
Abstract
Objectives:
Complementary and alternative medicine (CAM) use by patients could interact in unpredictable ways with conventional therapies. This trial was designed to study the prevalence, types, and clinical implications of CAM use in patients with cancer who are receiving radiotherapy.
Design:
A validated questionnaire was given to consenting outpatients in this ethics-approved study. Questions specified types of CAM used, clinician knowledge, reason for use, perceived effectiveness, safety, and cost.
Results:
Of the 101 assessable questionnaires, 38 patients (38%) of the total patient group used CAM, with vitamins (53%), antioxidants (29%), spiritual/meditation practices (29%), and herbs (18%) being the most commonly used. The intention of CAM use was to improve quality of life in 69% of patients and for either hope of cure or to assist other forms of treatment in 26%. The majority of patients (58%) were using CAM prior to their diagnosis of cancer, with 40% starting at diagnosis or during conventional treatment. Patients spent up to $300/month on CAM use. Patients using CAM were significantly more likely to also receive chemotherapy versus non-CAM users (45% versus 24%, p=0.045). Significantly fewer CAM users expected cure from conventional therapy, compared to non-CAM users (50% versus 75%, p=0.016). More CAM users expected conventional therapy to prolong life (58% versus 32%, p<0.001). Only 40% discussed CAM use with their oncologists.
Conclusions:
CAM is commonly used by patients with cancer. CAMs, particularly antioxidants, are being taken which could negate the underlying free-radical tumorcidal effects of radiotherapy. Oncologists need to have greater awareness of this use and of its potential adverse consequences.
Introduction
The first purpose of the current study was to determine the prevalence of CAM usage by outpatients attending the Radiation Oncology Queensland clinic in a regional Australian radiotherapy setting. Like the 2001 New Zealand Regional Cancer Centre study, 6 the current study tried to identify types of CAM being used, reasons for use, satisfaction, and financial cost of CAMs.
A further goal of the current study was to assess the disclosure of patients' CAM use to oncologists. In addition, the study also focused on disclosure of CAM usage to general practitioners (GPs). The current authors intended to compare this study with previous studies, investigate discourse between patients and doctors about CAM use, and explore any potential interactions of CAMs with radiotherapy.
Materials and Methods
After obtaining informed consent, outpatients attending the Radiation Oncology Queensland, Toowoomba for Radiotherapy clinic between April and July 2009 were offered a self-administered questionnaire by receptionists or nursing staff members. The questionnaire was based on one previously validated in a New Zealand regional cancer treatment center. 5,6 The questionnaires were anonymous. This study was approved by the Toowoomba and Darling Downs Human Research Ethics Committee.
The questionnaire (see Appendix 1) was designed to gather information about demographics, disease- and treatment-related data, and the expectations of patients regarding conventional biomedical therapy. CAM users were asked to indicate the types of CAM used, timing of initiation of CAM use, reasons for CAM use, perceived CAM effectiveness, and any side-effects the patients attributed to the CAMs. Patients were also asked about discussing CAM use with their oncologists, GPs, and other doctors, and were asked to provide estimate of the monthly cost of the CAMs used.
Data were entered into an Excel XP spreadsheet (Microsoft, Seattle) and analyzed using SPSS, version 17. Associations between CAM use and patient characteristics were assessed by a chi-square test for categorical variables and a Student's t-test for continuous variables. A p-value of <0.05 was considered potentially significant.
Results
One hundred and forty (140 questionnaires) were distributed and 102 returned (a 73% response percentage). Two (2) patients declined to take a questionnaire. One survey was excluded from the study because it contained incomplete data. One hundred and one (101) participants' responses were therefore included in the analysis.
Table 1 shows the patients' characteristics. Ages ranged between 23 and 87, with a median age of 68. The majority of the respondents were Caucasian (92%) and male (64%). The most common diagnosis was prostate cancer (39%), followed by breast cancer (22%). There were no significant differences between CAM users and nonusers with respect to age, gender, ethnicity, employment, or cancer diagnosis.
CAM, complementary and alternative medicine, pop, population.
Of all patients, 91% were currently receiving conventional oncology therapy. Among these, 98% received radiotherapy, 32% chemotherapy, and 26% hormonal therapy. The remaining 9% of patients had completed treatment and were under observation. Some respondents indicated more than one expectation for conventional treatment. Sixty-six percent (66%) of patients had the expectation that conventional treatment would cure their cancer, 34% expected that conventional treatment would control the cancer and prolong life, and 17% expected that conventional treatment would reduced symptoms and improve quality of life (QoL).
