
Abstract
Objectives:
Interdigital tinea pedis is the most frequent presentation, as well as the most severe clinical form of tinea pedis, constituting a therapeutic challenge. The aim of the study was to evaluate the effectiveness and tolerability of two concentrations of Ageratina pichinchensis extract (encecalin content, 0.76 and 1.52%, respectively) on patients with clinical and mycological diagnosis of chronic interdigital tinea pedis.
Design
Subjects:
One hundred and sixty (160) ambulatory patients of either sex between the ages of 18 and 65 years were enrolled.
Outcome measures:
The primary outcome variables were: clinical effectiveness, mycological effectiveness, therapeutic cure, tolerability, and treatment compliance. The secondary outcome variable was therapeutic success.
Results:
At the end of treatment, therapeutic cure was achieved by 34.1, 41.8, and 39.53% of Groups I, II, and III, respectively. No statistical difference between the groups was observed.
Conclusions:
Both treatments were effective for the treatment of interdigital-type tinea pedis, while better results were observed on patients that received the higher concentration of the extract.
Introduction
Ageratina pichinchensis (Kunth) R.M. King & Ho. Rob (Asteraceae) has been used in Mexican traditional medicine for treatment of skin diseases, principally superficial mycoses and pimples. 3,4 Eupatorium aschembornianum Sch. (Schauer) and Eupatorium bustamenta DC, (De Candolle) are described as synonymous. The antimycotic property of this plant was studied recently (2003), and by means of screening, nine medicinal plants (one of these A. pichinchensis) were evaluated in vitro against Candida albicans, Trychophyton rubrum, and T. mentagrophytes. Among the species included in the screening, A. pichinchensis showed the most important activity. 5 Through bioguided fractionation, different benzofurane compounds with antifungal activity were identified. 6 The main antimycotic activity has been attributed to encecalin, an acetylchromene compound identified on other plants from the Asteraceae family and that possesses activity against T. rubrum and T. mentagrophytes. 7
More recently, the antifungal property of this species has been also demonstrated by means of clinical trials. In patients with a diagnosis of onychomycosis, a nail lacquer formulation containing 5% and 10% extract of aerial parts of this plant demonstrated a therapeutic effectiveness of 71.9%. 8,9 In the present work, the results obtained from a randomized, double-blind clinical trial on selected patients suffering interdigital form of tinea pedis are depicted. Therapeutic effectiveness and tolerability of two concentrations (with encecalin contents of 0.76% and 1.52%) of A. pichinchensis extract were compared with 2% ketoconazole in topical treatment of patients with chronic interdigital tinea pedis.
Materials and Methods
Plant material
Ageratina pichinchensis (Kunth) R.M. King & Ho.Rob. (Asteraceae) was obtained from a controlled crop in Morelos state, Mexico. Dried and ground plant material (20.6 kg, leaves and stems) was extracted by maceration at room temperature with a solvent system consisting of n-hexane and ethyl acetate (7:3, 100 L) for 24 hours. The extract was filtered by using Whatman Grade No. 4 paper and concentrated by rotary evaporator (Heidolph Laborota 20) until a solid, dry material was obtained (672 g, 3.26%). This product (650 g) was submitted to a gravitational column with active charcoal (Merck). A mixture of n-hexane and ethyl acetate (7:3) was employed as eluent (8 L, 7 times). Depigmented extract (520 g) was dried under high vacuum.
Quantification of encecalin content in the extract
The main antimycotic activity of A. pichinchesis has been attributed to encecalin (Fig. 1), an acetylchromene compound. 7 Encecalin (98.97% purity) was used as monitoring compound. To quantify the encecalin content in the extract and in the phytopharmaceuticals, HPLC Waters equipment was used. Data obtained from the integrated area at 254 nm were used for the calibration curve (R 2 =0.99). Encecalin concentration in the depigmented extract was 152 mg/g.
Chemical structure of encecalin.
Treatment preparation
In order to prepare a pharmaceutical presentation, carboxymethylcellulose (Akucell 2201) was used as the base. Depigmented A. pichinchensis extract was added to the base until obtaining, on the first case, a 0.76% encecalin concentration, and in the second case, an encecalin concentration of 1.52%. Similarly, an identical control treatment was also prepared which contained ketoconazole (99% purity, Química Amer S.A de C.V., Mexico) with a final concentration of 2%. The products were packed in 15-mL collapsible tubes. Afterward, tubes containing the treatments were packed individually into cardboard boxes identified with the project number and a consecutive folio number.
