
Abstract
Background:
Diminished taste acuity (hypogeusia) has been linked to zinc deficiency in humans and animals. This phenomenon has been exploited in the Zinc Taste Test (ZTT), a taste acuity test commonly employed by Australian naturopaths. However, its validity has not yet been firmly established.
Methods:
A systematic search of several key databases was conducted. Only studies in which there were full reports of clinical trials comparing the ZTT to at least one other zinc test within the same sample population were included.
Results:
Three (3) studies matched the criteria for inclusion. Study I compared the ZTT with sweat zinc in patients with food intolerance, reporting moderate correlation. Study II recruited pregnant women using the ZTT and serum zinc to assess zinc status, with above 70% congruence between the two tests at the start of the trial and 100% congruence at the end. Study III also recruited pregnant women at three stages during gestation, assessing ZTT and leukocyte zinc initially, later adding dietary zinc intake and at delivery cord blood zinc. No significant correlation was found between the results of these different methods; however, statistically significant differences in the ZTT responders (tasters and nontasters) were found for pregnancy outcomes.
Discussion:
The methodology of the three studies is critically discussed. Although depletion of zinc leads to decreased taste acuity, it does not explain all cases of hypogeusia. Various other influences on taste perception are discussed in relation to the validity of the ZTT. Stringent exclusion criteria are therefore mandatory to increase specificity. Large variations from the original test design have been identified. The laboratory assays of zinc in these studies are also lacking sensitivity to accurately assess zinc status.
Conclusions:
To date, there are no tests that are both sensitive and specific that accurately assess marginal zinc status in humans. The ZTT, albeit widely used, does not fill this void, and further research is needed.
Introduction
Findings of a survey investigating the preferred zinc assessment methods of Australian naturopaths indicate that the dominant method used is a taste acuity test. 34 Several Australian companies produce and market a test solution based on a design proposed by Bryce-Smith in 1984, 35 commonly called “zinc taste test” (ZTT). Patients hold 5–10 mL of a 0.1% zinc sulphate septahydrate solution (ZnSO4×7H2O) in their mouth, swallow it, and then describe the taste after 10 seconds. Guidelines regarding the classification and interpretation of patients' responses mainly adhere to the Bryce-Smith scoring system (1–4), 36,37 where a score of 1 or 2 indicates zinc deficiency, necessitating supplementation.
The first published literature referring to the Bryce-Smith ZTT was a letter in The Lancet in 1984 35 in which the authors describe a case of anorexia nervosa in a 13-year-old girl tentatively diagnosed with zinc deficiency on the basis of her inability to taste the zinc sulphate solution, in contrast to other people. The girl's recovery from anorexia was attributed to subsequent zinc supplementation and “confirmed” by changes in her response to the test solution. Shortly after, Bryce-Smith and Simpson published another letter in The Lancet 37 detailing a series of ad hoc trials of the ZTT in patients suffering from a range of depressive disorders. The researchers found that individuals unable to taste the solution invariably experienced some symptomatic improvement following zinc supplementation. As a result of these informal and to-date unpublished trials, the ZTT design, its methodology, and the scoring system for interpreting subjects' responses were formalized. 36,37
To date, there are only three published studies utilizing the Bryce-Smith ZTT. 38 –40 Three (3) other trials 41,42 have been conducted but not reported in the scientific literature in their entirety. A small study comparing ZTT responses between patients with acquired immune deficiency syndrome and controls has only been reported in the form of a poster abstract. 42 The other two trials of the ZTT, conducted in women with postnatal depression, are referred to in a letter to the editor in the British Journal of Psychiatry in 1990. 41
While the underlying evidence supporting zinc's role in taste perception is extensive, 1 –4,15,16,43 –51 an accurate clinical measure of taste acuity that reliably reflects zinc status has not yet been identified. 30,52 In particular, chemical gustometry techniques have been criticized as being nonquantitative and subject to confounding variables such as nutritional habits, preferences, 53 satiety, and food residues. 54 Electrogustometry as an alternative means of determining detection thresholds has gained considerable recent support with some, 53,55 but not all, 56 researchers and specialist clinicians.
Methods
Search strategy
A systematic search of MEDLINE®, EMBASE, Allied and Complementary Medicine (AMED) and the Web of Knowledge was conducted using the terms
Study selection
Studies were only included if they were full reports of a clinical trial comparing the results of the ZTT with at least one other measure of zinc status within the same sample population.
