
Abstract
Objectives:
This study evaluated the effects of Class IV laser therapy on pain, Fibromyalgia (FM) impact, and physical function in women diagnosed with FM.
Design:
The study was a double-blind, randomized control trial.
Setting:
Testing was completed at the university and Rheumatologist office and treatment was completed at a chiropractic clinic.
Participants:
Thirty-eight (38) women (52±11 years; mean±standard deviation) with FM were randomly assigned to one of two treatment groups, laser heat therapy (LHT; n=20) or sham heat therapy (SHT; n=18).
Intervention:
Both groups received treatment twice a week for 4 weeks. Treatment consisted of application of LHT or SHT over seven tender points located across the neck, shoulders, and back. Treatment was blinded to women and was administered by a chiropractic physician for 7 minutes.
Outcome measures:
Participants were evaluated before and after treatment for number and sensitivity of tender points, completed the FM Impact Questionnaire (FIQ) and the pain question of the FIQ, and were measured for function using the continuous scale physical functional performance (CS-PFP) test. Data were evaluated using repeated-measures analysis of variance with significance accepted at p≤0.05.
Results:
There were significant interactions for pain measured by the FIQ (LHT: 7.1±2.3 to 6.2±2.1 units; SHT: 5.8±1.3 to 6.1±1.4 units) and for upper body flexibility measured by the CS-PFP (LHT: 71±17 to 78±12 units; SHT: 77±12 to 77±11 units) with the LHT improving significantly compared to SHT. There was a time effect for the measure of FM impact measured by the FIQ, indicating that FM impact significantly improved from pre- to post-treatment in LHT (63±20 to 57±18 units), while no change was observed in the SHT (57±11 to 55±12 units).
Conclusions:
This study provides evidence that LHT may be a beneficial modality for women with FM in order to improve pain and upper body range of motion, ultimately reducing the impact of FM.
Introduction

Tender point locations for women with fibromyalgia.
The etiology of FM is not known, and the prognosis for recovery in traditional medicine is generally poor. Traditional therapies include pharmacologic interventions such as tricyclic antidepressants, nonsteroidal anti-inflammatory drugs, anti-epileptic drugs, sedatives, muscle relaxants, and opiates. 10 The results of these drug interventions have been mixed, with some improvements in pain, sleep, fatigue, and mood. 10 It has been suggested that pharmacologic interventions achieve symptom relief for fewer than 50% of the FM population. 11,12 Drug interventions are also associated with a number of side-effects such as weight gain, morning “hangover,” gastrointestinal distress, and increased tolerance to the drug therapy overtime. One study found that 47% of the women with FM were nonadherent with their medication. 13 Due to the negative side-effects associated with pharmacological management, it is not surprising that nonpharmacological interventions have increased in popularity. In one survey, it was found that 91% of individuals with FM used some form of alternative medicine compared to 42% of the general population 14 ; however, there is no consensus on which type of alternative intervention is most beneficial for reducing pain and improving FM impact.
One alternative intervention that may be beneficial to women with FM is Class IV laser therapy. Therapeutic lasers have been studied extensively. However, published studies on the use of laser for pain or common musculoskeletal conditions appear to be predominately on Class IIIb lasers. 15 –22 Therapy lasers use light energy to modulate cell and tissue physiology to achieve therapeutic benefit. 15 The light produced consists of coherent beams of single wavelengths in the visible to infrared spectrum, which can be emitted in a continuous wave or pulsed mode. 15 Class IIIb lasers as classified by the Center for Devices and Radiological Health (CDRH) have an average radiant power less than 0.50 W. Like the IIIb lasers, recently developed Class IV therapeutic lasers use diffuse light at wavelengths in a therapeutic window that allow penetration of the light deep into the tissue. Class IV lasers are classified by CDRH as having an average radiant power greater than 0.50 W. While studies on Class IV lasers exist, a majority are on surgical lasers. 23 Surgical lasers use focused beams of light at wavelengths that are highly absorbed by water to cut tissue in surgical applications. Clinically available Class IV therapy lasers are up to 30 times stronger than Class IIIb lasers and allow for delivery of a therapeutic dose deep in the tissue in a shorter amount of time. This development has led to the use of Class IV lasers to treat a variety of conditions including skin lesions, 24,25 acute soft-tissue injuries, 26 and chronic pain syndromes 27 such as FM. Although Class IV lasers are being used clinically by a variety of practitioners, standards and treatment regimens are evolving and have not yet been clearly defined by controlled clinical studies.