Subjects
One hundred and sixty (160) patients of either sex between the ages of 18 and 65 years were enrolled in the study. For study inclusion, all patients must have presented two or more of the following signs and symptoms in the toe web: erythema, desquamation, fissures, pruritus, maceration, erosions, or malodor. With the aim of measuring the intensity of symptomatology, a 4-point severity scale was employed: 0=absent; 1=very mild; 2=mild; 3=moderate; and 4=severe. Grades for each symptom and sign were added together to make up a “total score.” A direct examination was carried out (mycological diagnosis) to integrate study inclusion criteria. This test consisted of direct identification by microscopy of filaments present in a sample of desquamation that was treated with potassium hydroxide.
Patients with diabetes mellitus, severe onychomycosis, immunodeficiency, or who had recently received treatment for tinea pedis, as well as pregnant women or women who were breast-feeding, were not included in the study.
Three (3) study groups were organized, with treatments assigned to patients based on a randomized numbers table. Patients in Group I (n=55) were treated with the phytopharmaceutical containing the extract with the lower concentration of encecalin (0.76%), patients assigned to Group II (n=54) received the treatment with the higher concentration of encecalin (1.52%), while Group III (n=51) received 2% ketoconazole. All treatments were administered once a day for 4 weeks.
To evaluate clinical evolution, tolerability, and treatment compliance, all patients were followed up twice during 4 weeks.
At the end of treatment, another skin sample was obtained with the aim of submitting this to direct examination and identifying the presence or not of the fungus.
The primary outcome variables evaluated were the following: (1) clinical effectiveness (no signs or symptoms of interdigital tinea pedis, or the presence of only one sign or symptom that was mild to very mild in intensity); (2) mycological effectiveness (no data of the presence of fungus by means of direct examination); (3) therapeutic cure (clinical effectiveness plus mycological effectiveness); (4) tolerability (no severe side-effect effects that required withdrawal from treatment), and (5) treatment compliance (87% administration of the treatment along the 4-week trial). The secondary outcome variable was therapeutic success (therapeutic cure plus tolerability).
Statistical analysis
Baseline and final data were submitted to statistical analysis. Frequencies, media, and percentages were used. The χ2 test was utilized for comparison between treatment groups. Values of p<0.05 were considered for establishing statistical difference.
Results
A total of 160 patients were included; among these, 33 (20.63%) patients withdrew from the study because of personal causes unrelated to the treatment or to clinical evolution. One hundred and twenty-seven (127) patients concluded the treatment: 41 (32.29%) patients from Group I (lower concentration), 43 (33.85%) patients from Group II (higher concentration), and 43 (33.85%) patients from Group III.
Analysis of patients showed that the median age was 45 years; there were more females, with a total of 101 patients (63.12%). Chronic evolution of the disease was found in all patients included, while 145 patients (90.62%) showed interdigital tinea pedis complex.
Based on the scale employed to evaluate signs and symptoms intensity, evolution was recorded in all groups during the 4-week treatment. As shown in Figure 2, patients had a mean of 8.6, 8.7, and 8.6 points (Groups I, II, and III, respectively) before treatment (no statistical differences between groups were observed). These values were reduced after 2 weeks of treatment (7.81, 7.78, and 7.57 points, respectively). Nevertheless, a favorable and consistent improvement was evidenced during the last 2 treatment weeks (3.45, 2.86, and 2.47 points, respectively). Evolution was similar between both groups, without statistical differences (p<0.54).
