
Abstract
Objectives:
Cocaine addiction continues to be a major public health problem in the United States. With no U.S. Food and Drug Administration–approved pharmaceutical therapy, treatment often relies on psychosocial interventions. This pilot therapy development study attempts to examine the feasibility and preliminary efficacy of adding breathing-based Integrative Meditation and Ear Acupressure (IMEA) to outpatient treatment of cocaine addiction.
Design:
Fifty-six (56) cocaine-dependent patients were recruited from an outpatient addiction treatment facility in Baltimore, MD and randomized into either an IMEA or a treatment as usual (TAU) group for the 12 weeks of study, with weekly meetings to monitor treatment outcomes and to facilitate meditative therapy.
Outcome measures:
The outcome measures consisted of treatment retention rates by week 8 and 12; abstinence rates measured by 6 continuous weeks of negative urinalysis for cocaine, and addiction-related symptoms such as anxiety, craving, depression, and withdrawal symptoms.
Results:
With the assistance of simplified breath training and a portable MP4 device, 80% of IMEA participants self-reported practicing breathing or meditation 5+ days a week with acceptable compliance and showed strong interest in meditative techniques. Compared to TAU, IMEA participants reported significantly higher treatment completion rates by week 8 (89% versus 63%) and week 12 (81% versus 58%), higher abstinence rates (66% versus 34%), and significantly greater reduction in craving, anxiety, and other addiction-related symptoms. Some participants continued meditation after study completion.
Conclusions:
It is feasible to add breathing-based IMEA to outpatient treatment of cocaine addiction. Although a number of limitations exist for this pilot study, further large-scale clinical trials and therapy-development studies of IMEA for addiction are warranted.
Introduction
IM, an adaptation of Chinese medical qigong practice, is a simplified form of mindfulness meditation. It involves adjusting the breath to near resonant frequency (RF, about six breaths per minute), shown to be a rapid way of improving the body's autonomic nervous system while lowering stress. 7,8 along with regulating the mind with inward attention, mindfulness, and guided imagery, and adjusting the body to experience relaxation, increased sensation, and a tranquil state. IM, relatively easy to learn and practice, helps to reduce the anxiety, depression, irritability, and difficulties with attention or concentration that are common in early addiction recovery. 4,9
EA has a long history in Traditional Chinese Medicine. It is similar to acupuncture, but instead of needles the therapist applies small herbal seeds or a magnetic ball to designated ear acupoints, which patients press to achieve a therapeutic effect. This technique is used to treat many disorders in China, including addiction. 10,11
Acupressure and meditation are self-applied treatment modalities and as such can complement existing addiction therapies. In this observational pilot study, it was found that IM plus EA showed encouraging results in dealing with the irritability, frustration, and other withdrawal symptoms of early abstinence when added to conventional treatment. This combined therapy will be referred to as IMEA (Integrative Meditation with Ear Acupressure).
The goal in this pilot Stage-I behavior therapy development study was to improve treatment outcomes for cocaine-dependent patients. The study objectives were to (1) explore the feasibility and acceptance of IMEA as an addition to regular outpatient addiction treatment; (2) determine whether adding IMEA to existing treatment increases retention; (3) investigate IMEA's effect on craving, anxiety, depression, and self-efficacy compared to treatment-as-usual (TAU) during a 12-week period.
Materials and Methods
Design
Qualified participants were stratified by gender, use of psychiatric medication, and polydrug use or cocaine only (8 strata) before being randomly assigned into either the IMEA or TAU group on a 1:1 ratio. Each participant went through 12 weeks of study and met with research staff weekly to monitor the treatment outcomes. The research protocol was fully reviewed and approved by the University of Maryland Institutional Review Board.
Participants
The study took place in an outpatient substance abuse treatment facility, part of the University of Maryland Medical System, Baltimore, MD. The facility, which treats about 350 patients a year, most of them (80%) heroin users and 50% of them cocaine or multiple drug users, has an intensive outpatient program (IOP) for drug and alcohol addiction.
Inclusion criteria were (1) diagnosis of cocaine dependence according to a checklist based on Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria 12 ; (2) cocaine or cocaine plus multiple drug use in the past 30 days; (3) 18 years of age or older; (4) willingness to adhere to the study protocol (e.g., provide urine samples and attend all visits and follow-ups); and (5) participation in the facility's IOP. Patients were excluded based on the following criteria: (1) at risk of suicide, including recent suicidal behavior or attempt in the past 30 days; (2) history of schizophrenia or other psychotic disorder; (3) pregnant or planned to be pregnant within 3 months; and (4) inability to read or understand English. Participation in the study was voluntary.
