
Abstract
Objectives:
Motion sickness (MS) is evoked by the conflict among somatosensory, visual, and vestibular input. Some of the MS symptoms and signs are mediated by activation of the autonomic nervous system (ANS). Transcutaneous electrical nerve stimulation (TENS), a maneuver used for pain control, was found to influence cardiovascular responses through ANS reflex, and to enhance motor function, visuospatial abilities, postural control, and cognitive function. The purpose of the present study is to investigate the effects of TENS on MS.
Subjects and design:
Fifteen (15) healthy young men participated in a within-subjects crossover study. Each completed four test sessions (control, rotation, TENS, TENS+rotation) in randomized order. Rotary chair (120°/s) combined with pitch movement of the subject's head was used as a model to provoke MS. Whole rotation protocol consisted of 5 1-minute rotations, each separated by a 1-minute rest period. TENS protocol involved simultaneous electrical stimulation of posterior neck and Zusanli acupoint.
Outcome measures:
Motion sickness susceptibility was rated on a standardized questionnaire (Motion Sickness Susceptibility Questionnaire). Motion sickness symptoms, blood pressure (BP), skin temperature, heart rate (HR), and heart rate variability (HRV) were measured. Saliva samples were collected to analyze the level of stress markers. Cognitive function was evaluated with d2 test prior to and after MS provocation.
Results:
Spinning by itself significantly decreased task response speed and contraction. MS symptom scores, BP, as well as the sympathetic parameter of HRV increased progressively with MS provocation (p<0.05), but skin temperature decreased (p=0.023). Severity of MS symptoms significantly decreased with TENS intervention (p<0.05). After TENS treatment, subjects were able to concentrate better and showed fewer errors in a cognitive test. Salivary cortisol concentration significant decreased after TENS treatment.
Conclusions:
Sympathetic activity increased but parasympathetic activity decreased during MS. TENS was effective in reducing MS symptoms as well as alleviating cognitive impairment.
Introduction
Prevention or medical treatment of MS symptoms, especially nausea and vomiting, are usually appropriate for general passengers. However, for professional travelers, certain side-effects such as dizziness, blurred vision, and dryness of mouth are easily confused with the symptoms of MS and are unacceptable in terms of mission effectiveness. 6 Some intolerable side-effects such as central sedation, impaired ocular motility, hand–eye coordination, or tracking tasks could decrease performance and possibly jeopardize safety. 6,7 As drug absorption is impaired during MS because of marked reduction in gastric motility, orally administered anti-MS medications must be given before exposure to motion to be effective. 7 Another drawback of currently available anti-MS drugs is an anticipation of prophylactic need because most of their peak plasma levels are not reached until several hours after administration.
In order to overcome these problems with pharmacologic treatment, several alternative medicine remedies are recommended for treatment of MS. Among these, acustimulation to the Neiguan (P6) acupuncture point suppressed MS symptoms of nausea and vomiting in a rotating optokinetic drum paradigm. 8 However, use of an acupressure band that involves self-applied continuous pressure on the P6 (or Nei-Kuan) point failed to increase tolerance to MS. 9 It is thus suspected that continuous vigorous stimulation of the P6 point is required to achieve significant benefit. From this perspective, continuous electrical stimulation through cutaneous electrodes may be worthy of study. Transcutaneous electrical nerve stimulation (TENS), a maneuver used for pain control, was found to influence cardiovascular responses through ANS reflex, and to enhance motor function, visuospatial abilities, postural control, and cognitive function. 10,11 The aim of the present study is to investigate the effects of TENS on MS.