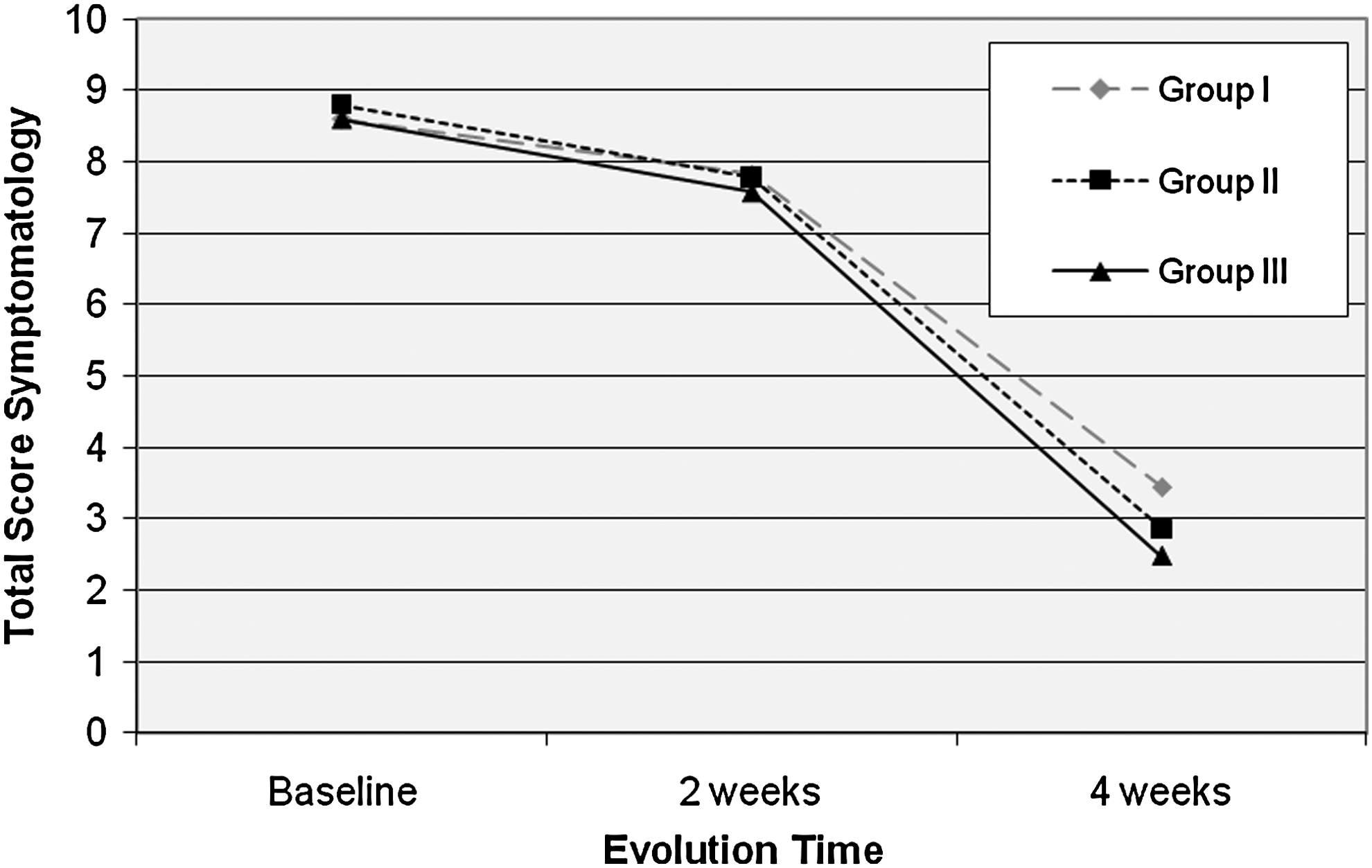
Clinical evolution (signs and symptoms intensity) in patients with interdigital tinea pedis during 4 weeks of treatment with the Ageratina pichinchensis extract with a concentration of 0.76% encecalin (Group I), 1.52% encecalin (Group II), and 2% ketoconazole (Group III).
Table 1 illustrates the patients' signs and symptoms before and at the end of treatment. In all cases, diminution of the percentage of patients with symptomatology was observed; notwithstanding this, no statistical difference was evident between treatments.
Before treatment, the predominating clinical stage of the disease was moderate, without statistical differences between groups (p=0.55). Once the treatment concluded, in all groups the very mild disease stage predominated; among Group I, this was 39.02% (16), while in Group II this was 39.53% (17), and in group III this was 44.18% (19) without showing statistical difference. The persistent sign with the highest proportion among patients was desquamation.
