
Abstract
Background:
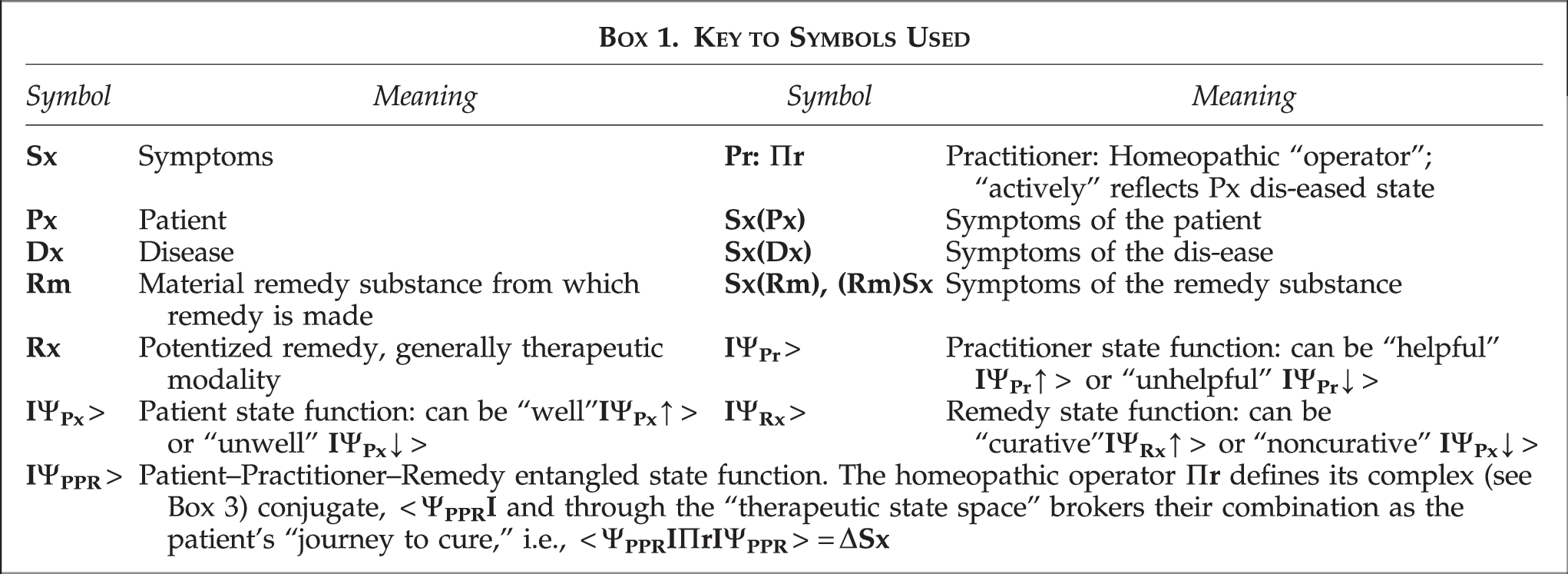
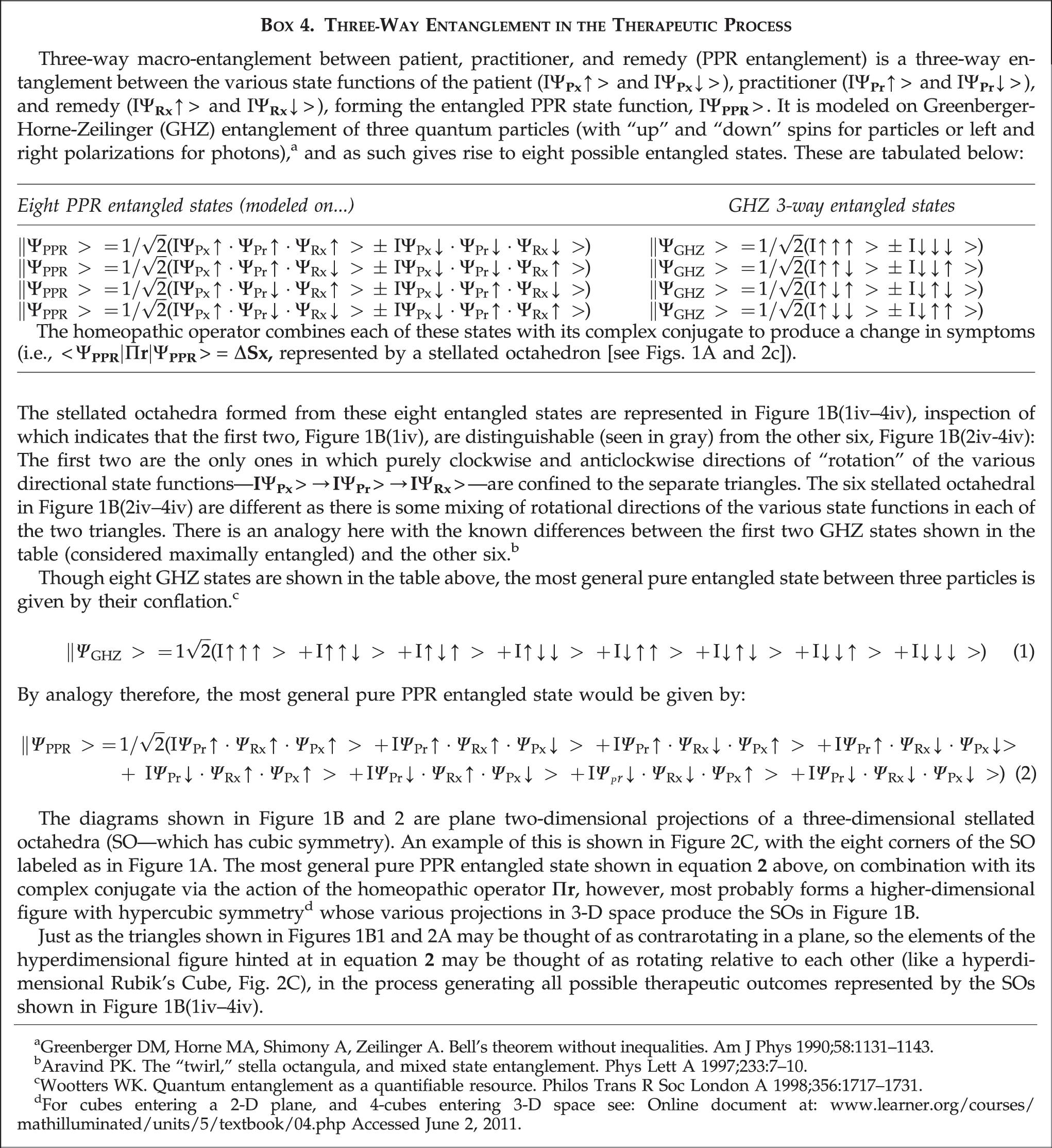
The discourse of quantum theory has been used to describe (1) the homeopathic therapeutic process (in terms of three-way macro-entanglement between patient, practitioner, and remedy, called PPR entanglement), and (2) the homeopathic concept of the Vital Force.