Of the 75 screened patients, 3 were excluded for various reasons; 72 were qualified and randomized to the IMEA+TAU or TAU-only control. Only 56 patients returned for study treatment after screening, for a total of 29 in the IMEA group and 27 in control. Figure 1 shows the participant flow chart specifying reason for exclusion and specific number of participants at each step. Participants received $10 for the time and effort of attending study sessions each week; payment was given in the form of gift certificates at the end of weeks 4, 8, and 12.
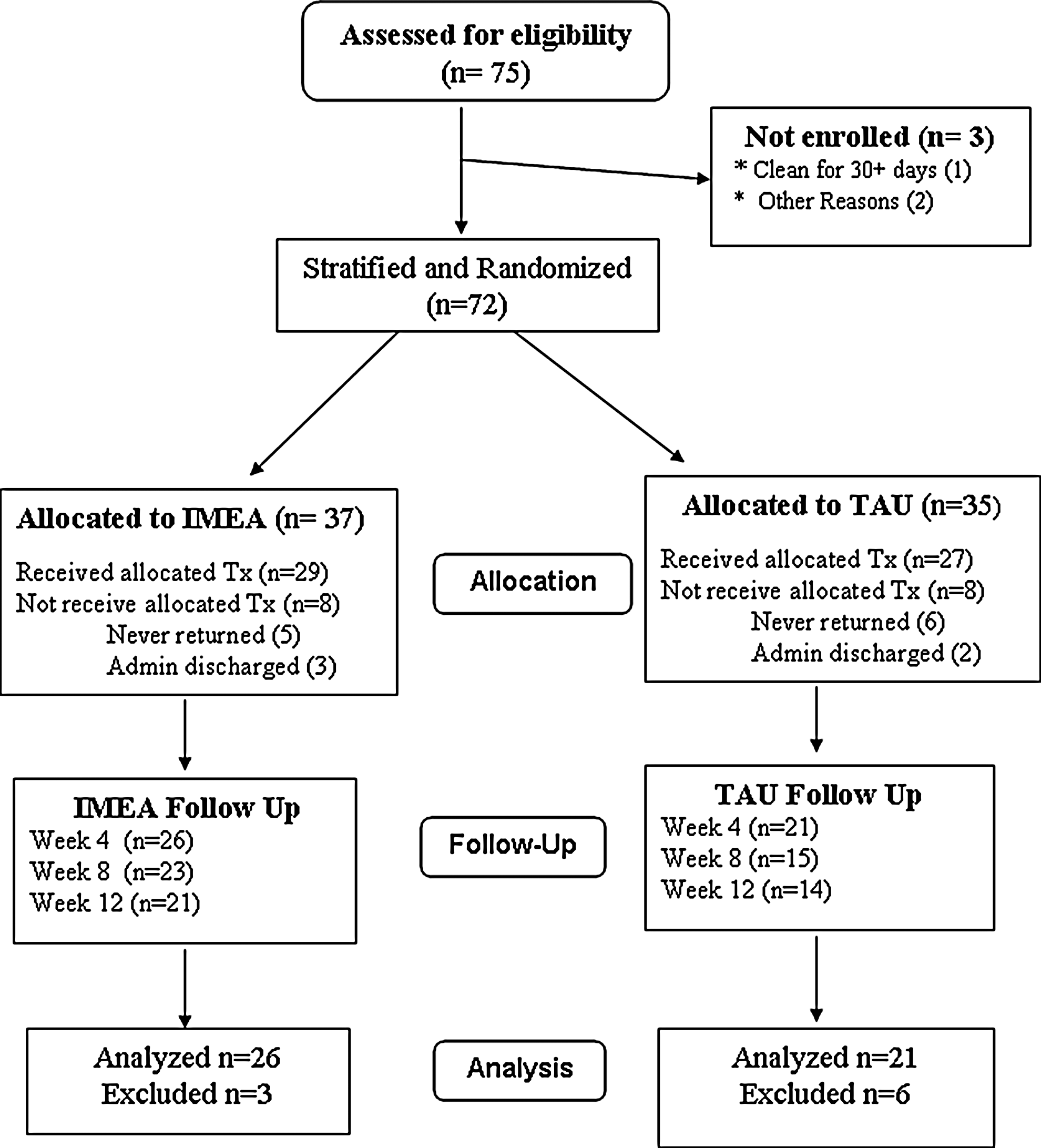
Participant flowchart. IMEA, Integrative Meditation and Ear Acupressure; TAU, treatment as usual.
