analyses and interpretation of data in this study. While this study provided helpful information on feasibility of recruitment, medication adherence, and an exploratory look at effect on mood symptoms, larger, placebo-controlled clinical trials are needed. There are numerous unanswered questions regarding treatment response, optimal dosing, mechanisms of action, and long-term effects of the nutrient doses found in EMP+. This study lays the groundwork for better-controlled micronutrient treatment studies for childhood BPSD and suggests that further, more scientifically rigorous study is warranted.
Footnotes
Acknowledgments
This study was funded by a grant from the Psychiatric Research Foundation, a local private foundation. EMP+ capsules were donated by the manufacturer, Truehope Nutritional Support, Ltd. No financial contributions were made by the manufacturer.
Disclosure Statement
Dr. Arnold receives consulting and speaking honoraria and research funding from numerous drug companies, but none from Truehope, which sells EMP+. Dr. Arnold has had research funding from Autism Speaks, Curemark, NIMH, Neuropharm, Novartis, Noven, Shire, Sigma Tau, and Targacept; has consulted for Abbott, Biomarin, Neuropharm, Novartis, Noven, Organon, Shire, and Sigma Tau; and is/was on speaker's bureau for McNeil, Novartis, and Shire. Dr. Fristad receives royalties from APPI, Guilford Press, and CFPSI. Ms. Frazier has no conflict of interest or financial ties to disclose.