Data extraction and synthesis
Key data extracted included characteristics of the study population, exclusion criteria, sample size, other method(s) of zinc assessment studied, methodology of ZTT, deficiency criteria for the ZTT, intervention, and other outcomes measured. Due to heterogeneity of the trials' study designs, ZTT methodology and statistical analyses comparing results is difficult; however, the details and results of each study are reported here as a summary of the evidence to date.
Results
The current review identified three studies comparing zinc assessment using the ZTT and at least one other measure of zinc status. The earliest study performed in 1990 compared the results of the ZTT with sweat mineral analysis. 38 Two (2) studies were conducted in pregnant women in 1993 by different researchers, the first of which used serum zinc concentrations for comparison 39 while the latter included three different comparative measures: leukocyte zinc concentrations, dietary intake, and cord blood zinc content. 40
Outline of Study Designs and Results
The study design used by Eaton et al. 38 (Fig. 1) involved food intolerance patients of mixed gender and ages self-administering the ZTT nightly for 1 month. Within the same period, a sweat mineral analysis was performed once on these subjects (T1). Zinc deficiency, as determined by the ZTT, was defined as any score <4 and the reference range for sweat zinc concentration was 410–980 μg/dL for women, 360–680 μg/dL for men, and 500–920 μg/dL for children aged 2–15 years.
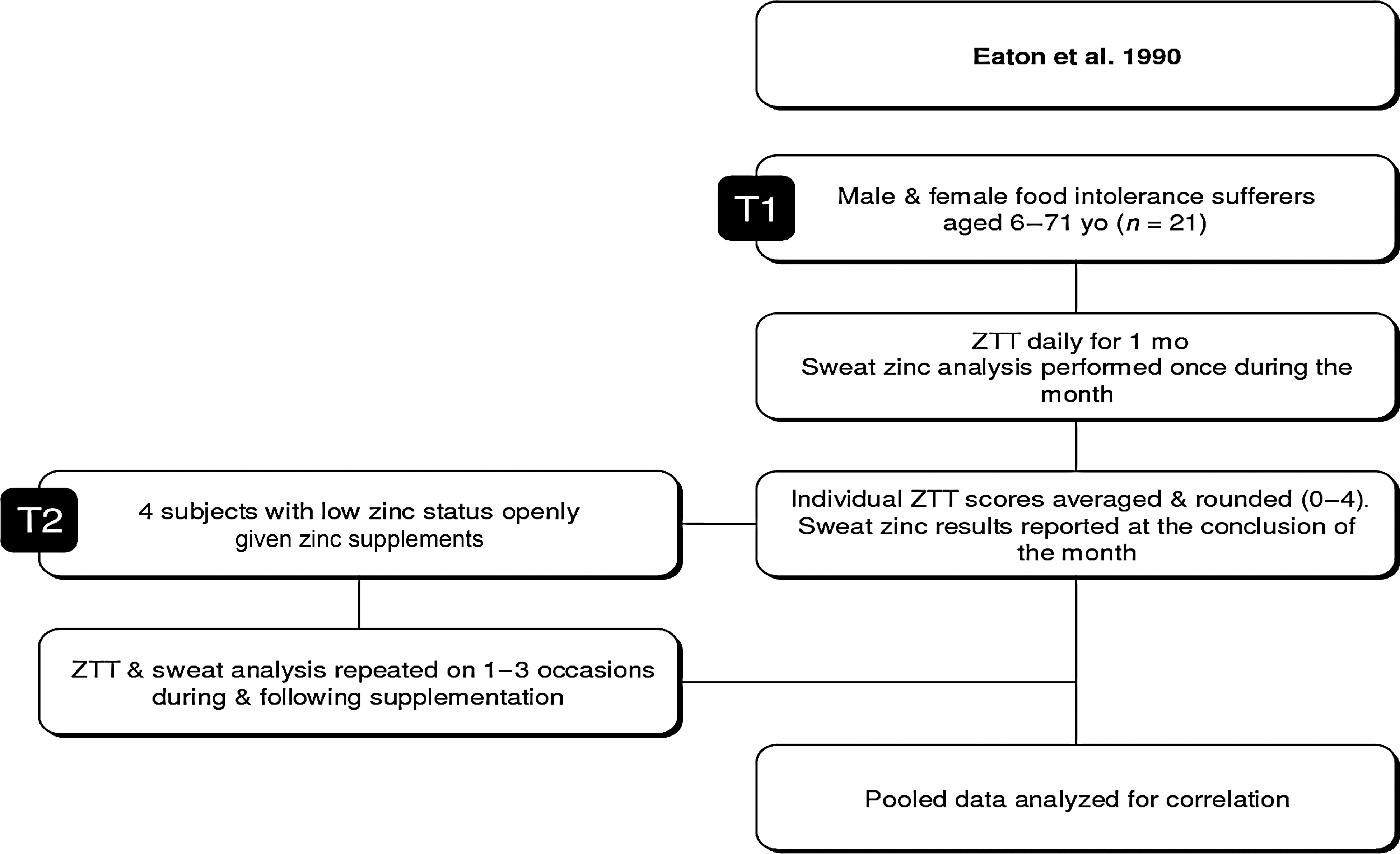
Eaton et al. 38 study design. ZTT, zinc taste test; yo, years old; mo, months.