At the end of the study, analysis of the results showed that clinical effectiveness was reached in 39.02% (16) of patients from Group I, in 48.8% (21) of patients from Group II, and 46.51% (20) of patients from Group III. Mycological effectiveness was achieved in 68.29% (28), in 72.09% (31) and 76.74% (33) of patients from Groups I, II, and III, respectively. Therapeutic cure was achieved in 34.14 % (14), 41.8% (18) and 39.53% (17) of Groups I, II, and III patients, respectively. Although results were favorable for the treatment with the higher concentration of encecalin, no statistical difference was evidenced between groups (Table 2).
No patients exhibited moderate-or-severe side-effects, and it was not necessary for any patient to withdraw from the study. Therefore, the total sample showed 100% tolerability. In both experimental treatments, 1 patient was identified with short-duration pruritus (48 hours) after treatment administration. Treatment compliance was 87.8% for Group I patients, of 81.3% for those of Group II, and 84.3% for Group III, without statistical difference between groups. Because tolerability was 100%, the values of therapeutic success are the same as those for therapeutic cure.
Discussion
Commonly, a skin infection produced by fungus formerly received first-choice treatment with imidazoles, allylamines, butenafine, tolnaftate, salicylic acids, tolcicate, and undecylanic acid, and sometimes by oral route with terbinafine, itraconazole, or fluconazole. 10 Nevertheless, when Gram-negative bacteria are involved in tinea pedis, the use of topical imidazoles is generally ineffective. Even systemic therapy of the interdigital variety with griseofulvin and ketoconazole is not recommended because mycological cure indexes are very low and relapses are common. 11 Because interdigital tinea pedis frequently involves bacterial growth, the use of broad-spectrum antifungals with antibacterial effectiveness is recommended. This situation is especially favorable for extracts obtained from medicinal plants, because the variety of compounds in these products could also possess antibacterial effectiveness. In previous clinical research on patients with a diagnosis of onychomycosis, a nail lacquer formulated with the standardized extract of A. pichinchensis administered topically reached a clinical effectiveness of 71.9%. 8,9 In the present study, patients were selected with diagnoses of interdigital-presentation tinea pedis, which, as previously reported, presents major therapeutic difficulty; consequently, the standardized extract of A. pichinchensis reached clinical effectiveness of 39.02% and 48.8% with an encecalin concentration of 0.76% and 1.52%, respectively, while therapeutic cure (clinical and mycological effectiveness) was 34.14% and 41.8%, respectively. These values are comparable with other reported results from clinical trials carried out with widely known antifungal products: butenafine (23%); 12 oxiconazole (38.8%); 13 ciclopirox (20%, 4-week treatment; 50%, 8-week treatment). 14 Until now, encecalin has been found to be the most active compound (against T. rubrum and T. mentagrophytes) isolated from A. pichinchesins; nevertheless, other chromenos and benzofuranes, identified in this plant species, have been shown to possess bacteriostatic and antifungal effects. Rios et al. (2003) isolated and identified different benzofurane compounds that exhibited antifungal activity: 5-acetyl-3β-angeloyloxy-2β-(1-hydroxyisopropyl)-2,3-dihydrobenzofurane, 5-acetyl-3β-angeloyloxy-2β-(1-hydroxyisopropyl)-6-methoxy-2,3-dihydrobenzofurane, 4-hydroxy-3,5-diprenylacetophenone, espeletone, and encecalinol. 6 Lock reported that encecalin, the main active compound present in the A. pichinchensis extract, possesses a phototoxic and antibacterial effect. 15 Moreover, the plant extract contains numerous compounds that could exhibit bacteriostatic or bactericide activity, therefore contributing to making this plant extract more efficient in the treatment of interdigital tinea pedis.
Conclusions
It is possible to conclude that the A. pichinchensis extract was effective for topical treatment of interdigital-type tinea pedis and, despite its having evidenced major effectiveness with the higher concentration of encecalin, it has not been possible to identify a statistical difference between the concentrations utilized.
Footnotes
Acknowledgments
This project was supported by the Programa Sectorial de Salud y Seguridad Social del CONACyT-México, project (SALUD-2008-CO1-87736), as well as by Fondo de Investigación en Salud of Instituto Mexicano del Seguro Social project FIS/IMSS/PROT/077.
Disclosure Statement
No competing financial interests exist.