Use of CAM
Of the 101 respondents, 38 indicated that they used at least one form of CAM. Of the CAM users, approximately two thirds used more than one type of CAM therapy. Figure 1 shows the types of CAM therapy used by patients. The four most common therapies were vitamins (53%), antioxidants (30%), spiritual practices (30%) and herbal remedies (18%). Only 2 patients used spiritual practices as their only CAM.
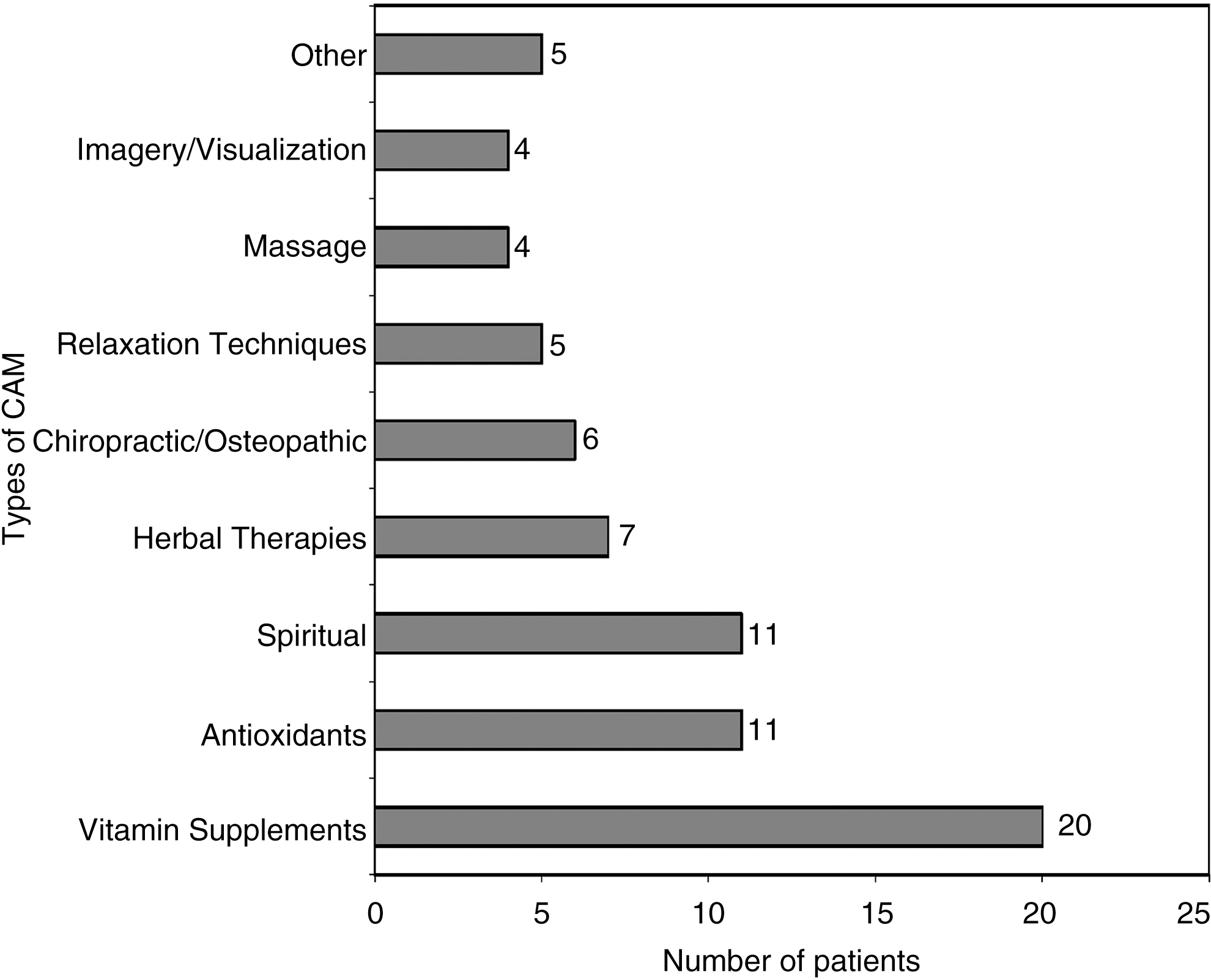
Number of patients using complementary and alternative medicine (CAM) therapies.
Initiation of CAM use
Of the 38 CAM users, 58% were already using these therapies prior to being diagnosed with cancer. Forty-two percent (42%) commenced using CAM after diagnosis or during conventional treatment. Similar ratios on timing of initiation of use were apparent for patients specifically using vitamins (80% versus 20%) and antioxidants (73% versus 27%), but were reversed for patients using herbal preparations (17% versus 83%).