Materials and Methods
Subjects
Fifteen (15) healthy, nonsmoking, young men were recruited for this study. All subjects were screened for vestibular, visual, cardiovascular, respiratory, and gastrointestinal tract disorders. The study protocol was approved in advance by the Institutional Review Board. Each subject provided written informed consent before participating. All procedures followed were in accordance with the declaration of Helsinki and ethical standards of a human research advisory committee. Subjects were instructed to refrain from the use of medication, alcoholic substances, and caffeinated drinks for 24 hours before and at the time of each study session. They were requested to be well rested and to fast 8 hours before each study session. To compensate for any learned behaviors, sessions were spaced at least 1 week apart. All testing was performed between 8
Experimental protocol and instrumentations
A within-subjects crossover design was used wherein each subject was asked to complete four test sessions (control, rotation, TENS, TENS+rotation) in randomized order. Each session consisted of four phases, and physiologic parameters were recorded throughout the whole session: Phase 1 (10 minutes), preparation and recording of baseline physiologic parameters; phase 2 (10 minutes), electrical stimulation (for TENS and TENS+Rotation sessions); phase 3 (10 minutes), MS stimulation (for Rotation and TENS+Rotation sessions); phase 4 (30 minutes), post-test period (Fig. 1). Prior to the test session, MS susceptibility of all subjects was evaluated with the Motion Sickness Susceptibility Questionnaire (MSSQ), the Chinese version of which had been validated. 12,13 The questionnaire recorded participants' previous everyday life MS experiences (e.g., different transportations, amusement park rides) during childhood (before age 12, subscale MSSQ-A) and during adulthood life (after age 12, subscale MSSQ-B). Frequencies of exposure to potential MS-provoking vehicles as well as symptoms were evaluated with a 5-point scale. Subjective MS symptom ratings were made verbally with Motion Sickness Symptom Ratings (MSSR). 13 The degree of severity of seven MS symptom (vertigo, headache, nausea, urge to vomit, tiredness, sweating, stomach awareness) were rated using a 6-point scale from 0 (not present) to 5 (very strong). The ratings were made at the end of phases 1–4 (R-20, R-10, R1, R30), halfway through phase 4 (R15), and after each 1-minute rotation in phase 3 (for Rotation and TENS+Rotation sessions only).

Schema of experimental time schedule. Open arrows indicate objective assessments and solid arrows indicate subjective assessment. Between R0 and R10, black bars indicate five 1-minute rotations, open bars indicate five 1-minute rests in between. MSSQ, Motion Sickness Susceptibility Questionnaire; MSSR, Motion Sickness Symptom Rating.
Motion stimuli
During phase 3, a Coriolis cross-stimulation paradigm (rotation combined with pitch movement of subject's head) was used to provoke MS. Rotation was induced using a custom-made rotary chair driven by an electric motor (Lucidem, Taiwan, ROC). The subjects were positioned and secured to the rotary chair with shoulder harness and waist belt. Their eyes were closed and their head position was kept upright and adjusted so that both lateral semicircular canals were close to the plane of stimulus. For rotation and TENS + rotation sessions, the chair rotated in clockwise motion about its vertical axis at a constant velocity of 20 rpm (angular velocity of 120°/s). The whole-rotation procedure consisted of five 1-minute rotations with 1-minute interruptions in between each rotation sequence. At 6-second intervals throughout the rotation period, the subject was prompted by audio cues to make forward head-pitch movements until his chin touched his chest and then to resume an upright posture. Each subject was rotated until the subject requested termination because of unbearable MS symptoms, could no longer elicit proper head movement, or the maximum duration of rotation (300 seconds) was tolerated. The tolerated rotation times (RT) were added to produce a total RT time (in seconds).
Transcutaneous electrical nerve stimulation
For TENS and TENS+Rotation sessions, electrical stimulation lasting 20 minutes (whole period of phases 2 and 3) was administered with a self-contained, battery-operated, dual-channel transcutaneous electrical nerve stimulator (SW320, SHINMED, Taiwan, ROC) at pulse rate 100 Hz. Per the manufacturer's instructions, the participants set the level of intensity (1–10) at the highest comfortable setting as intensity settings varies individually. Two (2) stimulation sites were chosen: (1) midline posterior nuchal region and (2) Zusanli acupoint, one finger breadth lateral to the tibia's anterior crest, about four finger widths below the knee.