The purpose of the proposed study was to examine the effects of Class IV infrared, therapeutic laser therapy in women who have been diagnosed with FM. It was hypothesized that 4 weeks of infrared laser therapy would reduce FM impact and improve functionality in women with FM.
Materials and Methods
Of the 95 women who called to express interest in the study, only 42 women with FM participated. See Figure 2 for progression of participants through study. Participants were excluded if they had uncontrolled hypertension (160/100 mm Hg or higher), uncontrolled diabetes, active heart disease, known history of cancer, long-term corticosteroid use, pregnant or planning to get pregnant, endocrine disease, anticoagulant therapy, bleeding disorders, history of stroke, a chronic infection, any type of malignancy, if they were taking medications that caused sensitivity to light, if they had a physical examination or radiological findings that would contraindicate the use of light or thermal therapy, and/or currently under the care of a chiropractic physician, acupuncture physician, massage therapist, or other forms of manual therapy. Approval of the study was obtained from the Institutional Review Board for Human Subjects Committee. Participants received $100.00 for participating in the study. Fifty dollars ($50.00) was given after the end of pretesting and another $50.00 was given at the completion of the study.
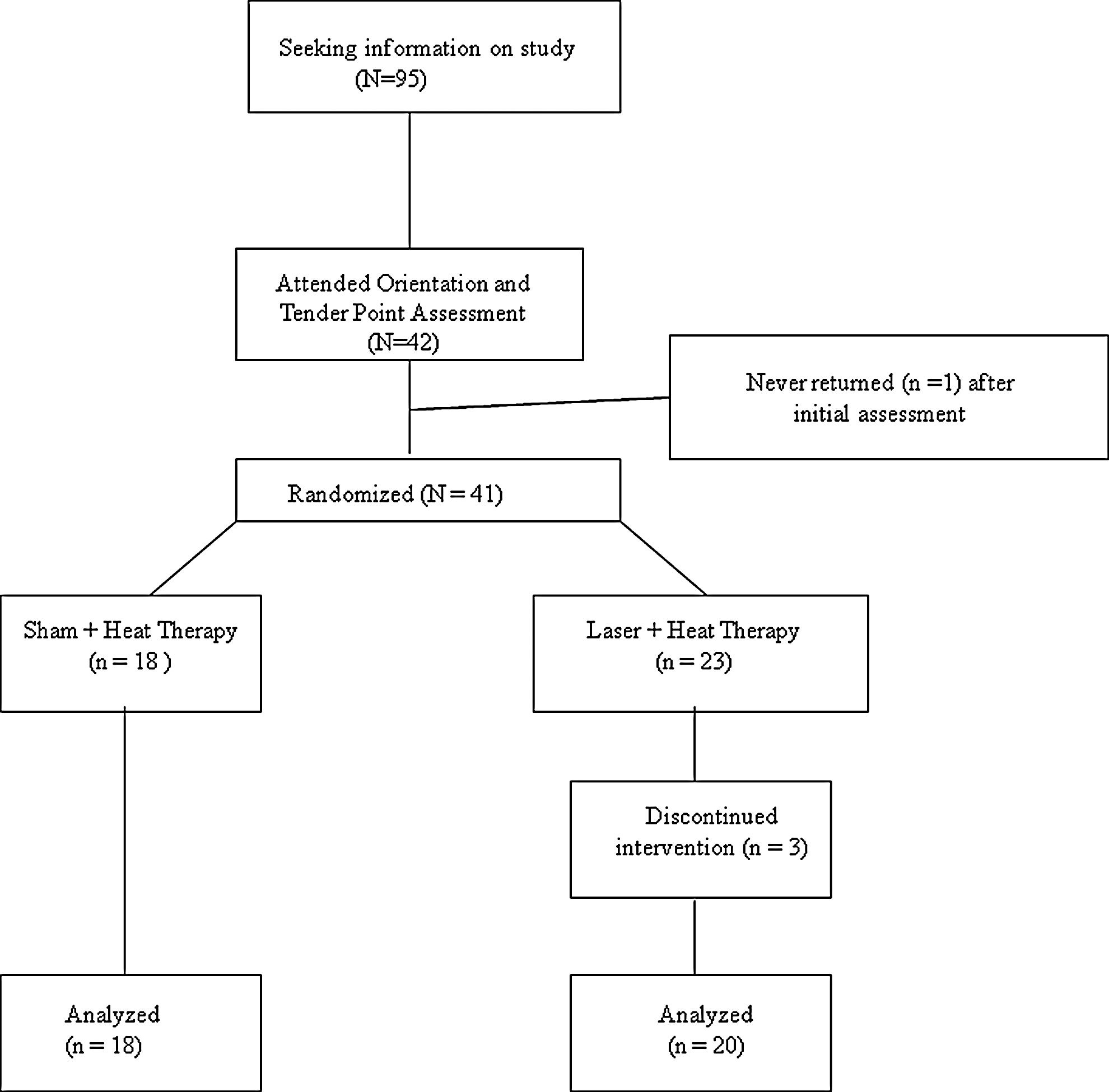
Progression of participants through study.