Methods:
Combining these two approaches leads to a semiotic (i.e., pertaining to the theory of sign systems in language) geometry that illustrates the nature of this entanglement and how it could facilitate the patient's journey to cure. Here, this geometry is extended further to gain insight into both practitioner and patient perspectives of the process.
Results:
From the practitioner's perspective, the semiotic geometry predicts PPR entanglement, generating a number of distinguishable therapeutic outcomes that depend on the various patient-, disease-, and remedy-based “contributions” to the overall symptom picture of the remedy arrived at holistically. Furthermore, these outcomes may be seen as different facets of a more generalized PPR entangled state whose semiotic geometrical representation is hyperdimensional. Likewise, the patient's perspective of the journey to cure can also be represented semiotically, this time as a series of cross-sections through a hyperdimensional figure of similar symmetry, entering and leaving the patient's notional “dis-ease” space.
Conclusions:
The semiotic geometries representing practitioner and patient experiences of the therapeutic process ultimately converge. Where they differ is that in elaborating the patient's journey to cure, the practitioner's perspective may be seen as from the outside of a whole process. As it is the patient who ultimately is traveling this journey, the patient's perspective is necessarily from the inside, of stages or cross-sections of the whole process.
Introduction
Scientism* is now considered a cultural curiosity in philosophical circles, 22 –24 yet it thrives in biomedicine, 25 even though there has been trenchant criticism 26 of certain scientistic beliefs (e.g., that purely science-based trials are the only acceptable form of evidence for a drug/procedure's efficacy). Crucially, scientism also dominates the health media discourse, 27,28 resulting in a dogmatic intolerance 29,30 of anything considered “unscientific” (e.g., homeopathy and complementary and alternative medicine [CAM]), that borders on fundamentalism. Consequently, regardless of whatever discourse is used to illustrate the nature of the therapeutic process, 1,2 homeopathy/CAM might be said to have an “explanation problem.”
In the orthodox interpretation of quantum theory, 31 a quantum state's mathematical formulation (Boxes 2 and 3) describes its objective physical reality and is thought to apply only to the incredibly small. Such an interpretation of quantum theory is said to be grounded in an exclusively “realist” or “strongly objective” ontology (i.e., the universe exists separate from us, regardless of whether we observe it or not). Zeilinger, however, has effectively challenged this view, considering the mathematical formulation of a quantum state to be only a representation of what can be known about it.* 32 This implies that an equally valid way of interpreting quantum theory is in terms of information, 33 which can have a more fundamental meaning than any notion of “objective reality.” D'Espagnet goes further, suggesting our reality is only weakly objective, not strongly objective as assumed by most scientists. 34 The implications for our conception of the universe are profound, for what constitutes information—meaning—is to some extent in the mind of the beholder; a beholder being required for it to be considered meaningful in the first place.
The pre-Socratic Greek philosopher Protagoras pre-empted this partly solipsistic conception of the universe with, “Man is the measure of all things.” 35 Since Protagoras, however, philosophers have tended to “banish” meaning outside and independent of human thought, not as modern interpreters of Protagoras have argued, fundamentally and dynamically grounded in human nature. Thus, Professor Mark Turner has argued that, “Meaning is conceived of…as essentially anchored in states of affairs in an objective reality, with the consequence that the meaning of an utterance must be the reality to which it refers…a semantic express train shoots straight from the linguistic symbols to an objective reality without passing through the human brain, let alone stopping in the human brain, let alone taking its entire journey there.” 36 Consequently, Turner argues for an updated, more cognitively aware attitude toward Protagoras, proposing the need for a new theory of meaning that could inform the physical and biosciences.
It is in this context that Zeilinger's interpretation of quantum theory 32 might prove useful. If a wave function contains within it all that can be known about a system by observation (not its presumed ontological [i.e., pertaining to the philosophical study of the nature of being and existence] reality outside of and separate from an observer), 37 then as Henry Stapp pointed out, the act of observation in part creates that which is observed 38 (or, as 18th-century Bishop George Berkeley put it, “To exist is to be perceived”). 39 It is this realization of an effectively nonlocal coherence between observer and observed, which is how the therapeutic process in any healing modality (including homeopathy) might usefully be described, using the discourse of quantum theory. 1
For example, consider “entanglement” between such qualitatively and apparently ontologically different “macroscopic” entities as a remedy (something derived from a material substance) and a symptom totality (an abstract idea generalized from one individual's observations about another). 40 From the standpoint of a realist ontology, such “entanglement” would appear unrealistic and indeed has been contemptuously dismissed. 31 However, if it is realized that remedy and symptom totality are before anything else sources of information 41 and thus have similar ontologies, then they are quite capable of becoming “entangled” (via the practitioner) during the therapeutic process. 42
Orthodox quantum theory is one of the most successful, pragmatic theories ever devised. Adopting an information-based interpretation of quantum theory allows generalization of its discourse beyond exclusive concentration on the physics of matter, to the therapeutic contexts described here. Indeed, via Weak Quantum Theory, such generalization has already been shown to be relevant to the description and understanding of such nonphysical phenomena as the dynamics of interpersonal relations (Box 1 and Box 2). 43

In addition, two recent trials (one indicating clinical benefits in rheumatoid arthritis solely from the homeopathic consultation and not homeopathic remedies, 44 and the other showing that placebos have meaningful clinical benefits in irritable bowel syndrome even when the patient knows they are receiving placebo 45 ) may be understood in terms of a previously described 46 complementary relationship between remedy and consultation, 47 similar to that found between momentum and position, or energy and time, in orthodox quantum theory.