Cognitive Function Evaluation
The d2 test was utilized for the assessment of cognitive function, more specifically visual attention, before and after each of the four sessions. The standardized paper-and-pencil test form consisted of a landscape layout of 14 test lines with 47 characters in each line. Each character consists of a letter, “d” or “p” marked with one, two, three or four small dashes. The respondent is required to scan the lines and cross out all occurrences of the letter “d” with two dashes while ignoring all other characters. Two (2) types of errors are calculated: errors of omission (missing characters that should have been crossed out) and errors of commission (crossing out characters that should not have been crossed out). The test results in the following norm-referenced scores: Total Number of items processed (TN, the sum of all items processed whether correctly or incorrectly), a highly reliable measure of processing speed; Percentage of Errors (E%, the proportion of errors made across all items processed), measurement of the qualitative aspects of performance; Total Number of items processed minus errors (TN-E), an indication of the implications of the combined speed and accuracy scores for attention and inhibitory control; and Concentration Performance (CP, the number of correctly processed items minus errors of commission), a check on distortion in response style. Prior to commencement of the study, all subjects were fully trained on the d2 test so the learning effect could be negligible. The test was performed before and after MS provocation.
Salivary stress biomarkers
Mixed unstimulated saliva samples were collected with a Salivette saliva collecting tube (Sarstedt, Nümbrecht, Germany) at each of the following time points: at the end of phases 1–4 (R-20, R-10, R1, R30) and halfway through phase 4 (R15). Samples were stored immediately after collection at 0°C and delivered to the laboratory on the next day where samples were frozen at −80°C until analysis. On the day of assay, samples were thawed completely, supernatants were collected, and salivary α-amylase (sAA) activity as well as cortisol concentration were measured according to the manufacturer's recommendations (Salimetrics Salivary α-amylase Assay Kit and Salimetrics Salivary Cortisol immunoassay kit, Salimetrics, USA).
Other measures
Each subject was instrumented with an automated blood pressure monitor (Tango+, SunTech Medical, USA). HR recording was obtained with the Polar system (RS 800 wrist unit and WearLink transmitter, Polar, USA). HRV was determined by forwarding HR data to Nevrokard LT-HRV software (Nevrokard Kiauta, d.o.o., Slovenia). Power spectrum analysis in the frequency domain was performed by fast Fourier transformation. Low-frequency power component (LF; 0.04–0.15 Hz), high-frequency power component (HF, 0.15–0.40 Hz), ratio of low-to-high frequency spectra power (LF/HF), high-frequency ratio (HF/LF+HF) and low-frequency ratio (LF/LF+HF) were derived. Skin temperature was recorded with thermometer through temperature probe (TM-903A, Lutron Electronics Enterprise Co. Ltd., Taiwan, ROC) pinched between the subject's thumb and middle finger, fixed with an adhesive band. These parameters were measured at the end of phases 1–4 (R-20, R-10, R1, R30), and halfway through phase 4 (R15). For HR, HRV analysis, and skin temperature, extra data were collected after each 1-minute rotation in phase 3 (for rotation and rotation+TENS sessions only).
Statistical methods
Nonparametric statistics were used to analyze the data. For comparison between sessions, a repeated-measures analysis of variance was used. Correlations between MSSQ and MSSR were assessed by Pearson's correlation coefficient. Data analysis was carried out using SPSS (version 15.0, SPSS, Chicago, IL). Results are reported as significant when p<0.05.
Results
Each of 15 healthy young men (ages: 23.8±0.62 years, height: 173.5±1.2 cm, body weight: 70.1±1.6 kg, body–mass index: 23.3±0.6) completed four test sessions (Control, Rotation, TENS, TENS+Rotation) in randomized order. Total tolerated rotation time was marginally prolonged by TENS treatment (Rotation, 277.1±9.6 s; TENS+Rotation, 286.6±8.4 seconds; p=0.059) and more people completed the whole 300 seconds of rotation challenge with TENS treatment than without (12 versus 10). The child score of MS susceptibility (MSSQ-A, 11.75±3.3) was significantly different (p=0.036) from but only moderately correlated with the adult score (MSSQ-B, 4.79±1.62) (r=0.48, p=0.069) (data not shown). Severity of MS symptoms as reflected by MSSR scores increased immediately after the first minute of rotation and continuously with the progression of rotation. MSSR scores were significantly lowered after TENS intervention (p<0.05; Fig. 2). There was strong correlation between MSSQ-B and MSSR during all five rotation sequences (p<0.01), while MSSQ-A only correlated with symptom scores of the fourth and fifth rotation (p<0.05) (Table 1).