Table 2 shows sources of information for CAM. Family (32%) and friends (37%) were the most common sources of information on CAMs. Of the health professionals, doctors were the most common source of information (29%) with nurses and pharmacists making up 5% each. More than two thirds of patients (68%) reported improvement of QoL as the reason for taking CAM. Thirty-one percent (31%) of users were taking CAM to control the cancer or prevent recurrence. More than one quarter (26.3%) were taking CAM with the hope for a cure (Fig. 2).
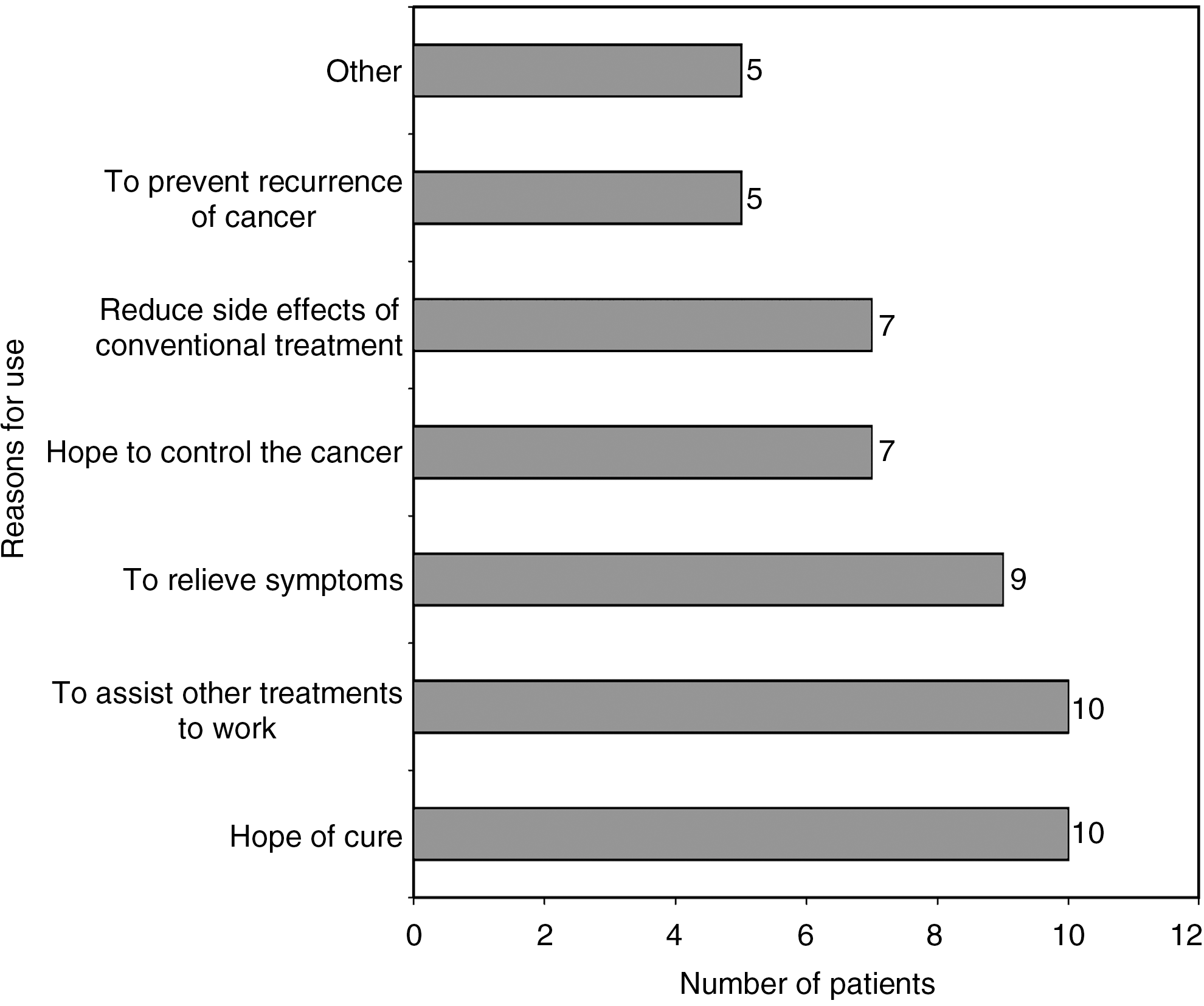
Reasons why patients use complementary and alternative medicine.
CAM, complementary and alternative medicine.