Intervention procedures
All participants received TAU. Typically, IOP was 10+ hours per week (about 2 hours each day, 5 days a week) and encompassed such interventions as scheduled group or individual counseling, cognitive behavioral therapy, motivation enhancement therapy, human immunodeficiency virus education, relaxation training (such as t'ai chi), and buprenorphine (for opioid-dependent patients). The control group received TAU only but met with research staff weekly for study data collection.
EA
During detoxification, a modified version was used of the five-point ear protocol recommended by the National Acupuncture Detoxification Association for cocaine users—Shenmen, subcortex, heart, lung, and liver—to target major withdrawal symptoms. After informed consent, IMEA participants received the first acupressure treatment, in which trained staff taped three to five herbal seeds at the designated acupoints on one ear and taught participants to press each seed properly. Participants were instructed to press 20 times per session in 4–5 sessions a day for the first 2–3 weeks. A trained staff applied new seeds every week and checked the quality of the acupressure technique.
IM
EA, RF breathing, and IM were implemented interactively in three steps designed to complement TAU and enhance transition through the different stages of treatment (Table 1).
IMEA, Integrative Meditation and Ear Acupressure; RFB, resonant-frequency breathing; IM, Integrative Mind–Body–Breathing Meditation.
Although as a self-care therapy, meditation requires minimum counselor intervention, it was found to be difficult for some patients in the early stage of addiction treatment, when irritability and frustration are common. Thus, therapists introduced IM techniques in weekly facilitation periods, step-by-step based on feedback from the prior week. Participants were first taught abdominal breathing, 6 breaths per minute (near RF), and counseled to count their breaths whenever possible. As data indicate that the success of IM for cocaine addiction depends on the quality of the participant's daily practice as well as on facilitation, participants received an MP4 device with a customized RF breathing program of audio and visual aids to use at home for guidance in daily breath and meditation practice. This consisted of 15 minutes of abdominal breathing with eyes open, then progressing to 15 minutes of RF breathing with eyes closed, then to meditation: first 15, then 20, then 25 minutes. At each session the therapist would get feedback; teach new IM components for anxiety and relapse prevention; and link IM techniques to anxiety, addiction, and relapse prevention. The description of each facilitation session and accompanying homework is detailed in the therapist manual developed during the study.
Procedures for increasing compliance
Compliance is challenging in this type of study, given that patients with addictions usually have difficulty focusing. A series of procedures and aids was developed to increase acceptance and compliance: (1) weekly handouts summarizing the benefits of EA and meditation with a brief description of the techniques; (2) breath-counting, taught and integrated into daily life before meditation was begun; (3) a portable MP4 player with audio/video homework assistance; (4) EA to reduce irritability and withdrawal symptoms and increase focus during meditation; (5) weekly phone calls to remind participants about homework and get feedback; (6) weekly group meditation, offered to all facility clients, including nonparticipants; (7) special magnets for refrigerator or bedside to remind participants of homework; and (8) alternative methods for dealing with problems following the instructions.
Outcome measurements
Primary outcomes were treatment retention rate, urine screening (abstinence), and drug use assessment using a timeline follow-back procedure. 13
Secondary outcomes included number of sessions completed plus the following: (1) an adjective rating scale for withdrawal 14 ; (2) craving scale to evaluate the desire for cocaine or heroin in different situations 15 ; (3) Voris Cocaine Craving Scale 16 ; (4) Spielberger State–Trait Anxiety Scale (State only 17 ); (5) Beck Depression Inventory-II 18 ; (6) Sobell's Brief Situational Confidence Questionnaire 19 ; (7) Readiness to Change Scale: Drug and Alcohol Versions of SOCRATES 20 ; (8) Self-Efficacy Scale 21 ; and (9) adverse events checklist. Most of these instruments have been used in previous studies and have good validity and reliability.
To assess the quality of breathing and meditation, a feedback form was created on which IMEA participants reported daily practice, quantity, and quality. This form was used to gauge acceptance of the therapy and evaluate the degree of relaxation and tranquility during and after IM. 4
All outcomes were assessed at baseline and weeks 4, 8, and 12, with the exception of the timeline follow-back drug use report, urine test, and IMEA practice feedback, which were collected weekly.