Motion Sickness Symptom Rating scores in Rotation (filled circle) and transcutaneous electrical nerve stimulation (TENS)+Rotation (open circle) sessions. R-20, 20 minutes before rotation; 1st, 2nd, 3rd, 4th and 5th, rotation sequences. *p<0.05 compared with R-20; #p<0.05 compared with Rotation alone.
Motion Sickness Susceptibility Questionnaire (MSSQ-A): score A for childhood (<12 yrs); Motion Sickness Susceptibility Questionnaire-B (MSSQ-B): score B for adulthood (>12 yrs). 1st ∼ 5th: sequences of one minute rotations. Data are Pearson's correlation coefficients. * p<0.05, ** p<0.01*
An increase of blood pressure (systolic and diastolic blood pressure) and HR were observed after rotation. However, skin temperature decreased with the progression of rotation (Table 2). HRV analysis revealed that rotation suppressed high-frequency ratio (HF/LF+HF) and caused an elevation of low-frequency ratio (LF/LF+HF). Ratio of low-to-high-frequency spectra power (LF/HF) also progressively increased with the advance of rotation (p<0.05). These effects of rotation were all eliminated with TENS treatment (Fig. 3).
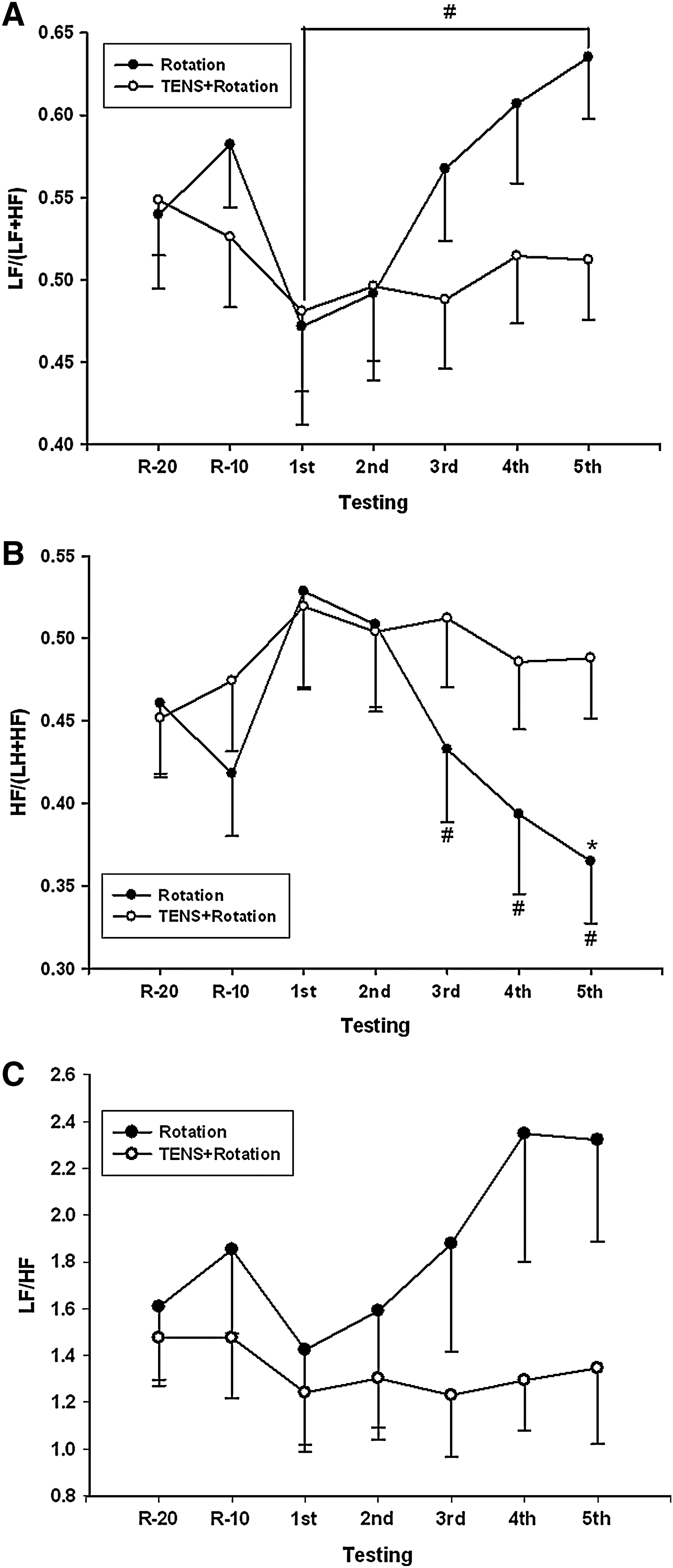
Low-frequency (LF) ratio
Continuous variables were presented as mean±standard deviation.