Patient characteristics associated with CAM
CAM users were more likely to be treated with chemotherapy (45% versys 24%, p=0.045). Those patients whose expectation was achieving a cure from conventional therapy were significantly less likely to use CAMs than those who did not have this expectation (50% versus 75%, p=0.016). Patients who expected conventional therapy to prolong life rather than effect a cure were significantly more likely to use CAMs (58% versus 32%, p<0.001).
Helpfulness and safety of CAMs
On a Likert scale of 1–5, with 1 being “not at all helpful” and 5 being “extremely helpful,” the CAM users' median rating of helpfulness was 3. Twenty-two percent (22%) rated CAM use as “not helpful” (rating 1 or 2); however, 36% rated CAM usage as “very” or “extremely helpful” (rating 4 or 5) for treating of their cancers. Ninety-two percent (92%) of CAM users responded that CAM usage was “safe.” No patients attributed any side-effects from their CAM therapies.
Discussion with medical practitioners
Of CAM use in general, 40% of patients discussed usage with their oncologists and 60% with discussed it with their GPs. Thirty-two percent (32%) discussed CAM usage with both their oncologists and GPs, while 32% had discussed it with neither.
Costs
Of CAM users, 23 (59%) estimated their average monthly expenditure on CAMs. They were not asked specifically to add in costs such as travel and practitioners' fees. Expenditure ranged from USD$10–$315 a month, with a median amount spent being USD$37 a month and the average USD$68.
Discussion
Patients are taking CAMs under the possible misconception that they are completely safe from both short-term obvious side-effects, but also longer-term, more-subtle interactions with conventional treatments. Ninety-two percent (92%) of CAM users in the current study believed that their CAM usage was completely safe, with no CAM user feeling CAMs were unsafe. Antioxidants may be safe under normal circumstances; however, the same claim cannot be definitively stated for usage while undergoing radiotherapy or chemotherapy. There is controversy regarding antioxidants and cancer treatment, with one researcher strongly suggesting that antioxidants are beneficial adjuncts to radiotherapy and chemotherapy, 7 while another's recommendation is against the use of these as possibly harmful products until better clinical evidence emerges. 8 Many oncologists have a more-relaxed attitude about CAM usage for patients who are seeking palliative help compared to those who are being treated with a curative intent. 9
Radiotherapy works, in part, by formation of intracellular free-radicals, such as the hydroxyl ion. This causes DNA strand breaks, and if this damage exceeds the cell-repair capacity, the eventual result is cell death. 10 The body has natural defenses against this oxidative stress, such as the reducing enzyme superoxide dismutase. Antioxidants act as free-radical scavengers in vivo, muting the cytocidal effect of radiation in free-radical creation. There is evidence that administered antioxidants such as amifostine, 11 albana, 12 carnitine, 13 and Ginkgo biloba, 14 are radioprotective. A study on the effect of combining vitamin E and radiotherapy in mice showed a reduced radiosensitivity in the tumor cells. 15 This clearly has implications for patients who are undergoing radiotherapy treatment and simultaneously using antioxidants.
A randomized clinical trial in 540 patients with head and neck cancer undergoing radiotherapy showed a marked reduction in overall severe adverse effects during radiotherapy (19% versus 25%) in patients randomized to receive the antioxidants vitamin E and [[[Greek beta]]]-carotene. 16 However, the mortality results from all causes was increased in the supplemental arm 3.5 years after the end of recruitment (37% versus 29%). 17 While these follow-up results showed an increase in the rate of second primary malignancy during the period of supplementation (treatment +3 years), paradoxically, the second primary malignancy rate was much lower than in a placebo group after cessation of supplementation. At 8 years, both groups had equivalent rates. 18 In addition, a systematic review of 280 peer-reviewed articles on concomitant nutrient use with chemotherapy and/or radiotherapy concluded that antioxidants enhanced the therapy. 19,20 Clearly, the data to date are inconclusive regarding the risks and benefits of antioxidants, therefore further research is needed in this field to clarify the interaction between radiation and antioxidant supplements.
Vitamins and antioxidants were the most commonly used CAMs in the current survey. This finding is consistent with the New Zealand study and that of CAM usage by patients with breast cancer. 6,21 This shows a possible shift from a 1995 Australian study on patients with cancer, which showed dietary and psychologic methods as the most common CAMs utilized. 5 However, many compounds not specifically labeled as antioxidants, such as vitamins and herbs, produce significant antioxidant activity, hence, the true incidence of antioxidant use is likely to be much higher. The real concern is that many patients are taking medications, such as antioxidants, which can, at least theoretically, directly counteract the anticarcinogenic effects of radiotherapy and some chemotherapy. It should also be acknowledged that antioxidant compounds, such as quercetin 22 and the lipophilic derivative of vitamin C 23 may act as prooxidants depending on the concentration taken. In any event, this therapy is being used by patients, often without their oncologists' knowledge.