Analytical strategy
The intent-to-treat principle was followed. All subjects randomized into treatment were included in the generalized estimate equations (GEE) model except for those who dropped out of the study before week 4, since there were no outcome evaluations until that point. Baseline differences in demographics, drug use, and main outcomes were analyzed with a χ2 test for categorical variables and an F-test for continuous variables to assess compatibility. To examine the significance of changes over time and possible group differences in key outcomes, a GEE model with control for potentially confounding variables was applied. As this model takes into consideration correlations among repeated measures and missing values without imputation, it is the most appropriate method for data from clinical studies with high dropout rates. SPSS (IBM Corporation, Armonk, NY) for Windows (version 18) was used to analyze the data.
Results
Baseline demographics and assessments
Of the 56 randomized participants, 57% were male, 94.7% African American, 50% never married, 58.2% were unemployed or laid off, and 66% had less than a high-school education. Table 2 presents baseline demographics, drug use, and outcome measures. There were no significant demographic differences between the groups except that on average, IMEA participants were 3 years older than those in TAU.
Chi-square test for categorical variable and F test in ANOVA for continuous variables.
TAU, treatment as usual (control); IMEA, Integrative Meditation and Ear-Acupressure.
Most participants (86%) considered themselves religious and 78% prayed for better health. Most believed that meditation is helpful (mean=7.8 on 1–10 scale), and were ready to change their cocaine use (mean=8.8 on 1–10 scale).
Regarding drug use and treatment circumstances, the main reason for entering treatment was self-referral (40%), followed by referral by court and probation officer (21%). On average, participants had used cocaine for 20+ years and had taken it 14.5 days of the past 30 and 2.4 days of the past week; 70% considered cocaine as their drug of choice (primary drug), 82% had multiple drug problems, and 75% also used heroin. The majority (78.6%) smoked crack cocaine and 68% tested positive in urine toxicology the week that they entered the study. There were no significant differences between the groups in baseline drug use measures or outcome measures used to assess treatment efficacy (Table 2).
Acceptance and primary outcomes
The IMEA program started with abdominal breathing and counting breaths, which patients could do easily anytime and anywhere, plus daily EA for relaxation and reduction of anxiety. Acceptance of these was relatively high, and the portable MP4 player with the video/audio RF breathing and meditation instruction was a great help for home practice. By the end of weeks 4 and 8, 80% of participants in the IMEA group self-reported doing their daily homework 5 or more days a week with minimum quantity (15 minutes or more daily), and 70% attained acceptable levels of quality by scoring 4+ on a scale of 1–7. Although previous studies of this population indicate that self-reports may be unreliable, most participants liked IM, and some even asked family members to practice with them. Only 1 did not want to continue IM after the study and returned the MP4 player; the rest chose to keep the player to continue the IM practice. A few TAU participants chose the MP4 player with IM instructions instead of the $30 gift certificate, as they wanted to try IM after witnessing its benefits in weekly group meditation.
Figure 2 shows retention rates of both groups by weeks 4, 8, and 12. Excluding those administratively discharged (n=3 in each group, e.g., transferred to inpatient or going to jail), 80.8% in IMEA completed the 12-week study compared to 58.3% in TAU (p=0.08). Significantly fewer IMEA participants dropped out of treatment by week 8 compared to those in TAU (88.5% versus 62.5%; p=0.03).

Participant retention rates over time by study groups. IMEA, Integrative Meditation and Ear Acupressure; TAU, treatment as usual.
In general, those in the IMEA group reported better primary outcomes than control, had a higher retention rate (Fig. 2), completed more study sessions (9.7 versus 7.6; p<0.05), and had a higher abstinence rate as measured by 6 or more consecutive weeks of negative urine tests for cocaine (65% versus 33%; p=0.06).
Other outcomes
Table 3 presents the results of standard outcome measurements frequently used to study addiction-related symptoms. Although the mixed-effect model can take repeated measures into consideration and censor dropouts without imputation, it cannot account for bias arising from the fact that those who dropped out of study were more likely to be those with more severe problems, while those who remained were more likely to have improved during treatment.
Numbers do not include dropouts before week 4. Ns in weeks 8 and 12 are smaller due to dropouts. This also affects the means, since those with problems or symptoms are more likely to drop out. Actual Ns in each mixed-effect model are around 118 due to repeated measures of the same outcome.
Mixed-effect regression models are estimated with baseline measure as a predictor, individual participant as a random effect, and with control for gender, age, and time as covariates.
SD, standard deviation; CI, confidence interval; IMEA, Integrative Meditation and Ear-Acupressure; TAU, treatment as usual (control).