The authors recorded the changes in sweat minerals and taste test as a result of zinc supplementation in subjects with low status. 38 The doses administered were not mentioned. This small subgroup comprised 4 subjects whose ZTT score average was between 0 and 3, and sweat zinc values ranged from 193 to 416 μg/dL. All subsequent ZTT and sweat zinc results for these individuals were pooled with the rest of the data (T2), which were then analyzed for correlation between T1 and T2.
ZTT results and sweat zinc concentrations for the pooled data were reported to exhibit a significant moderate correlation (p<0.01) using analysis of variance. Postintervention results for the four supplemented patients were not subject to independent correlation testing, and therefore the ZTT sensitivity to altered zinc status cannot be commented on from this study.
Garg et al. 39 (Fig. 2) tested pregnant women. They report using exclusion criteria for sample selection that included cardiac, renal, or hepatic disease and habitual tobacco or betel nut chewing. Recruited subjects were assessed using the ZTT and serum zinc upon entry into the trial (T1), and again at term, following randomization into treatment (45 mg elemental zinc per day) and placebo (B complex tablets) (T2). It remains unclear whether both deficient and replete subjects were randomized into control and treatment groups or only those deemed deficient at baseline. Also, it is unknown whether the administration of the intervention was single- or double-blinded. The three subgroups (I, II, and III) reflect both the subjects' pregnancy trimester at the time of recruitment and the subsequent duration of treatment with either zinc or placebo. Zinc deficiency was defined as a score of 1 or 2 for the ZTT and<90 μg/dL serum zinc (T1). In 70.0%–100.0% of subjects, the two values concurred (Table 1).
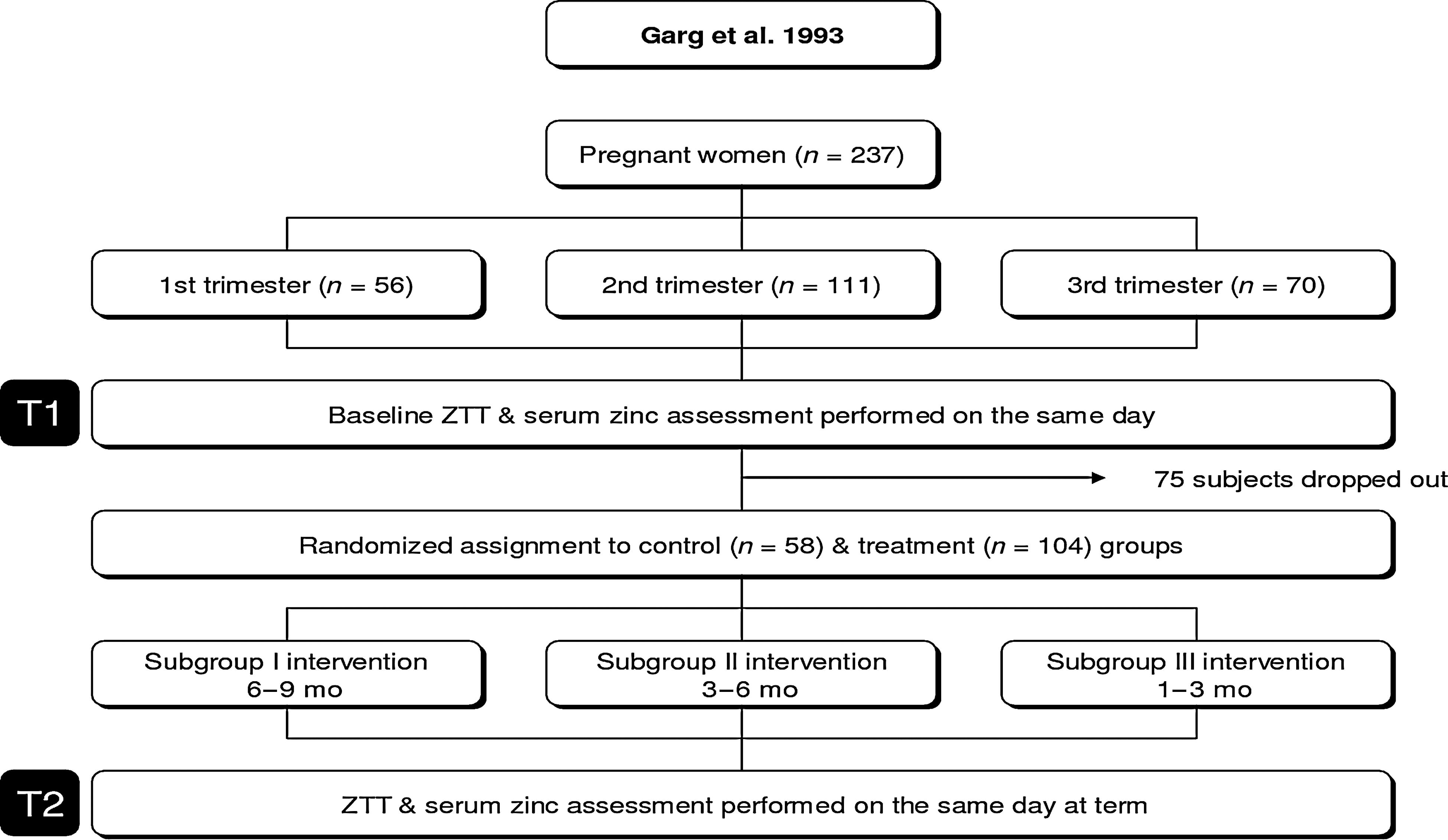
Garg et al. 39 study design. ZTT, zinc taste test; mo, months.
All subjects in the treatment group recorded a ZTT score of either 3 or 4 at the end of the trial (T2). Individual serum zinc results for this period were not reported; however, the authors state that the two measures demonstrated 100% agreement.
Mahomed et al. 40 (Fig. 3) assessed the zinc status of a sample of pregnant women three times: at enrollment <20 weeks (T1), at 28–32 weeks (T2), and again at delivery (T3), the latter two occurring subsequent to randomization into double-blinded control (unknown placebo) and treatment groups (20 mg/day elemental zinc). The T1 assessment phase comprised ZTT and leukocyte zinc. The T2 assessment repeated both ZTT and leukocyte zinc in addition to dietary intake analysis for zinc. T3 assessment involved the ZTT and measurement of zinc content of cord blood.