Thus, the discourse of quantum theory could lead to conclusions about the therapeutic process akin to those of current holistic worldviews, and more ancient vitalistic traditions, 48,49 no doubt provoking negative responses from those who believe anything pertaining to vitalism is an anachronism.
Representation of the Therapeutic Process as Topology
Semiotics is the study of signs and symbols, a sign being anything as long as it is interpreted as a sign (i.e., it signifies something). Without signification (by someone), a sign of itself has no intrinsic meaning. From this perspective, it is the meaningful use of signs that concerns semiotics. 50 In this respect, this article represents the culmination of a project to develop a semiotic “geometry” to describe the therapeutic process.
In previous articles, two quantum metaphor/models of the therapeutic process were elaborated. These described the following: 1. the Vital Force (or Vf—a venerable concept used by most forms of CAM, including homeopathy) in terms of the wave function for a spinning quantized gyroscope,
51
and 2. the relationship between patient, practitioner, and remedy as a nonorthodox quantum-type three-way entanglement—called PPR entanglement—between patient, practitioner, and remedy.
1
It was possible to combine these two representations, 2 so that the Vf gyroscopic wave function could be “normalized,” allowing different stages of the curative homeopathic process to be elucidated. Particularly, a semiotically derived geometrical description of the “therapeutic state space” was identified, allowing a topology for the patient's journey to cure to be glimpsed.
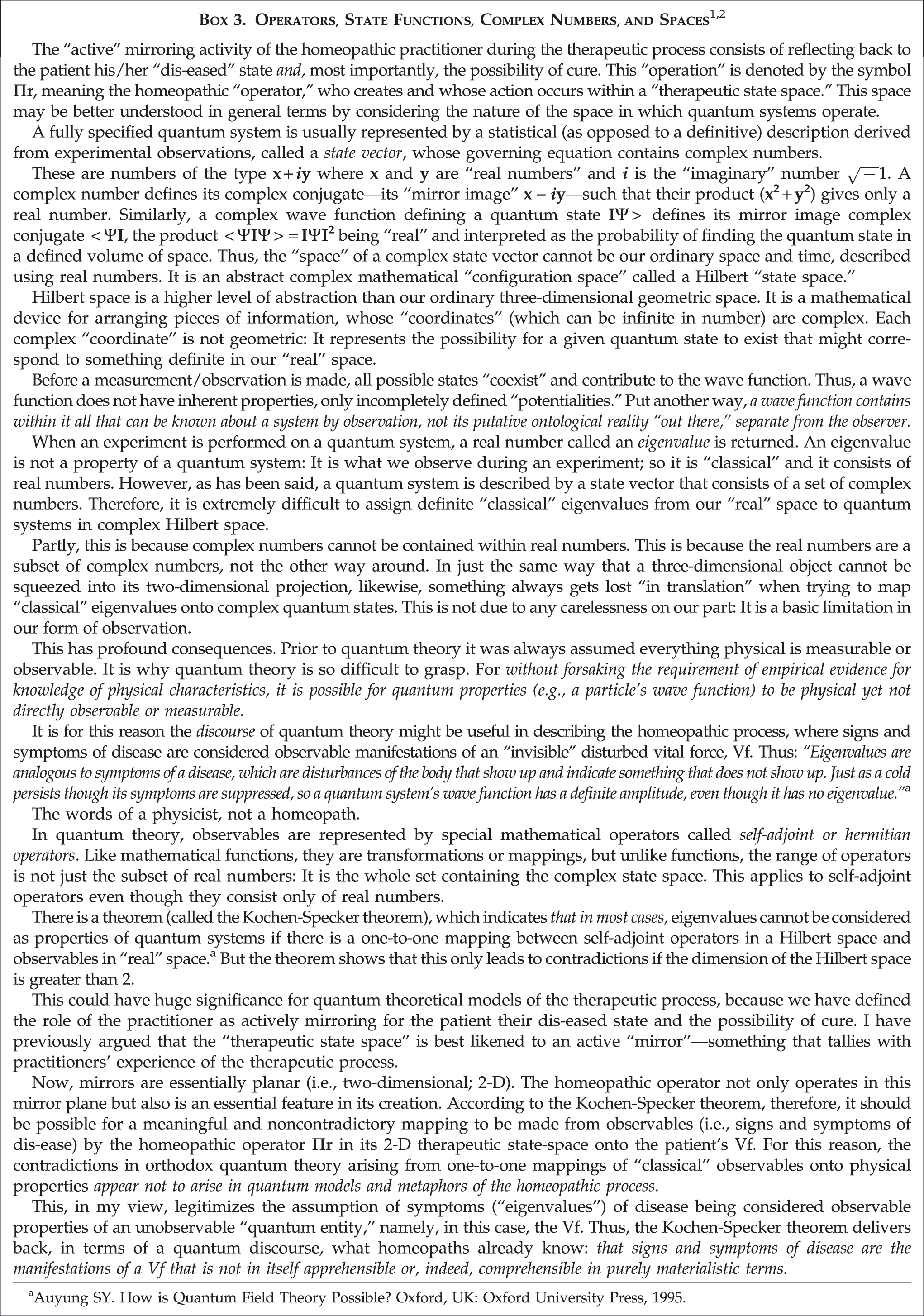
Thus, during the consultation, the practitioner provides the conditions necessary for an active “mirror-like” (i.e., two dimensional) “therapeutic state space” to arise in which the patient's dis-eased state—represented as a chiral tetrahedron 1 —is not only reflected, but also “inverted.” In terms of this semiotic geometry, the possibility of cure is represented as the inverted mirror image chiral tetrahedron (Boxes 1 and 2).