There were significant differences or differences approaching significance between the two groups. IMEA participants reported greater reduction in craving (p=0.03) and anxiety states (p=0.09), as well as greater increase in situational confidence (p<0.01) in drug temptation settings and more self-efficacy (p=0.06), than did control. There were no significant group differences in depression, withdrawal symptoms, or the Voris cocaine craving scale. 16
Discussion
This is the first documented randomized controlled study assessing the feasibility and efficacy of adding meditation and EA to outpatient treatment of cocaine addiction. As a Stage-I behavior therapy–development study, the overall outcomes are very encouraging.
In general, the self-reported data indicate good acceptance of these self-care treatment components by these voluntary participants. With the assistance of a portable MP4 device and weekly phone reminders, 80% of IMEA participants reported that they were able to practice breathing or meditation 5+ days a week. Most participants showed strong interest in the techniques and learned to practice them at acceptable levels. Some continued IM after completion of the study.
Compared to TAU, IMEA participants were less likely to drop out of treatment, showing a significantly higher completion rate by weeks 8 (88.5% versus 62.5%) and 12 (81% versus 58%). They had higher abstinence rates for cocaine (66% versus 34%), and completed more study sessions (9.7 versus 7.6). They also reported significantly greater reduction in anxiety, craving, and other addiction-related symptoms, and significantly greater increase in self-efficacy and self-confidence.
Given the positive results, it is important to consider the strengths of this approach. The approach is theory driven, as participants learn to cultivate an internal frame of reference through daily breathing, acupressure, and meditation, which by themselves facilitate active behavioral coping skills and attitude change. The increased self-confidence and self-efficacy of the IMEA group support this point. In line with tension-reduction theory 22 and the consideration of negative mood as a primary precipitant of relapse, 23 IMEA is specifically intended to reduce physiologic arousal and facilitate relaxation and positive affect, thereby reducing the probability of relapse. Additionally, the participant learns to achieve tranquility, or “restful alertness,” 24 which is associated with activation of attentional systems and deactivation of thalamic input circuits. 25 This process helps rebuild attention networks and fosters self-reliance through internalized attention to keep the abstinent patient from relapse. Although future work is needed to study underlying mechanisms more explicitly, these treatment advantages are a useful starting point.
As a pilot trial, this study had some limitations. First, its small sample and homogeneous participants, primarily urban African Americans, limit the study's power for subgroup analysis and generalizability. Second, the control group did not receive an equal amount of treatment attention or contact time, as the primary goal of this therapy development study was feasibility and acceptance. Thus, the efficacy results are subject to the bias of nonspecific effects to an unknown degree, such as the placebo effects or “Hawthorne” effects. Third, only a DSM-IV checklist was used to qualify participants, not a full structured clinical interview for DSM-IV (SCID-IV) screening interview that includes comorbid psychiatric disorders. The latter would offer more information on what parts of the meditative therapy are and are not working in terms of comorbid mental health problems common in addiction patients. Finally, the study did not include a long-term follow-up to determine whether treatment benefits persist over time.
In the future, the authors would like to run more sophisticated clinical trials on a larger scale to further develop the proposed meditative therapy into the regular clinical program for addiction patients. The possible improvements to the current trial include applying a more compatible control condition (such as supportive counseling with journaling as homework assignment in comparison with active coaching and meditation) so that both treatment groups get the same attention and additions of new therapy components; using full SCID-IV to screen addiction patients so that we will know what type of psychiatric comorbidity responds to the new therapy, what type does not; and integrating the meditative component into the evidence-based Individual Drug Counseling manual for cocaine addiction so that this becomes an integrated part of the standard treatment program instead of an add-on or standalone.
Conclusions
In general, the study data suggest that IMEA may improve attention, reduce tension, and prevent relapse. As a self-care therapy, it may help patients switch from the traditional treatment pattern of seeking help outside from therapist, therapy, or facility to looking within (“I can do it myself”). Such self-responsibility is a key component for treatment success since it affects a root of addiction: the malfunction of attention networks. 26,27 This self-care feature makes IMEA complementary to existing treatment programs and potentially suitable for wide application to communities where access to treatment is a problem, thus increasing the capacity to meet the growing need for effective treatment of addiction.
Footnotes
Acknowledgments
This pilot study was partially supported by generous donations from Dr. Lucy R. Waletzky and from the Allman Brothers Band. We would also like to thank the following individuals for their assistance in study coordination or their contributions to therapy delivery and data collection during the study: Barbara Kandel, Margaret June Mangaali, Lynn Klimkiewicz, and Ginnea Morrison-Carver.
Disclosure Statement
All authors confirm that no competing financial interests exist.