What are the reasons for nonreporting of CAM use to oncologists? The conventional medical paradigm may not be a good fit with the patient's view of health and disease. CAM has an emphasis on the concept of a vital force that is different from—and greater than—the physical and chemical forces of the organism, emphasizing a mind–body connection or the notion of holism. 24 Fear of oncologists' disapproval has been shown to be a reason for nondisclosure 5,25 of CAM use and of a reason why some patients with terminal cancer patients not taking CAMs. 26
Do doctors know what their patients are taking? Past work has shown that patient disclosure of CAM use to oncologists is in the range of 40%–60%. 4,5 In line with these findings, the current study found a disclosure rate of 40% to patients' oncologists. This low disclosure rate is not unique to the specialty of oncology. A study by Harrigan published in January 2011 highlighted that only half of CAM-using women attending specialist obstetrical and gynecology services disclose CAM usage to their physicians. 27 Given the potential for such treatments to interact with radiotherapy, it would seem prudent for all physicians to build better rapport with their patients in this regard.
In a self-reported study on oncologists' views on CAM, Newell and Sanson-Fisher 28 found that only 25% of respondents reported a good knowledge of common CAMs. The majority reported gaps in their knowledge of unconventional therapies. There is supporting evidence for the use of certain CAMs, such as acupuncture and hypnosis, to reduce the nausea and vomiting associated with chemotherapy. 29 There has also been a recent trial showing a significant increase in immune response to concomitant relaxation and guided imagery in patients with breast cancer undergoing multimodality conventional therapy. 30 Auricular acupuncture has been shown to reduce cancer-related pain. 31 Three studies have supported the use of hypnosis/relaxation/imagery interventions for symptom relief in patients with cancer requiring advanced palliative care. 32 Despite this, these CAMs were not commonly used in by the patients in the current study or those in the New Zealand study. This suggests that evidence-based assessments of CAMs used in oncology should be more widely disseminated among health care professionals and their patients.
The current study showed that 38% of the patients with cancer surveyed reported using at least one form of CAM, with two thirds of these patients using more than one form of CAM. The methodology is open to selection bias because the survey was voluntary and anonymous. Given that the survey was performed in a radiotherapy center, patients who chose CAMs as their sole treatment for cancer were also not represented. The current study's results of CAM use are consistent with a multicountry review showing an average prevalence rate of 31% for CAM use in adult patients with cancer. 3 The 2007 study of Western Australian patients cancer showed the prevalence of CAM usage in that population to be 30%, 33 which is lower than the estimated CAM usage by the Australian general population of 50%. 23
A survey of Australian radiotherapy departments found that 60% of the respondents recommended psychosocial CAM modalities, such as relaxation and meditation. 34 This was supported by a study looking at the attitude of integration of CAMs by GPs. 35 More than 65% of the 664 Australian GPs surveyed responded that acupuncture, hypnosis, meditation, and massage were beneficial and safe. The researchers surmised that this was because doctors do not require as much personal knowledge about nonmedical therapies to support their use safely. These CAMs use a different healing paradigm and, therefore, have a low likelihood of interaction with conventional medical therapies.
The current study indicated the most common source of CAM knowledge/recommendations were family and friends (69%), with doctors being the most significant source of health professional advice about CAM (29%). The disclosure rate to patients' radiation oncologists was 40%; however, when GPs were included, the overall disclosure rate to any one doctor was >70%. This gives medical professionals an opportunity to advise patients regarding CAM use, and, hence, behooves the profession to improve its knowledge on the roles, safety, and interactions of such therapies.
Conclusions
The current study is the first to assess CAM usage in a predominantly rural and regional population as well as specifically in a radiotherapy department in Australia. CAMs are widely used and only sometimes discussed between radiation oncologists and their patients. Given the potential for hazardous interactions between CAM use and radiotherapy, the current authors suggest the following recommendations: 1. CAM usage should be specifically inquired about and recorded during the initial consultation. 2. Antioxidants, in particular, should be discussed. Their risk–benefit profile in radiotherapy is currently unknown. 3. The use of CAMs with radiotherapy requires further scientific clarification.
Footnotes
Acknowledgments
The authors wish to acknowledge the contribution of Dr. Richard Isaacs MB ChB, FRACP for permission to use the validated questionnaire of his study as the basis for the questionnaire used in this study as well as Daniel McDonald BA(Hons) a librarian at the Toowoomba Health Services, for his help with the literature search and technical preparation of this article.
Disclosure Statement
No authors of this article have any conflicts of interest to disclose.