
Abstract
Background:
In May 2006, a multidisciplinary community-based integrative medicine (IM) clinic was established in Sydney, Australia. It was designed to offer a wide range of IM services, for primary care and to serve as a referral center.
Objective:
The aim of this study was to determine which factors were successful and which ones posed challenges for establishing this kind of clinic.
Method:
A study of the first 4 years of this primary care integrative medicine clinic was undertaken, using mixed methods—both qualitative and quantitative.
Results:
Consistent with success factors identified in the literature, the clinic had an open-minded culture, credible supporters, suitable facilities, and clinically competent practitioners. Throughout the 4 years of its existence, the clinic strove to create an economically sustainable environment and to develop the service. As time progressed, it became evident that at least half of the practitioners needed to be biomedical doctors for the practice to remain viable. The challenges encountered were creating an economically sustainable clinic, managing high staff and practitioner turnover, finding the right balance between practitioners and services offered, developing an integrative medicine team, and building research capacity to evaluate the clinic and patient outcomes.
Conclusions:
Although many integrative medicine clinics fail to survive the first few years, after 4 years, this multidisciplinary primary care clinic had succeeded in establishing a viable health care service offering both integrative medicine and conventional, traditional, complementary, and alternative medicine. Finding the right mix of staff members and following up with evaluations to track progress are important.
Introduction
Services offering orthodox biomedicine, and traditional, complementary and alternative medicine (TCAM) provided by 1 or more practitioners are often referred to as integrative medicine (IM) clinics. The definition of IM is evolving, and, for many providers and consumers it has supplanted such terms as holistic, natural, complementary, and alternative medicine. 1,2 In this article an IM clinic refers to any clinic that offers both conventional biomedicine and TCAM services.
Two kinds of locations for IM clinics are reported in the literature: the hospital and the primary care setting. IM clinics have adopted service models ranging from those simply housing health care practitioners from different paradigms, through to clinics offering multidisciplinary, integrated, patient-centered care. 2 –6 Few IM clinics have been described in the literature and little is known about the Australian setting. 3,7
Many IM clinics fail to survive beyond the first few years of operation. 8 Evaluations of IM clinics have found similar prerequisites for survival beyond inception funding. These were: an open-minded culture; credible supporters; high competency of practitioners, with the right fit of practitioners and staff; effective communication and trust; suitable physical facilities; an economically sustainable environment; and resources for service development and evaluation. 3,9 –12
Specific to IM primary care clinics, a review of four clinics in the United States, found that, although the practices varied in their philosophies, therapies, and practitioner skills, there were common characteristics that contributed to their success. All four practices had created business models that enabled extended consultation time. Most of the biomedical doctors were already trained in TCAM therapies before joining the practice and, if not, they developed an interest in TCAM quickly and began integrating such therapies into their work. As well as offering primary care services, some of the practices also had a specialized consultative role. 13
Methods
This study was conducted to describe the 4 four years of a primary care IM clinic and to examine the factors contributing to its success and what challenges were posed.
Debate continues about appropriate methodology for evaluating complex healthcare such as IM 14,15 and the applicability of mixed methods for this purpose. 16 Similar to a proposed evaluation model by Walter et al., 17 the current investigators returned to Donabedian's model—structure, process, and outcomes 18 —as the basis for evaluation.
The methods for data collection proposed by Walter et al. 17 included both qualitative and quantitative approaches drawing on a wide range of disciplines, and were similar to other mixed-method approaches, including rapid-assessment procedures. 19 Based on this, both qualitative and quantitative data from the first 4 years of the clinic were collated and analyzed. Qualitative data were obtained by reviewing the minutes of staff meetings, checking written responses from a staff questionnaire, and incorporating 2 of the current authors' personal knowledge of the clinic's history regarding dates, staffing, services offered, and confidential information, such as the clinic's finances. Quantitative data were obtained from a staff questionnaire, a patient-satisfaction questionnaire, and analysis of data routinely collected for administration and clinical records.
Based on the literature, a staff questionnaire was developed and distributed shortly after the clinic's third anniversary. All practitioners, the medical director, and 1 nonclinical director responded on the written questionnaire anonymously. The aim was to document their opinions, especially the less-vocal ones. The questionnaire consisted of 27 questions, beginning with an exploratory broad open-ended question about top three issues, followed by 25 statements, with a 5-point response option and prompts for comments. The statements were designed as “questions” about the provision of patient-centered care, 9 the IM team, and the success factors for an IM clinic identified from the literature. The results of the questionnaire responses were presented and discussed in a staff meeting shortly after.