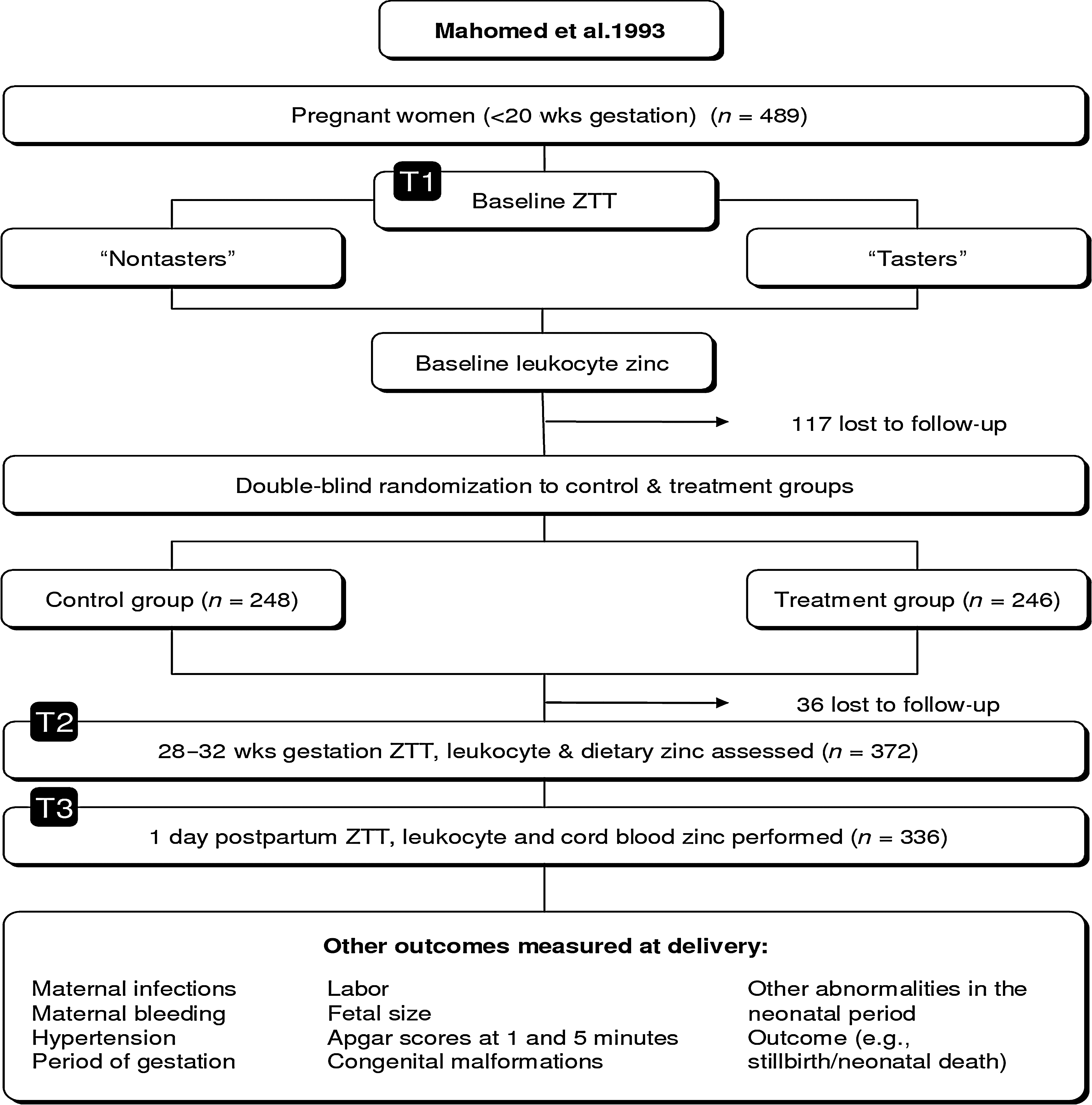
Mahomed et al. 40 study design. ZTT, zinc taste test; mo, months; wks, weeks.
Based on the authors' previous experience with the ZTT, 41 the original Bryce-Smith scoring system was replaced by the following categories: no taste; mild/moderate; and strong. ZTT responses were then further simplified into two groups: “nontasters” (no taste) and “tasters” (mild-strong taste). Nontasters were interpreted as being zinc deficient and tasters zinc replete. The reference ranges for leukocyte and cord blood zinc values were not given.
Statistical comparisons between different zinc assessment methods at all three assessment periods were made using Mann–Whitney tests (comparison of ranked means). At T1 there was a nonsignificant trend of higher leukocyte zinc in nontasters than tasters (p=0.16). At T2 there were no significant differences in leukocyte zinc or the dietary intake of zinc between tasters and nontasters. At term, leukocyte zinc again failed to demonstrate a statistically significant relationship with subjects' ability to taste the ZTT; however, median cord blood zinc concentration showed a nonsignificant trend of being slightly higher in infants of nontasting mothers than tasting mothers.