The initial visit was an orientation session where written informed consents were signed, questionnaires on demographics and medical history were completed, and the tender point assessment was performed by a board-certified rheumatologist. Participants were asked to refrain from pain medication 24 hours prior to seeing the rheumatologist. The rheumatologist determined the number of tender points (Fig. 1) and rated the sensitivity of pain on a scale of 0 (no pain) to 3 (withdrawal of patient from examiner) of each tender point to determine myalgic score. 28 Each of the 18 tender points is evaluated, with the highest possible myalgic score being 54. Myalgic score is a subjective rating given by the physician to describe the sensitivity of a tender point when pressure is applied. Test–retest correlations for tender-point evaluation and myalgic score of 12 women with FM in our previous research was r=0.80 and r=0.60, respectively. To be diagnosed with FM, a person must present with at least 11 tender points out of the possible 18. 29 Therefore, at least 11 out of 18 specified tender points were required for eligibility to participate in the study. Analyses were also completed on just the eight tender points that are located on the back of the body where treatments were given. Myalgic score was also calculated for these eight tender points.
On the second visit, height and weight, FM Impact Questionnaire (FIQ), and physical function using the Continuous Scale Physical Functional Performance (CS-PFP) test were measured. The FIQ can be broken down into three subscales that measure physical function (instrumental ADL), general-well being, and FM related-symptoms. 29 The FIQ consists of 20 questions pertaining to morning stiffness, mood, pain, and the ability to perform ADL. Scores range from 0 to 100 units; the higher the FM impact score, the greater the impact of disease on quality of life. On average, individuals afflicted with FM score about 50 units, while a severely impacted individual scores above 70 units. Construct validity for the FIQ has been demonstrated through correlations of FIQ scores for physical impairment, pain, depression, and anxiety with the Arthritis Impact Management Scale (r=0.67–0.76). Test–retest correlations range from 0.56 with pain to 0.95 for the physical function scale. 30 Since pain was a primary interest of the study, question number 15, “How bad has your pain been?” of the FIQ was also analyzed. This question was on a 10-point scale, with 0 being “No pain” and 10 being “Very severe pain.”
The 10-item CS-PFP was used to evaluate function.
31
This test has been validated in older adults
32
and has been used in previous studies with women with FM.
7,33,34
Functional performance is measured by simulating tasks of routine activities. The CS-PFP was based on ordinary routine tasks, performed at maximal effort within the bounds of safety and comfort. Ten (10) tasks were administered, and a combination of time, distance, and weight was used to quantify performance. Tasks quantified using both weight and time included (1) pot carrying and (2) carrying groceries. Tasks quantified by time alone included (3) transferring laundry from washer to dryer and from dryer to basket, (4) putting on and removing a jacket, (5) floor sweeping, (6) climbing stairs, (7) getting down and up from the floor, and (8) picking up four scarves from the floor. Tasks that were quantified by distance alone included (9) 6-minute walk and (10) highest reach. Time was used to calculate speed, so that higher numbers reflected higher function for each unit of measure (weight, distance, and speed). Each task was scaled 1–100 according to the following formula:
The total CS-PFP score (CS-PFP total) was the average corrected score of all tasks. The CS-PFP total was also broken down into domains representing upper body strength, upper body flexibility, lower body strength, balance and coordination, and endurance.