p<0.05 compared with baseline values.
SBP, systolic blood pressure; DBP, diastolic blood pressure; bpm, beats per minute.
Two (2) salivary stress biomarkers, α-amylase and cortisol, were evaluated to reflect acute and subacute stress responses from MS, respectively. Salivary α-amylase activity increased after rotation, although not reaching statistical significance (data not shown). TENS treatment did not change this trend. However, salivary cortisol concentration elevated significantly with Coriolis stimulation, and TENS treatment substantially eliminated such change (Fig. 4).

Salivary cortisol concentration changes (mean±standard deviation) in Rotation (filled circle) and transcutaneous electrical nerve stimulation (TENS) +Rotation (open circle) sessions. *p<0.05 compared with baseline (R-20) measurements. #p<0.05 between Rotation and Rotation+TENS treatment sessions.
With the development of MS, subjects' performance in the d2 test deteriorated, as reflected by smaller number of items processed (TN), increased percentage of errors (E%), and poor concentration performance (CP). After TENS treatment, subjects had more concentration in a cognitive test and showed less error. Specifically, processing speed and concentration increased while errors decreased (p<0.05) (Table 3).
TN, E%, TN-E, and CP are all parameters in the d2 test.
TN, total number of item processed; E%, percentage of errors; TN-E, total number of items minus error scores; CP, concentration performance.
p<0.05 compared with Control; ** p<0.05 compared with Rotation.
Discussion
The Coriolis cross-coupling stimulation paradigm had been used for assessing the efficacy of pharmacologic agents for terrestrial MS. Performance had been found to decline as MS developed in the subjects in the current study, in accordance with previous reports. 14,15 Such observation indicates that there is a clear need to find effective countermeasures. 16 –18 The authors adopted TENS as a new strategy for MS prevention. The primary finding from this study is that TENS was effective in reducing MS symptoms as well as negating the impact of MS on cognitive performance. While TENS has traditionally been used in alleviating pain, it was also reported to enhance motor function, visuospatial abilities, and cognitive function. 10,11 Results of previous studies with acupuncture, acupressure, and electroacupuncture for the prevention or treatment of MS had been controversial with success in some, 19 –21 but not all, 9,22 clinical trials. One possible confounder is the location of electrical stimulation. Two (2) sites with presumably different mechanisms of action were simultaneously stimulated to circumvent possible absence of effect with stimulating a single spot and to gain additive or synergistic responses. Electrical stimulation on the midline posterior nuchal region have been shown to improve visuospatial function in patients. 23,24 It is known that neck proprioceptive inputs plays a major role in body segment position and orientation in space and during locomotion. 25 Possible mechanisms of TENS could involve modification of proprioceptive signaling processes through vibratory stimulation of neck muscles. Zusanli acupoint was chosen because acustimulation of the Zusanli acupoint had been shown to enhance the regularity of gastric myoelectrical activity 26 and had been proven beneficial for chemotherapy-induced acute vomiting. 27
Past occurrence and severity of MS had been used to predict performance and susceptibility of MS. In this study, MSSQ, a published and validated instrument for Chinese population, was adopted to evaluate MS susceptibility. 13 Consistent with published data, the child scores were higher than adult scores, reflecting evolutionary habituation. 28 However, scores in the present study (MSSQ-A, 11.75±3.3; MSSQ-B, 4.79±1.62) were significantly different from published normative data by Golding (28.8±23.3 and 16.7±17 for MSSQ-A and MSSQ-B, respectively) and a study by Klosterhalfen et al., who compared ethnic differences in MS susceptibility between whites and Chinese (for Chinese subjects, both MSSQ-A and MSSQ-B scores were ∼20). 