By “inverting” that which is reflected in it (i.e., not simply passively reflecting back the patient's unwell state, but actively demonstrating to the patient what a cured state might be), the therapeutic mirror plane may also be considered to exhibit the topological features of a Möbius strip. 52 The initially elaborated patient dis-eased state, by active reflection, may be thought of as taking one “turn” around the therapeutic state space's “Möbius strip,” 2 becoming inverted in the process into the practitioner's reflection of the cured state. Recognizing this in effect “chirality,” the patient's “journey to cure” is represented metaphorically as a movement “through the looking glass” of the mirrorlike therapeutic state space, in effect combining the reflected dis-eased and cured states into a stellated octahedron representing the curative PPR entangled state. 1
In this respect, the practitioner might also be considered to be acting as an “impulse” 53 on the patient's Vf wave function, temporarily increasing its “amplitude” so that the movement “through the looking glass” can be achieved. But the practitioner is also included in PPR entanglement, not least by “witnessing” the therapeutic process. Underpinning this is the very nature of the homeopathic consultation which because of its length, depth, and subtlety 44 effectively isolates the patient and practitioner from the outside world: conditions, it turns out, that are ideal for their coherence.†
By so providing the ground for entanglement, the practitioner-derived mirrorlike therapeutic state space that arises reflects in both directions. Consequently, it is possible to consider the patient as an “impulse” acting on the practitioner's Vf wave function, and to perform on it a series of normalization operations (similar to those on the patient's Vf) to see how it too fluctuates through the therapeutic process. 2 Thus, there is a coherent interplay between patient and practitioner that can be rather aptly represented by M.C. Escher's etching of “Drawing Hands.” 54,55
It seems possible, therefore, to render a visualization of the homeopathic therapeutic encounter in terms of a semiotic topology on which the various stages of the therapeutic process can be represented as a changing pattern of geometric shapes. These shapes are themselves derived from a semiotic representation of the dynamic relationship between the patient, the practitioner, and the remedy, which can be understood as becoming “entangled” during the therapeutic encounter.
As such, therefore, the therapeutic encounter may be amenable to the general discourse of quantum theory (which is not to say that the basis of homeopathy is orthodox quantum physics, or that the various geometric shapes discussed and the space(s) in which they exist conform to real physical shapes or dimensions). This article, therefore, describes further work into the nature of these semiotic relationships: in particular, how they might be perceived from the different perspectives of the patient and the practitioner.
Practitioner and Patient Viewpoints: A Matter of Perspective
The Practitioner's Perspective