As part of quality-assurance requirements for registration as a general practice (GP) clinic, an ad-hoc survey of 93 patients who had seen a GP was undertaken. This questionnaire had been recommended by the registration body. The questionnaire had 16 statements with a 5-point response option from “very unsatisfied” to “very satisfied” that were designed to measure patient satisfaction with the services provided by the clinic. There was no evidence that the questionnaire was a tested, standardized tool, but this questionnaire was readily available and locally acceptable.
Qualitative data were manually coded on paper from which categories and themes were identified using iterative and recursive processes. 20 The practitioner questionnaire was an important data source. As well as addressing the topics identified in the literature, the open-ended questions and discussion about the results at a staff meeting generated new themes. As part of this process, the qualitative analysis drew on the quantitative data to provide further contextual information. Quantitative data were analyzed using descriptive statistics.
Results
Information was most readily available about the structure, such the building, staff and, apothecaries; and process, such as the business model and the services provided. The only outcome data were obtained from the patient-satisfaction survey.
Description of the clinic
The clinical director's vision (which was often expressed at staff meetings) was to create a center for excellence in the practice of IM. The clinic used the definition of IM written by The Consortium of Academic Health Centres for Integrative Medicine. 21
The business model used by the clinic was common for primary care in Australia. Only the managerial staff members were employed by the clinic. A mix of biomedical doctors, and allied-health and natural therapy practitioners subcontracted their services to the clinic, earning money on a fee-for-service basis, with a proportion paid to the clinic to cover operational costs.
Recruitment of practitioners to the clinic aimed to provide a comprehensive skill mix and to meet perceived patient demand. Table 1 lists the 15 practitioners, who were working in the clinic at the fourth-year anniversary, and shows their skill base. Two (2) biomedical doctors, 1 psychologist, and the 1 shiatsu practitioner were male. All practitioners worked part-time.
Note: Blank spaces indicate No.
Energy medicine includes TOM (Chi), homeopathy, flower essences, and Reiki.
GPs providing conventional primary care services +/− TCAM.
Doctor refers to a biomedical doctor providing specialized environmental and nutritional medicine only.
TOM, Traditional Oriental Medicine; GP, general practitioner.
Aside from a small Chinese herbal apothecary and a small Western herbal apothecary where practitioners mixed individualized formulas, no products were sold directly to patients by the clinic. Instead, patients were given a written prescription to purchase natural therapies from local health food stores and pharmacies.
The majority of patients self-referred to the clinic and could choose to see any practitioner. Often, patients who had complex chronic health problems were unsure about which practitioner to visit first. The receptionists were not trained in medical triage and were instructed in these instances to schedule an initial consultation with a biomedical doctor. Most patients used the clinic as their primary health care practice. A small number of patients, who sometimes were referred by an outside practitioner, used the clinic for specialized IM or TCAM services. The administrative software was not used to record any data about referral patterns.
Most patients paid a fee at the time of the service and claimed a partial refund through their private health insurance or through the government-funded Australian Medicare system. Both public and private health care rebates were small, with out-of-pocket expenses commonly ranging from 50% to 80% of the fees paid by patients. Approximately one sixth (15.8%) of services were billed directly to Australian Medicare or to other insurers with no out-of-pocket cost to the patients. In most cases, this was for services provided by the biomedical doctors.