The only statistically significant relationships reported for ZTT scores by Mahomed et al. 40 were with a variety of pregnancy outcomes. Nontasters reportedly exhibited less maternal weight gain (p<0.05), higher incidence of diastolic hypertension (p<0.01), and increased rates of fetal retardation from previous pregnancies (p<0.05). The authors also report a nonsignificant trend of higher rates of proteinuric hypertension (7.1% of nontasters versus 2.1% of tasters); however, they subsequently dismiss this as being likely due to chance as there was no significant relationship between ZTT responses and infant size.
Discussion
Overall, high-quality evidence comparing the ZTT and other measures of zinc status is currently lacking. The large methodological variability of the three trials presented here hinders direct comparison of results and also heralds a number of methodological issues.
Interindividual variability in taste acuity independent of zinc
There are many influences upon taste acuity that appear to be independent of zinc status. These include both age 21,53,57 –63 and gender 54,64 –67 ; therefore, samples that comprise both males and females across a wide age distribution, while using one generic scoring system such as in the study by Eaton et al., 38 warrant further review.
Two (2) of the clinical trials included in this review used pregnant women as their study population. Zinc status is of particular interest in light of research indicating a critical role for zinc in both maternal and fetal health, 28,68 –70 in addition to epidemiological evidence that suggests suboptimal intake of zinc may be widespread in this group. 71 The majority of pregnant women, however, demonstrate some degree of altered taste perception from the first trimester onwards, 64,72 –75 which may be independent of zinc nutriture. 74
Individual responses to taste acuity testing have also been shown to vary in relation to recency of food consumption. 54,76 Results of a study performed in healthy young males suggest higher recognition thresholds for sweet and salty substances during satiety in comparison to fasting (14–16 hours) periods. 54 Sensitivity to bitter flavors appeared unchanged, and sour taste was not included in the investigation. Information pertaining to effects on the perception of a metallic taste is currently not available.
Of the studies reviewed here, only Eaton et al. 38 provided details about the timing of the ZTT, with subjects advised to administer the test “late at night, well after the last meal.” The potential variations in time of administration of the ZTT may introduce a confounding influence upon ZTT scores as a result of difference in satiety state between individuals within the one study and between different studies.
Additionally, taste recognition thresholds can be lowered with repetitive exposure to a given taste acuity test. 18 In the studies performed by Garg et al. 39 and Mahomed et al., 40 minimal testing over extended periods (e.g., two to three tests conducted over 12–40 weeks) minimizes the effect of this confounding influence.
The improvements noted by Eaton et al., 38 however, with nightly tests for 1 month, could mean that any improvements in ZTT responses, resulting in a higher average score, were an artifact created by “practice effect” rather than indicating improved zinc levels.
An additional issue for consideration is the influence of genetics. Recent research in psychophysics has revealed that an estimated 25% of the American population are “super-tasters” as a result of two dominant alleles on chromosome 5, producing higher taste bud density and significantly lower taste thresholds for a variety of flavors, while another 25%, the recessive homozygotes, suffer “taste-blindness.” 65,77 –79 It would be advantageous to identify and exclude individuals of both genotypes from subsequent taste acuity studies through validated testing techniques. 77
Additional causes of taste impairment
Research into the etiology of taste impairment has revealed a long list of possible causes and contributing factors that includes various pathologies and drugs. 53 –55,58,64,80,81 Henkin, a pioneer of research into zinc-related hypogeusia, concluded in 1976 that zinc could not explain all cases of taste impairment, 82 with a subsequent review concurring that it was likely that “depletion of zinc can lead to decreased taste acuity but decreased taste acuity is not necessarily associated with depletion of zinc.” 1 More recent research supports this, implicating zinc deficiency in only 10% of Japanese patients 55 and approximately 33% of American patients presenting with taste disorders. 80
Consequently, it seems imperative that all clinical trials utilizing the ZTT as a measure of zinc status develop and implement stringent exclusion criteria to rule out extraneous causes of hypogeusia/ageusia. In doing so, subjects suffering from taste disorders unrelated to zinc status, and consequently false-positive test results, could be minimized. Of the three studies reviewed here, only Garg et al. 39 reported using any exclusion criteria; however, it does not appear to have been comprehensive/complete nor prospective, citing only that “in the present study, all these factors, which could affect taste perception were ruled out” (p. 321).