As has been developed in previous articles published here and elsewhere, 1,46,47,51 the homeopathic consultation results initially in the practitioner showing the patient their dis-eased state, represented semiotically as a chiral tetrahedron at whose “epicenter” is the patient (Fig. 1A), itself derived from consideration of the patient, practitioner, and remedy as a tripartite relationship (Box 3). 1
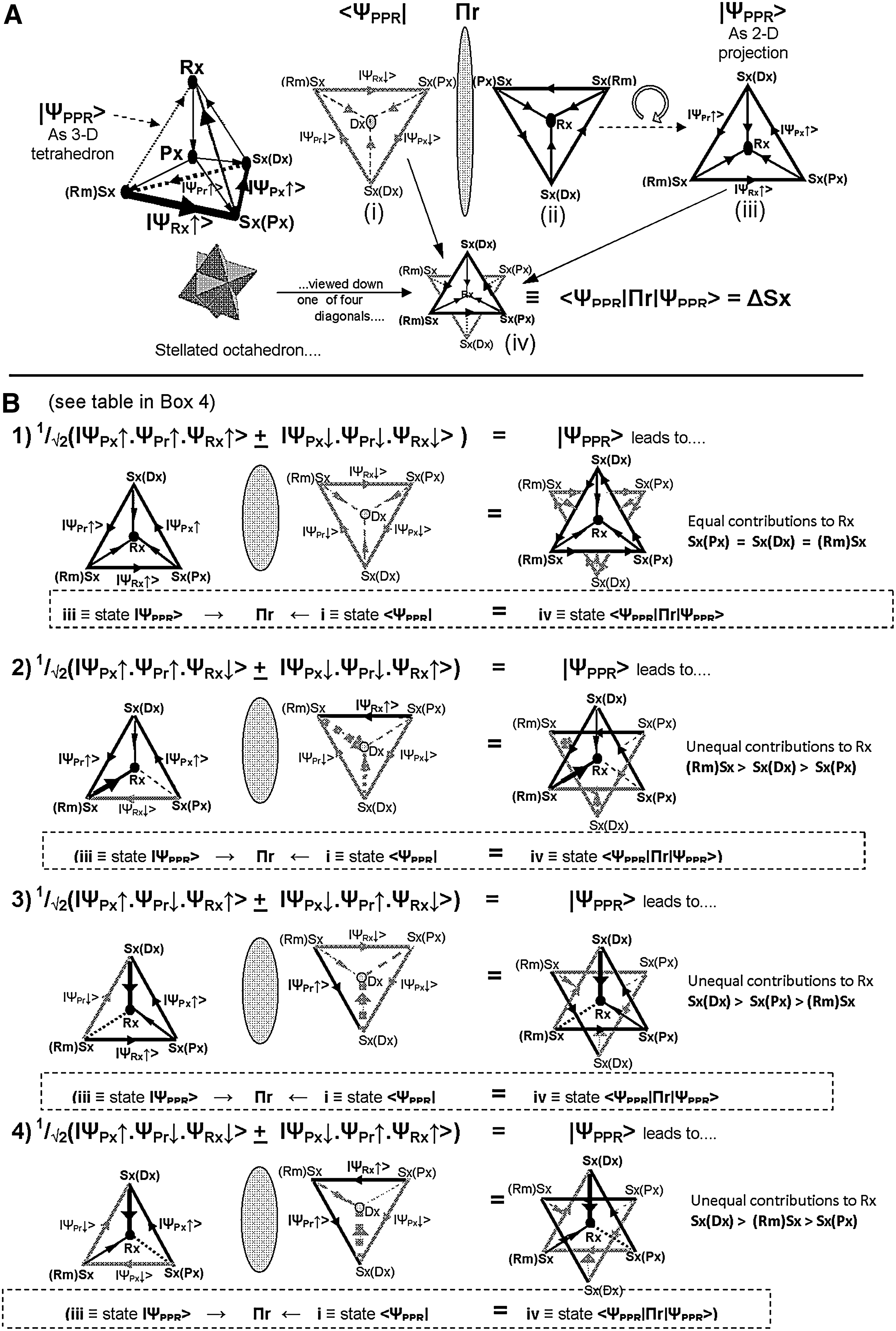
Précising the conclusions of the previous article, 1 the possibility of cure is then represented as the inverted mirror image of the semiotic tetrahedron, topologically equivalent to the mirrored state going once around the Möbius strip-like “therapeutic state-space,” becoming inverted in the process. 1 Positioned at the epicenters of both semiotic tetrahedra, the patient begins their notional “journey” to cure by stepping “through the looking glass” of the two-dimensional mirrorlike “therapeutic state space” (Box 3), effectively combining the initial and possible final states (i.e., “fusing” the two semiotic tetrahedra) into a “ curative” stellated octahedron.‡ 1
For ease of visualization, Figure 1A shows the plane projections of these three-dimensional figures (e.g., a tetrahedron projected through one of its corners reduces to an equilateral triangle, while similarly projecting a stellated octahedron gives a Star of David or hexagram). The base triangle of the semiotic tetrahedron (projected through its
In addition in Figure 1A, there is a sequence of noncommuting therapeutic “operations,”
56
which may be considered as directional state functions (Boxes 1, 2, and 3) represented by the sides of the semiotic tetrahedron's base triangle. These state functions are: • the patient's experience of symptoms, state • which are observed and considered by the practitioner, state • who on the basis of observations, knowledge, and experience, prescribes a remedy, state • whose effect on the patient state
However, there are a variety of possible therapeutic outcomes depending on the nature of the various state functions which, for simplicity, have been reduced to two for each state. Thus: • the patient state function, • the practitioner state function, • the remedy state function,
providing a rotational “directionality” to the therapeutic sequence, which in terms of the semiotic tetrahedron's base triangle goes
etc.…←
This now gives rise to two semiotic triangles—the second being a mirrored inverted version of the first (the gray triangle in Fig. 1A), which when superimposed, results in the Star of David configuration shown in Figure 1A and 1B1—and a contrarotating directionality to the therapeutic sequence, i.e.:
Referring to Figure 1A, the patient's initial dis-eased state (given by the inverted gray triangle—
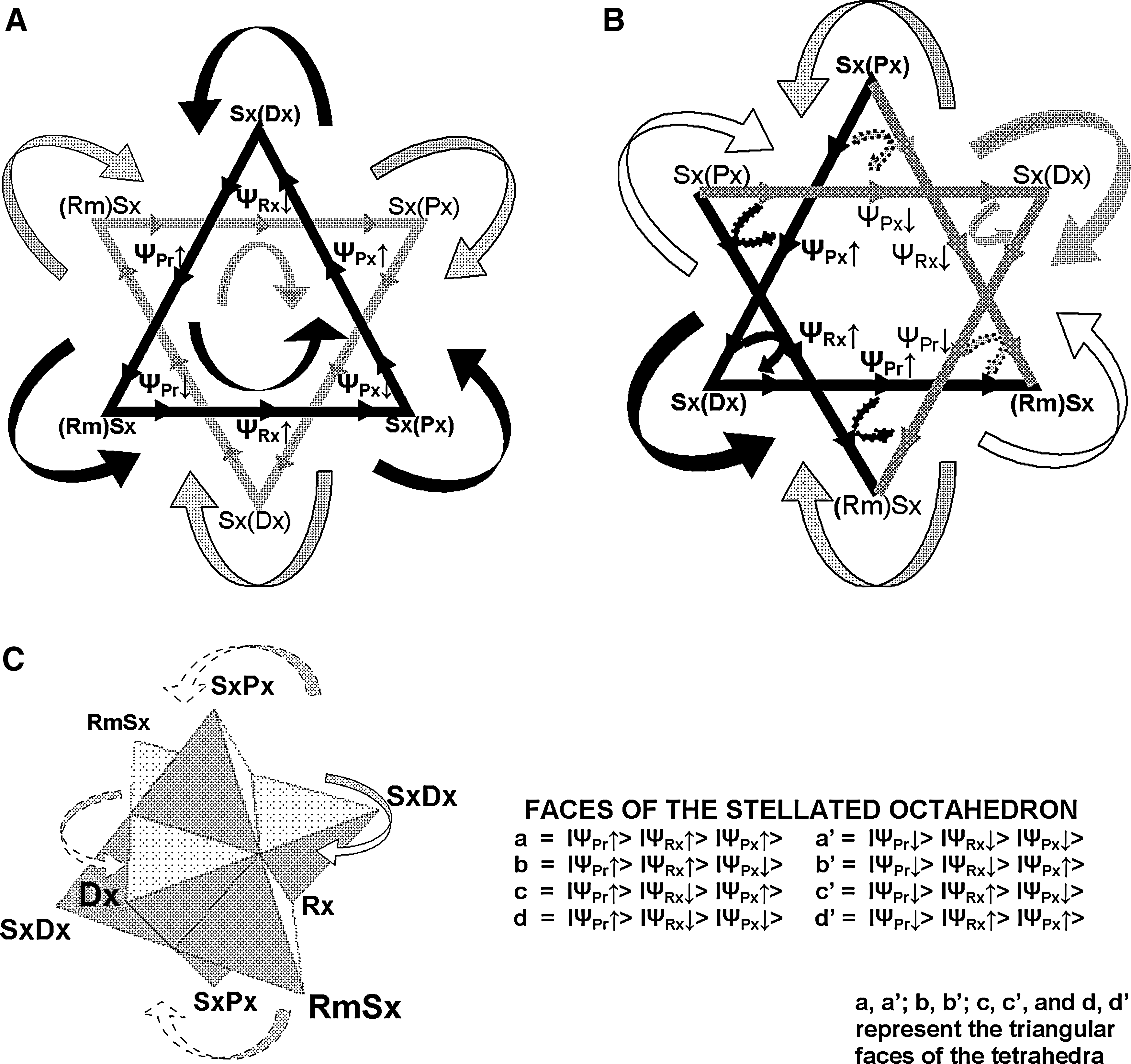
Inspection of the hexagram shown in Figure 1B1iv (and magnified in Fig. 2A) reveals an interesting relationship between the contrarotational directions of the black and gray (inverted) larger triangles. The overlap of the two larger triangles can be seen to generate six smaller triangles with their own rotational directions (see curved arrows around each corner of the hexagram). These not only “mesh” together as if they were a set of interlocking cogwheels, but they also harmonize with the overall contrarotating directions of the large triangles (see curved arrows inside them).