Notwithstanding the personal expenses to patients, the demand for the services offered by the clinic continued to grow at a steady pace. After 4 years, 6604 patients were registered with the clinic (Fig. 1). Patient demographics were in keeping with population trends for TCAM use in Australia. 22
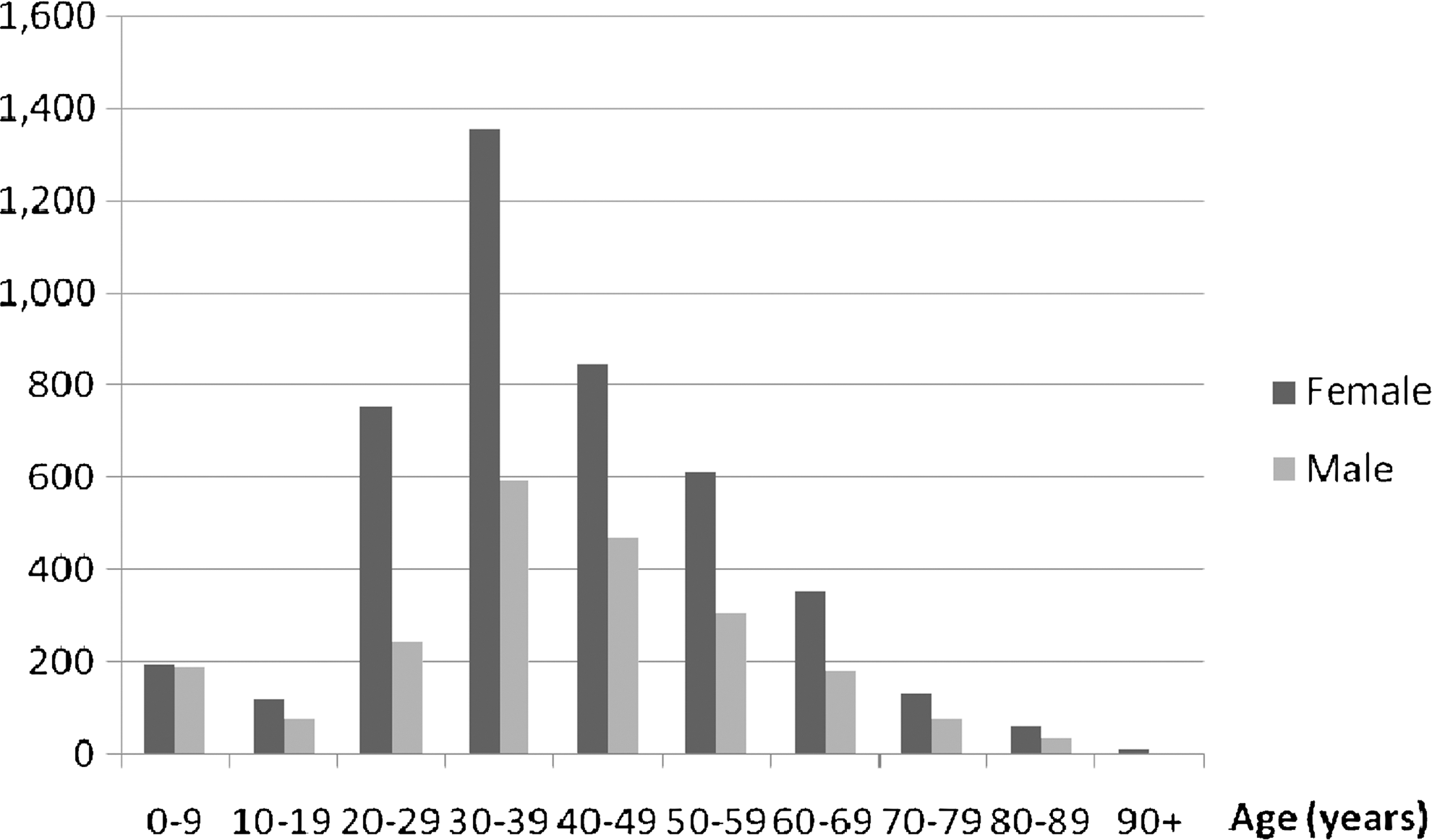
Number of patients registered with the clinic (May 1, 2006 to April 30, 2010).
The clinic opened with a larger proportion of allied-health and TCAM practitioners; however, 4 years later, there was an equal number of biomedical doctors. Biomedical doctors were the main income generators for the clinic; they saw the most patients, billed more per consultation, and had shorter consultations. Biomedical doctors provided approximately two thirds of the consultations each year. The median consultation time for biomedical doctors was 30 minutes and for other practitioners, the median consultation time was 1 hour (Fig. 2). In the fourth year, the clinic became financially viable.