The absence of exclusion criteria in the study by Mahomed et al. 40 is of particular concern, given the high proportion of heavy smokers (20+/d) in the nontasters' subsample compared to the tasters (14% versus 3%, p=0.001). Research suggests that smokers exhibit varying degrees of taste impairment not exclusively associated with zinc deficiency. 65,83 –86 This therefore prompts the question of whether the response of these smokers to the ZTT was an accurate reflection of their zinc status or of other smoking-induced gustatory pathology.
ZTT methodology
All three groups of researchers 38 –40 identify the ZTT method they used as being based on the original Bryce-Smith design 35 ; however, each exhibits elements of modification from this methodology (Table 2). 36,37 It becomes evident that there are significant differences in the execution of the ZTT in many areas, including the concentration and quantity of the test solution, scoring and interpretation of subjects' responses, and the timing of the test.
In chemical gustometry, the detection threshold is the lowest concentration at which a taste can be detected (e.g., subject recognizes that the solution is not water) while the recognition threshold is the lowest concentration at which a taste stimulus can be accurately identified. 87 Traditional chemical gustometry techniques have employed tastants in a variety of concentrations using an “up–down staircase technique,” 87 whereby subjects are administered increasing or decreasing concentrations to establish detection and recognition thresholds. 18,88 In contrast, the ZTT proposes to account for both thresholds given a fixed concentration, with subjects scoring more lowly if they can distinguish the zinc sulphate solution from water but cannot accurately identify the specific flavor than those who can do both. In light of this important difference between traditional chemical gustometry and the ZTT, it is imperative that the original test solution concentration (0.1%), as used by Bryce-Smith, 36,37 is always used if the original scoring and interpretation of subjects' responses are to remain meaningful.
However, because of the various starting concentrations and dilutions used by the different trials reviewed here, the final test solution concentrations were 0.01%, 38 1%, 39 and 0.1%. 40 The concentration cited by Garg et al. (1%) 39 begs the question of whether this has been incorrectly reported. Based on the earlier discussion, different test solution concentrations warrant different scoring systems for subjects' responses and yet Garg et al., 39 using a test solution 10 times stronger than that proposed by Bryce-Smith, have used the same scoring system. 37 The scoring system used by Eaton et al. 38 introduces one new response category but otherwise also correlates with the Bryce-Smith scores while using a solution 10 times weaker.
The quantities of the test solution used also varied between studies: 55 mL, 38 2 mL, 39 and 10 mL, 40 which creates another potential confounding variable, and with increasing concentration there is a corresponding increased risk of excess and toxicity.
The authors' interpretation of subjects' ZTT responses in relation to their zinc status were consistent for “no taste,” which was deemed by all authors to be indicative of zinc deficiency and “strong taste,” which was taken to indicate zinc repletion. 38 –40 Response categories between the two poles were interpreted differently by different authors. It is interesting to note the decision of Mahomed et al. 40 to simplify the ZTT response categories to “nontasters” and “tasters.” This decision appears in part to be the result of two earlier studies they conducted involving the ZTT. 41 The researchers commented that there was marked difficulty in differentiating between a “2” and “3” response as defined originally by Bryce-Smith. The inconsistent interpretation of these response categories by other researchers may act as confirmation of this.
Comparator zinc assessment methods
According to the scientific evidence, there is currently no means of assessing zinc status in humans, particularly with respect to the detection of marginal deficiency states, that has demonstrated absolute accuracy, and the identification of such a test has been flagged as an area requiring urgent research. 12,28,89,90 Consequently, in light of the knowledge that hypogeusia is a feature of early zinc deficiency, 10 –18,20 the choice of assessment method with which to compare the results of a ZTT is not straightforward.
Serum testing, as used by Garg et al., 39 although currently the first-line orthodox test for zinc status, has been principally validated as a tool to assess zinc adequacy of large populations 91,92 and lacks the sensitivity to accurately ascertain individual adequacy. Decreased serum values are reported to be reflective of end-stage depletion only. 15,28,43,46,48,91,93,94 Furthermore, serum zinc concentrations are influenced by multiple confounding variables. The most relevant to the study by Garg et al. 39 include diurnal variation and hemodilution of pregnancy. 28,52,69,95 Neither of these issues was addressed in their article; therefore, it must be assumed that they were not accounted for, potentially leading to incorrect interpretation of results.