The significance of this is indicated by inspection of the other hexagrams shown in Figures 1B(2iv–4iv), for example Figure 1B2iv (also magnified in Figure 2B). Now opposing rotational directions are mixed into the two larger triangles. This is mirrored in the six smaller triangles of the hexagram. Though their overall inner rotational directions again mesh with each other (the curved arrows around each corner of the hexagram), they now also contain an opposing rotation to the smaller and larger triangles (the small arrows inside the smaller triangles): indeed, this small opposite rotation could be said to constitute a kind of internal “friction”—or “brake”—on the larger rotations. Similar patterns of internal “friction” on the rotations of the larger triangles exist for the other hexagrams shown in Figures 1B3iv–4iv. Thus, because they have no internal “friction,” the two states shown in 1B1iv and Figure 2A are distinct from the other six states 1B2iv-4iv, which do have internal “friction” (Box 4).
What the term “friction” could mean in this context can probably be best understood as the relative balance of factors that determine how the practitioner arrives at a remedy solution. Thus, the eight combinations of state vectors shown in Figures 1B1(iii & iv)–1B4(iii & iv) (which affect the overall directionality of the “rotation’ in each of the semiotic tetrahedral base triangles) could be said to lead to ways of predicting various possible “contributions” to the remedy Rx arrived at, based on practitioner-based observations of patient symptoms (Sx[Px]), experience of disease symptoms (Sx[Dx]), and knowledge of remedial substance symptoms ([Rm]Sx) (Box 1).
So, Figures 1B1iii/iv and 2A represent the result of equal contributions (i.e., no “friction”) from practitioner-based observations, experience, and knowledge of these three symptom groups. However, it is also possible for there to be unequal contributions (i.e., “friction), resulting in Figures 1B2iii/iv–4iii/iv and 2B. Here, practitioner-based observations, experience, and knowledge of, respectively, (Rm)Sx (1B2iii and 2B) and Sx(Dx) (1B3iii and 4iii), make the dominant contribution to selection of the remedy Rx.
Recall that the diagrams shown in Figures 1B and 2 are plane projections of higher-dimensional (three-dimensional) stellated octahedra (SO), an example of which is shown in Figure 2C, with the eight corners of the SO labeled as in Figure 1A. Also, SOs are cubically symmetric, which means they can be inscribed within a cube. The most general pure entangled state shown in equation
Just as the triangles shown in Figures 1B1 and 2A may be thought of as contrarotating in a plane, so the various elements of the hyperdimensional figure hinted at in equation
Finally, to sum up this section: elaborating a semiotic geometry for the therapeutic process, from the practitioner's perspective, may be seen to employ an increasing number of dimensions from: 1. The two dimensions of the mirrorlike therapeutic “state space” and the basic triangular entangled relationship of the patient, practitioner, and remedy; 2. To the three dimensions of the tetrahedral dis-eased and stellated octahedral states and the patient's notional “journey to cure” through the therapeutic state-space; 3. To finally, the hyper-dimensional general patient–practitioner–remedy entangled state.
The patient perspective
Multidimensional geometry can also be employed to illustrate the patient's perspective of the therapeutic process (Fig. 3). Here, one assumes a patient's dis-eased state is, in the most general sense, necessarily limiting and that cure of that state implies that the role of the practitioner is to in some way assist the patient in removing or becoming free from that limitation. One then imagines that the patient in their diseased state is confined (“stuck”) within a “space” of limited (and limiting) dimensions; the practitioner's role in cure may then be thought of as helping to free the patient from the confines of a lower-dimensional “dis-ease space” so the patient can occupy a higher-dimensional “healthy space.”