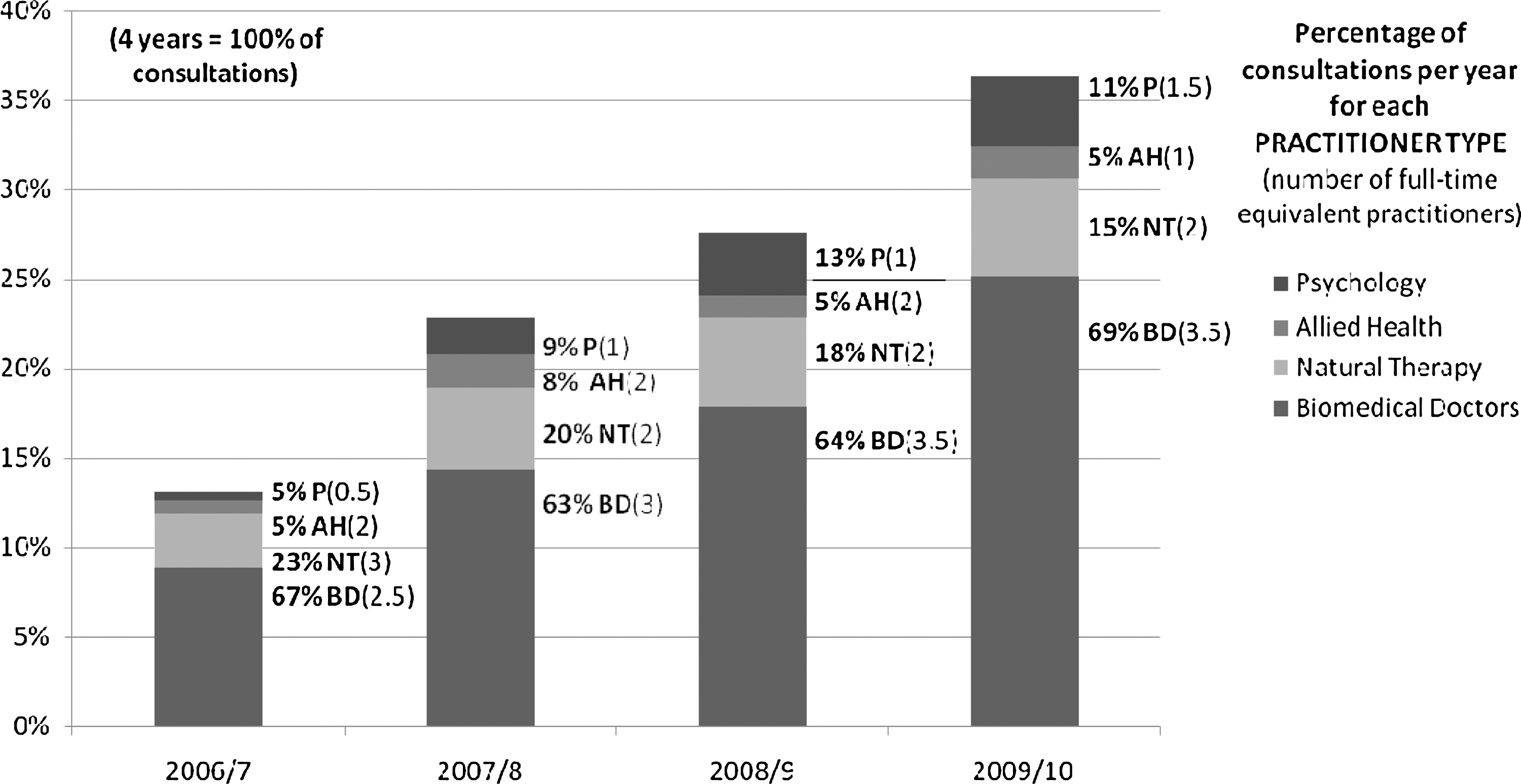
Percentage of the total 4 years of patient consultations per year by practitioner group (May 1, 2006 to April 30, 2010). Allied Health is defined as services provided by nonmedical practitioners who are recognized by the Australian Government for Medicare funding and are not a biomedical doctor. The category includes dietitians, exercise physiologists, chiropractors, osteopaths and physiotherapists. Natural Therapy includes all other traditional, complementary, and alternative medicine (TCAM) practitioners.
The clinic was computerized and used integrated clinical records. Except for highly confidential psychology notes, all practitioners could enter and access all clinical information. The clinical software was the most common software used in general practice in Australia. Its main limitations for use in an IM setting were that many of the functions were only relevant to the biomedical doctors and the majority of the natural-medicine products had to be entered into the prescribing software so that medications, both pharmaceutical and natural, were listed together. This also meant that the system lacked an automatic function to flag potential drug–herb–nutritional interactions.
The clinic participated in a national accreditation program for primary-care clinics. However, the accreditation body was designed to assess conventional primary care clinics rather than those offering IM, and there were no accreditation bodies in Australia for TCAM or IM clinics. Therefore, aspects of the clinic's activities that were beyond the scope of conventional primary care were not reviewed by the accreditation body.