12,13 Possible explanations for such differences include difference in subject numbers, ethnicity, gender, test modality, and experimental designs. The present evaluated MS susceptibility on 15 male subjects, while Golding and Klosterhalfen had both male and female subjects (M:F 70:77 and 37:45, respectively). As women are generally more susceptible to MS than men, it is expected that the scores in the present study would be lower. 13 Ethnic and type-specific sensitivity to MS stimulation had been established. 28 Golding used only subjects of white origin. While Chinese subjects are more susceptible than whites to MS in a rotating optokinetic drum paradigm, the present study used the Coriolis cross-coupling stimulation paradigm to provoke MS. The results in this study supported the theory that susceptibility to MS is model specific. Correlation between MSSQ-A and MSSQ-B was only marginal (r=0.48, p=0.069) in this study, different from previous reports when 227 German and 82 Chinese subjects were tested (r=0.69, p<0.001). 13 Ethnic effects could not be ruled out in causing such disparity.
TENS treatment significantly ameliorated MS symptoms immediately after the first minute of rotation. TENS treatment per se did not significantly change BP, skin temperature, and HR as well as salivary stress biomarker levels. However, TENS treatment alone affected autonomic components of HRV (Table 4). In this model, sympathetic activity (low-frequency ratio, LF/LF+HF) is elevated and parasympathetic activity (high-frequency ratio, HF/LF+HF) is suppressed, with resultant dominance of sympathetic over parasympathetic activity (increased LF/HF ratio). One possible mechanism whereby TENS carries out its effect is by counteracting certain pathways stimulated by MS. The fact that TENS effectively ameliorated MS symptoms in parallel to its effect on HRV supports the above hypothesis.
SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; bpm, beats per minute; LF, low-frequency power; HF, high-frequency power; sAA, salivary α-amylase activity.
p<0.05 compared with Control.
Basal levels of salivary stress biomarkers had been correlated with MS tolerance in the experimental paradigm. 29,30 However, in the subjects in the present study, basal cortisol levels were not associated with severity of MS symptoms (i.e., MSSR scores), and hence not associated with MS tolerance (data not shown). One possible cause of such discrepancy is gender, since cortisol had been shown to predict MS tolerance in women but not in men. 31 Salivary α-amylase activity increased after rotation, although not reaching statistical significance. Gordon et al. have shown that salivary amylase activity was significantly higher in subjects susceptible to seasickness as compared with nonsusceptible subjects. 32 The present study's results could be explained by low susceptibility (i.e., smaller MSSQ scores) of the subjects, as stated earlier.
The present study has some limitations that need to be acknowledged. The small sample size and the study design with all young male subjects make it impossible to generalize the results to average MS sufferers. Autonomic responses to different MS models are not universal. Therefore, whether TENS treatment can be applied to other conditions such as virtual reality or optokinetic drum awaits future study. This study used crossover design without prescreening for susceptible subjects. It is possible that the effect of TENS could be averaged out. Testing the effect of TENS on model-specific MS-susceptible subjects might provide an answer.
Conclusions
In summary, with Coriolis stimulation, sympathetic activity increased but parasympathetic activity decreased during MS. TENS was effective in reducing MS symptoms as well as alleviating cognitive impairment.
Footnotes
Acknowledgments
This research was supported with funding from the National Defense Medical Center DOD97- 01-03.
Disclosure Statement
All authors declare that no competing financial interests exist.