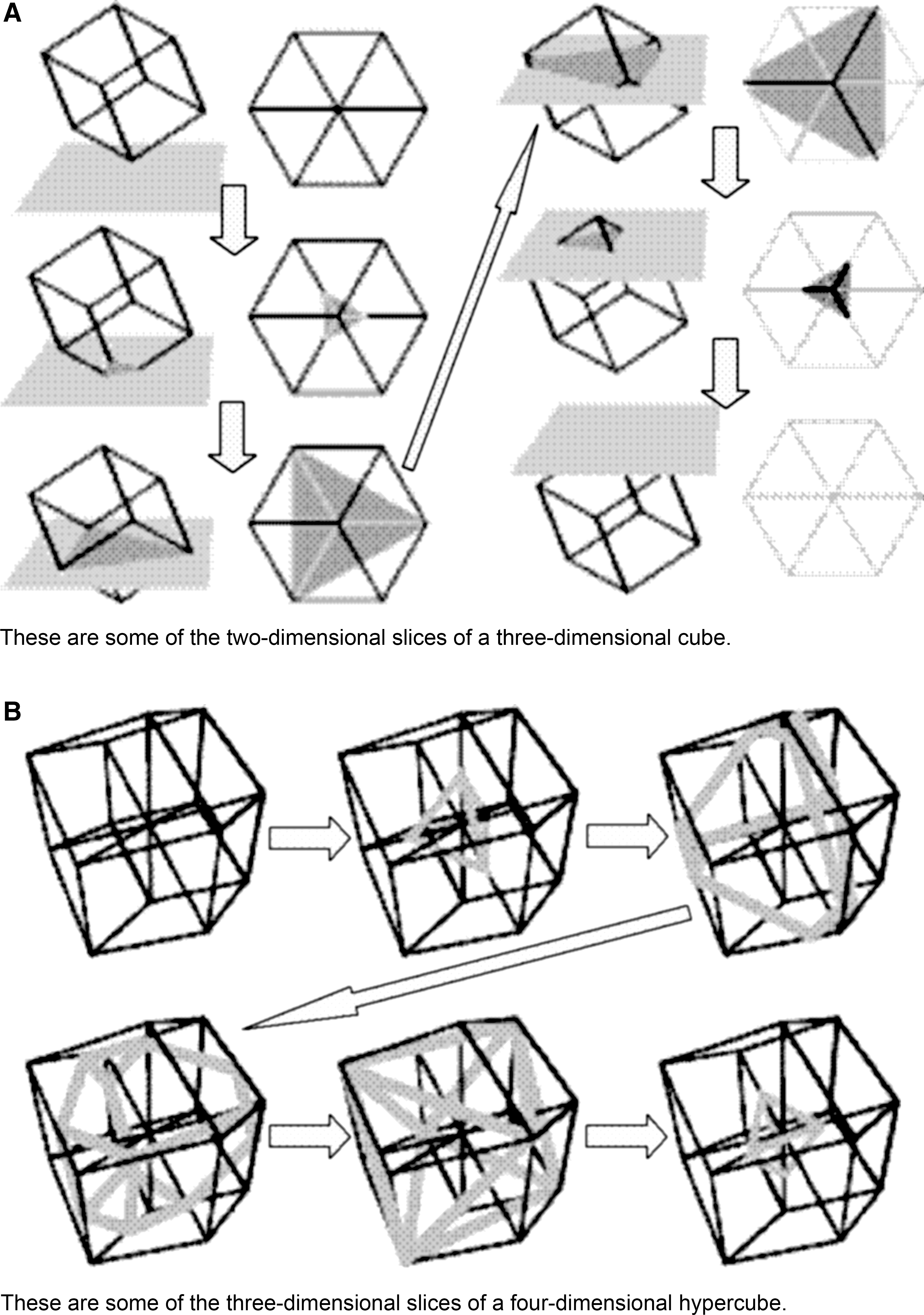
This is relatively easy to represent geometrically. A simple example is to imagine how a three-dimensional cube might appear to hypothetical beings living in a two-dimensional universe if the cube were to enter their two-dimensional “space” corner-first 57 (see Fig. 3A—such hypothetical two-dimensional beings were satirized in the late 19th century by E.A. Abbott in his novel, “Flatland: A Romance of Many Dimensions”). 58
Thus, on entering the two-dimensional universe, its occupants observe not a cube but a series of fluctuating polygons, beginning with an equilateral triangle that gradually grows in size as the cube penetrates corner-first further into the plane. After the cube has passed a third of the way through, the equilateral triangle begins to truncate (i.e., lose its corners) until half way through, a hexagon is formed. Further passage of the cube through the plane reverses and inverts the previous sequence of shapes, so that the hexagon deforms back through a truncated triangle, then an equilateral triangle (inverted compared to the triangle formed when the cube first entered the two-dimensional space) that diminishes in size until, as the cube leaves the two-dimensional plane, it vanishes as “magically” (as far as the two-dimensional beings are concerned) as it appeared.
Going up a dimension, a similar series of operations can be envisaged for the appearance in three-dimensional space of a four-dimensional hypercube along one of its diagonals (Fig. 3B). 57 Here, it is the sections of the hypercube that are observed as fluctuating polyhedra. Thus, as the hypercube enters and travels through three-dimensional space, a gradually growing tetrahedron is observed. The tetrahedron then becomes truncated as the hypercube penetrates further into the three-dimensional space, before turning into an octahedron. The sequence of polyhedra is then reversed and inverted, finally forming an inverted tetrahedron that diminishes in size and disappears as the hypercube leaves the three-dimensional space.
From the patient's perspective of the therapeutic process, the significance of this series of operations is that, like the practitioner's perspective, it too generates a pair of semiotic tetrahedra, one inverted compared to the other, but now near the beginning and near the end of the four-dimensional hypercube's journey through three-dimensional space. In this respect, the effect of the therapeutic process on the patient can be likened to and illustrated by the passage of the practitioner's four-dimensional “hypercube” through the patient's three-dimensional “space.” This results in the patient being first “shown” their dis-eased state (the first tetrahedron), followed by the possibility of cure (the second inverted tetrahedron), while “setting up” the patient for their “journey to cure” from the dis-eased to the cured state. From the practitioner's perspective, this is the patient going “through the looking-glass” of the therapeutic state space, in effect combining the reflected dis-eased and cured (tetrahedral) states into a stellated octahedron representing the curative PPR entangled state. (Fig. 1A).
This convergence of the practitioner and patient perspectives may be generalized as, Humans are those beings who by their conscious, intentional efforts can ensure the enlivening and fructification of “lower dimensional” states (i.e., those with fewer possibilities) by interfacing with states of higher dimensionality (i.e., those with greater possibilities). No more so is this most likely to be true than in the therapeutic process.
Conclusions
As previously stated, semiotics is the study of signs and symbols, with a sign being anything as long as it is interpreted as a sign (i.e., it signifies something). Without signification (by someone), a sign of itself has no intrinsic meaning. From this perspective, it is the meaningful use of signs that concerns semiotics. 50 In this respect, this article represents the culmination of a project to develop a semiotic “geometry” to describe the therapeutic process.