Ninety-seven (97) patients (56 females and 37 males) who had seen a biomedical doctor completed the satisfaction questionnaire. Virtually all of the patients (94/97) stated that they were “very satisfied” with all 16 aspects of the clinic. Three (3) patients marked the next level down, “satisfied,” for a few questions and “very satisfied” for the remainder.
Success factors
Many of the components outlined in the introduction of this article as important for a successful IM clinic were met. Results from the staff questionnaire and observations from clinic meetings showed that there was general agreement among the practitioners of a shared vision, an open-minded culture, credible supporters, suitable facilities, and confidence in the clinical competency of the other practitioners. Generally, practitioners believed that they and the other practitioners provided patient-centered care.
In an effort to create an economically sustainable environment and develop the service, the directors took a pragmatic approach and remained amenable to trying new ideas. The directors explored different marketing strategies and tried various therapies and clinical services. Sound financial planning was essential for the clinic's survival, especially factoring in the capacity to run at a loss in the early years to allow time for the business to grow. The financial pressures required strong leadership and commitment from the directors to see the clinic through its toughest times.
Challenges
The overriding concern for this clinic was to create a sustainable business while fulfilling the vision of the directors—to create a center for excellence in the practice of IM. This was not without its costs and compromises. The challenges encountered were: managing high staff and practitioner turnover; finding the right balance between biomedical doctors and other practitioners and the services they offered; creating an IM team; and building research capacity.
By the end of the study period, the clinic had employed its fourth practice manager. Typical issues arose that can occur with any employment, particularly in a new business, such as problems with personality, management styles, competency and role overload. The common theme however was that, although the first three managers were experienced practice managers, none of them had experience working in an IM clinic with a variety of practitioner types. This called for new organizational and interpersonal skills, including the ability to respond to a wider and complex range of patient and practitioner needs. Eventually the clinic promoted a receptionist with previous non-health managerial experience, who performed well and was free of preconceptions about clinic management.
Practitioner turnover was also a problem. The clinic opened with 13 practitioners: 5 biomedical doctors; 1 dietitian; 1 exercise physiologist; 1 psychologist; 3 naturopaths, 1 Traditional Chinese Medicine practitioner; and 1 shiatsu practitioner. Over the first 4 years, 20 practitioners came and went, including: 6 biomedical doctors; 3 naturopaths; 3 nutritionists; 3 dietitians; 2 exercise physiologists; 1 physiotherapist; 1 masseuse; and 1 chiropractor. The most common reason for practitioners leaving the clinic was insufficient patient numbers and, therefore, lack of personal income.
It was very difficult for the clinic to find highly skilled practitioners who also had the charisma and drive to build their own patient bases. Most practitioners had to build their patient bases from scratch. This proved to be slow and difficult. Early on, the clinic tried many different marketing techniques. However, the most successful was word of mouth.
In the case of biomedical doctors, it was hard to find clinicians with adequate IM training and knowledge. Many started in the clinic with open minds but had limited TCAM knowledge. Those who have remained have been active in self-directed learning to expand their skill base in IM.
Regarding allied-health and TCAM practitioners, the biggest challenge was building a sustainable patient base. This, in turn, affected the clinic's ability to offer a comprehensive range of services, because many practitioner types (especially those offering physically based therapies) left the clinic.
The reasons given by practitioners for why it was difficult to build a patient base were: 1. Not enough referrals from biomedical doctors within and outside the clinic 2. The challenge of establishing a point of difference from biomedical doctors in the clinic who had similar skills 3. Aspects of the business model that removed the pressure on practitioners to pay a service fee irrespective of throughput, and prevented natural therapists from making commissions from selling products and generating return customers by selling elite products that were difficult to find elsewhere.
In response to feedback from patients and staff, the directors tried a variety of approaches to build the business. This included trying different multidisciplinary speciality health programs; and encouraging patients with complex health problems to see a range of practitioners, including joint consultations, in which the practitioners worked together to formulate a management plan. However, there was little or no demand for these services and the comment from some practitioners was that patients had stated they often felt “overserviced”.
Forming a strong cohesive team was a challenge. Practitioners commented that team building was constrained by: high turnover of staff and practitioners; little opportunity for formal team building; limited face-to-face contact with other practitioners (communication between practitioners relied heavily on shared clinical records, electronic correspondence, and corridor conversations); time and financial pressures; and a lack of indepth understanding about what the other practitioners did. Comments from the staff questionnaire indicated that biomedical dominance also affected team building negatively. *
Although the directors and many practitioners wanted to undertake research, it had yet to become an integral part of the clinic's culture. For example, they used an unpublished patient satisfaction questionnaire and administered it, using no scientific rigor. Another example was the presumption that, in choosing the most popular software used in Australia, data for health services and clinical data would be extracted easily for research purposes; this turned out not to be the case. Both the administration and clinical software had very limited search functions and did not use a standardised coding system.