The decision to use sweat mineral analysis in the Eaton et al. study 38 is also controversial, given the lack of ongoing validating research into this assessment method. Although some promising studies were reported between the 1960s and 1990s, 96 –98 sweat zinc analysis has been superseded by other more accurate methods (e.g., metallothionein monocyte mRNA). 93
The measurement of leukocyte zinc, as used by Mahomed et al., 40 still lacks adequate validation according to some researchers. 93 –99 While other studies have demonstrated a strong correlation between leukocyte zinc concentration and total body zinc 52,100 other research suggests that leukocyte zinc levels may be limited to the detection of severe rather than marginal deficiency states. 99,101 Importantly, due to an increased monocyte-to-polymorphonuclear-leukocyte ratio in pregnancy and the resultant “elevated” zinc content of mixed leukocytes, analysis of neutrophil zinc concentrations is a more accurate method in a pregnant population. 52 While this does not invalidate the use of leukocyte zinc, it necessitates the use of reference ranges tailored to each trimester of pregnancy, which does not appear to be the case in the study by Mahomed et al. 40
Conclusions
Scientific attempts to validate the ZTT as an accurate marker of zinc status through controlled comparisons with other zinc assessment methods is a difficult undertaking. The most significant obstacle is arguably the lack of sensitive and specific markers for the detection of marginal zinc deficiency in which taste impairment is an early feature. To address this, future attempts to investigate any correlation between ZTT scores and other zinc measures could be improved by comparing the ZTT results with a combination of cohesive zinc assessment methods (e.g., serum, metallothionein monocyte mRNA 89,93 and functional response to supplemental zinc). 28,102 However, careful interpretation would still be necessary to allow for the established and hypothesized limitations of each assessment tool.
Two (2) additional priorities have emerged as a result of this review: (1) the need for the development and consistent implementation of exclusion criteria in all future studies investigating the ZTT, such that individuals suffering from hypogeusia/ageusia independent of zinc status are excluded from the sample, thus reducing the potential for false-negative results; and (2) the establishment of a unanimous model for the execution of the ZTT, thereby permitting a more thorough comparison of the results of future studies.
Another area for follow-up research is a comparison between the ZTT and previously validated taste acuity testing methods used in marginally zinc-deficient populations. 11,14,16,18 –20,22 These tests, based on the large amount of research linking low zinc status to higher taste thresholds (especially in relation to salt detection) demonstrate the robustness of taste acuity assessment in general. 87 Such studies would clarify the relationship between subjects' taste thresholds for the four primary flavors (salt, sour, sweet, and bitter) and subjects' ability to detect the zinc sulphate solution, which falls outside of these, being of a metallic taste. 37,39 They would need to incorporate a biochemical index of zinc status in addition to these functional tests. 30 The results of this research alone may rule out the need for future studies of the ZTT and therefore should be flagged as a priority.
The three studies included in this review reveal the limited evidence currently available for the ZTT. Of these articles, one reported high rates of consensus between ZTT results and serum zinc 39 and one a moderate correlation between the ZTT and sweat zinc in a small group of subjects 38 ; however, neither study was of a particularly high quality and both possess methodological flaws that place some doubt on these findings. The largest study to date 40 failed to demonstrate a correlation between the ZTT and three different measures of zinc status performed during successive assessment periods in pregnant women and, although still exhibiting some methodological weaknesses, was the best of the three in terms of study design. It also reported some statistically significant relationships between individuals' ZTT scores and pregnancy outcomes that warrant further investigation. At present, there appears to be insufficient evidence to support the use of the ZTT as a means of assessing zinc status in individuals.
To accurately assess zinc status is difficult because this mineral is widely distributed within the body and plays a role in many enzymatic reactions. The research reviewed here shows insufficient power and accuracy to validate the ZTT as a marker for zinc deficiency, especially in its mild form. Stringent inclusion and exclusion criteria need to be established in order to increase sensitivity and particularly specificity of the ZTT.
To address these shortcomings, future studies should focus on comparisons of the ZTT, with currently employed methods as well as less utilized yet more cohesive assays, such as serum metallothionein monocyte mRNA and functional response to supplemental zinc.
Footnotes
Acknowledgments
This review was part of a large survey that received funding of AUS$1,000 from Health World Ltd. Australia.
Disclosure Statement
No competing financial interests exist for any of the authors.