Walach was probably the first to specifically apply modern semiotics 59,60 to the homeopathic therapeutic process. Instead of considering the supposed local, causal effects of a potentized homeopathic remedy (i.e., its pharmacologic activity, regardless of the presence or absence of molecules of the substance), he adopted the semiotic notion that the homeopathic remedy is a “sign” working simultaneously in and for two different but connected meaningful contexts. Each of these contexts was represented geometrically in two dimensions as a semiotic triangle. 40
These are (1) the symptoms of a sick person signifying a disease state (first meaningful context), and (2) a homeopathic remedy in the materia medica (second meaningful context), connected by the Law of Similars. Walach 42 then demonstrated how semiotics illustrates homeopathy as two instances of generalized entanglement: one between the potentized remedy (Rx) and the original unpotentized remedial substance (Rm); the other between the individual symptoms of a patient (Sx[Px]) and the symptoms of the substance produced during homeopathic proving (Sx[Rm]). This double entanglement approach is said to generate testable predictions, and is thought to be analogous to the cryptographic and teleportation applications of orthodox quantum entanglement. 42
PPR entanglement is a more general approach to the therapeutic process. Adding a third semiotic triad explicitly representing the practitioner (who in Walach's model is only implied, creating entanglement via application of the Law of Similars), 40 PPR entanglement considers the patient (Px), practitioner (Pr), and remedy or therapeutic modality (Rx) coming together in a potentially therapeutic macro-entangled state, the geometrical representation of which (compared to Walach's model) can be “folded” into a third dimension. 61 By using purely discursively the formalism of three-way quantum entanglement (see Box 4), this may be represented by a state function IΨPPR>(as are the states of each of the patient, IΨPx>; the practitioner, IΨPr>; and the remedy/therapeutic modality, IΨRx>, Box 1) existing in a practitioner-elaborated, active mirrorlike “therapeutic state space.”
However, it is not yet possible to relate these state functions to quantifiable physical observables, as in orthodox quantum theory (e.g., position and momentum). These state functions represent more qualitative observables, such as the signs and symptoms of a dis-ease, as expressed by the patient and observed by the practitioner. Though a more detailed mathematical proof is needed to flesh out the meaning of state functions and hypothetical spaces used in this semiotic context (Box 3), a topological representation of PPR macro-entanglement as presented here leads to a more generalized (if less quantitative) quantum-type description of the therapeutic process, with possible applications to other healing modalities.
Although not constituting direct experimental evidence of PPR entanglement (and such as there is, is still controversial), 62 –65 it could be argued that inklings of confirmation of the PPR entanglement hypothesis are beginning to appear. Consider, for example, the trial mentioned earlier, in which clinical benefits were indicated in rheumatoid arthritis solely from the homeopathic consultation and not any homeopathic remedy. 44 Though it was too underpowered to draw such a conclusion, far from being evidence against the effectiveness of homeopathic remedies, this trial might actually be hinting at something far more profound: a form of complementarity between remedy and consultation (similar to that between momentum and position or energy and time in orthodox quantum theory), that is imposed as a direct result of the intrinsic reductionist rationale of the randomized controlled trial (RCT). 47
Thus, conventional RCTs, with their emphasis on the effect of the medicine/drug, might necessarily lose sight of the consultation. On the other hand, RCTs that attempt to isolate the effect of the consultation (as in the trial mentioned above) would necessarily lose sight of the medicine. For by analogy with orthodox quantum theory, the RCT rationale with its emphasis on blinding, would only allow knowledge of the medicine or the consultation as parts of a complementary pair of phenomena making up a whole, but not both with equal certainty at the same time. 47,66 Inspired by the results of an earlier study of homeopathic RCT data, 67 it is interesting that such a conclusion had been earlier predicted, 46 based on the PPR entanglement hypothesis.
It took around 50 years for Schrödinger's 68,69 original suggestion of the conditions for entanglement in orthodox quantum theory to be verified experimentally by Aspect and Dalibard. 70 One can only hope such experimental verification of entanglement in the therapeutic process will not take so long.
In the meantime, the semiotic geometries developed here representing practitioner and patient perspectives of the therapeutic process may be seen ultimately to be convergent. Where they differ is that in elaborating the patient's journey to cure, the practitioner's perspective ultimately is from the outside looking in at a potential whole process. But it is the patient who is taking their journey to cure, so the patient's perspective is necessarily from the inside looking out, at perceived stages or cross sections through a whole process, developing through time.
Footnotes
Acknowledgments
The author wishes to gratefully acknowledge fundamental insights provided by Professor Lucius S. Diamond, without whom this work would have not been possible.
Disclosure Statement
No financial conflicts exist.
*
Scientism is the unsubstantiated belief that (1) only scientific knowledge is real knowledge; (2) there is no rational, objective form of inquiry that is not a branch of science; and (3) science is the absolute and only justifiable access to truth.
*
Indeed, mathematics might have an even more fundamental role in science than mere representation; see for example, Rowlands P. Zero to Infinity:The Foundations of Physics (Series on Knots and Everything,vol. 41; series ed. Kauffman LK). Singapore: World Scientific Publishing, 2007.
†
The conditions for coherence between the entities of a system in orthodox quantum theory are known to involve their isolation from the rest of the universe. See Hameroff SR, Penrose R. Orchestrated reduction of quantum coherence in brain microtubules: A model for consciousness. In: Hameroff SR, Kaszniak A, Scott AC, eds. Toward a Science of Consciousness: The First Tucson Discussions and Debates. Cambridge, MA: MIT Press, 1996:507–540. Also, Gernert D. Conditions for entanglement. Front Perspect 2005;14:8–13.
‡
It should be made clear that the shapes shown in Figures 1 and ![]() are geometrical representations of the various ‘state functions’ alluded to in the text and an alternative way of representing the results.
are geometrical representations of the various ‘state functions’ alluded to in the text and an alternative way of representing the results.