Discussion
As the clinic evolved, it became apparent that the business model required that at least half the team be biomedical doctors, because they were the main income generators and an important referral source for the other practitioners. The available data made the current authors unable to explain fully this greater demand for biomedical doctors.
Extended consultation time is a factor commonly cited by users and providers of TCAM and IM as a reason that patients seek this style of care. 13,23 However, this does not explain the greater demand for biomedical doctors in the clinic, because other practitioners generally spent more time with patients. Studies have identified other factors, such as practitioner empathy, holistic care, and a patient-centered approach, as reasons patients seek TCAM and IM. 7,13,23 However, it is unlikely that the biomedical doctors in the clinic were better at providing this style of care compared to the other practitioners.
Another contributor may have been the greater range of services provided by the biomedical doctors. As well as offering selected TCAM/IM services, these practitioners provided biomedical services that the other practitioners were not trained and/or legally permitted to provide. Furthermore, the Australian general practitioner is the gatekeeper to subsidized testing, biomedical specialists and the tertiary-hospital sector.
In keeping with an in-depth review of patients attending three other IM clinics in Sydney, Australia, 7 it is possible that the clinic's patients may perceive that there is “enhanced safety” gained from visiting biomedical doctors. This raises interesting questions about how patients might be reconciling a conservative modern scientific approach with more postmodern ideologies that reject science as the only truth and that are often attributed to the rise in popularity of TCAM. 24
In Western societies, biomedical doctors are still at the top of the hierarchy in the health care system. 25 The social mindset of patients, receptionists, and practitioners will unwittingly generate a higher demand for biomedical doctors. Biomedical dominance along with further exploration about the IM team will be discussed in more detail in a second article.*
Out-of-pocket costs to patients (for consultations with practitioners and natural therapy products) were often considerable. As such, economic theory suggests that the clinic was providing a luxury service. The willingness-to-pay by a growing patient base provided weak evidence to suggest that at least some aspects of health care needs were being met.
Although the directors planned for the clinic to undertake research, capacity was limited. A lack of research culture and difficulties with using Australian clinical software for research purposes was not unique to this clinic. 26,27 Another Australian research group evaluating primary care reported similar frustrations with using the common general practice software packages. 28
In Australia, coding of symptoms, diseases, or management are not requirements of clinical governance nor of service payment. As such, there is little incentive to build these functions into clinical software in this country. However, even if systematic coding were to become a feature of the clinical software, aside from Traditional Oriental Medicine, as yet there are no internationally agreed coding systems for other TCAM therapies nor for IM. 29
Regarding the limitations of this study, neither of the questionnaires were standardized tools; therefore, the validity and reliability of the results are unknown. Much of the content of the practitioner questionnaire was in response to the literature rather than arising from discussions with practitioners and patients. However, the large number of open-ended questions provided many opportunities for practitioners to discuss other issues. Nevertheless, indepth interviews would have generated much richer data. The patient sample was likely to be biased because patients filled out the questionnaire on an ad-hoc basis (i.e., neither consecutively nor randomly sampled). Therefore, the current authors still have very limited information about the patients' experiences.
Conclusions
After 4 years, this clinic had succeeded in creating a sustainable business offering a range of IM and TCAM services in a multidisciplinary primary care setting. The challenges were many, often reflecting the tension between high ideals and economic necessity. This affected the development of the IM team and the range of services offered.
The development of IM clinics is still in its early stages. Irrespective of scientific evidence for effectiveness, there is an increasing market demand for this style of medicine and more IM clinics are appearing across the globe. Therefore, it is important to describe and evaluate existing IM clinics to promote understanding regarding their advantages and disadvantages, and the models of health care provided. The use of mixed methods is appropriate for IM health service evaluation.
Footnotes
Disclosure Statement
Dr. Phelps is the owner and medical director of the clinic. Aside from indirect financial benefit from improving the reputation of the clinic through publishing research, Dr. Phelps has no competing financial interests.
No competing financial interests exist for the other three authors.
*
In press: JACM-2011-0393.R3 December 2012.