The laboratory for administration of the CS-PFP was set up to adhere to published dimensions 32 and was administered using the published protocol 35 along with a scripted dialog with minor changes tailored to this laboratory. Participants wore Polar™ heart rate monitors throughout the entire test so heart rates could be monitored. Ratings of perceived exertion were also taken from the participants at the end of the entire test to get a subjective level of perceived exertion. 36
After completing the initial testing, participants were randomly assigned, by picking a number out of a hat, into one of two groups: a treatment group that received laser and heat therapy and another group that received sham and heat therapy. Because of the thermal affects associated with Class IV laser, and because the laser manufacturer's website specifically mentions the “soothing warmth” of laser therapy, a sham and heat therapy treatment was designed to disguise true laser treatment from sham treatment. The device for the treatment was designed to force warm air, provided by a commercially available air warmer through a tube. The air warmer was mounted out of view inside a vented cart upon which the laser was mounted so as to appear as a single unit. The air warmer was mounted to a short section of insulated pipe, which was then attached to a T fitting with a gate valve attached to one side and the warm air supply hose attached to the opposite side. The gate valve was used to control the flow of warm air. The warm air supply hose was then bound together with the laser's fiber-optic cable with zip ties, and wound with white elastic tape to obscure both the tube and the fiber-optic cable. The air supply tube was routed through a hole drilled in the laser handpiece so that warm air could be delivered alone for the sham and heat therapy or in tandem with the laser for the laser and heat therapy. The same device was used for both groups, so the treatment group received both laser and warm air, and the sham group received only warm air. Although neither the skin temperature, nor the warm air output of the treatment device was measured, an effort was made to standardize the heat treatment by utilizing the same medium heat setting for each treatment preceded by a warmup period of approximately 5 minutes to provide a consistent application of warm air at approximately the same temperature from treatment to treatment. The air flow and temperature were adjusted by way of the gate valve and the air warmer's heat settings in an attempt to mimic the warmth associated with the Class IV laser with sufficient warmth so that participants could not discern whether they received the laser treatment or the sham.
Treatment was designed to be consistent with the laser manufacturer's recommendations and consisted of twice-weekly sessions for 4 weeks for a total of 8 sessions. The duration of each session was approximately 15 minutes, while actual treatment time was 7 minutes. During the treatment sessions, the participants were either gowned, or wore a sports bra to expose the skin of the cervical, thoracic, and lumbar regions. Participants were positioned face down on a treatment table or a massage chair, depending upon their comfort and preference. Participants wore eye protection with an optical density rating >5.0 at 810 nm and 980 nm in order to protect their eyes and further obscure which treatment they received. To ensure consistency between the laser and heat and sham and heat group, the treatment targets consisted of seven tender points used as part of the diagnostic criteria to establish a diagnosis of FM (Fig. 1). Treatment was delivered to an area approximately 2.5 inches×3.5 inches or approximately 56.45 cm2 to conform to LiteCure's manual “Clinical Overview and Application of Class IV Therapy Laser” written by Riegal and Pryor.
For the laser group, treatment was rendered utilizing a LCT-1000 (LiteCure LLC, Newark, DE) solid-state GaAlAs laser delivering a continuous-wave, dual-wavelength laser with 20% 810 nm, and 80% 980 nm at 10 W. Each 56.45 cm2 treatment point was treated with laser at 10.63 J/cm2 and warm air utilizing a grid scanning technique to avoid overheating tissue. Participants were instructed to expect some warmth but that the treatment should not burn and to provide verbal cues if the treatment spots became excessively warm. Each treatment point was treated for exactly 60 seconds for a total of 600 J per point, for a total daily treatment dose of 4200 J. The dual wavelength was used for two reasons: (1) this is what is commercially available and (2) two wavelengths allow for treatment in patients with different skin colors since different melanin concentrations will absorb light differently. Both wavelengths are in the accepted therapeutic window. The sham treatment consisted of 60 seconds of warm air alone over the seven tender points. A timer was used to ensure that each area was treated for exactly 60 seconds so that the treatment time was identical for both groups. At the completion of the 4-week intervention, participants repeated all the testing that was completed initially. Investigators measuring tender-point sensitivity, FIQ, and functionality were blinded to the group assignment of the participants. Only the chiropractor delivering treatment was aware of group assignments. Participants were also blinded to their group assignment.
One-way analysis of variance (ANOVA) was used to determine whether there were initial differences in baseline data. Dependent variables were analyzed by a two-way (group×time) ANOVA with repeated measures. When interactions were significant, one-way ANOVA was used to compare pre- and post-training values within groups. If there were sphericity violations, the Greenhouse-Geisser adjustment was used to test the effects of experimental condition and time interactions on the dependent variables. Data are presented as means±standard deviations. All significance was accepted at p≤0.05. All analyses were performed using SPSS (version 19.0).
Results
Of the 42 women who attended the orientation and tender-point assessment, 38 women completed the study. One woman never returned after initial assessment, 2 women randomized to the laser group dropped out due to scheduling conflicts, and 1 woman also randomized to the laser group was severely depressed during post-testing and could not complete the testing procedures. Table 1 presents the participant characteristics. Of the 38 women who completed the study, 36 were white and 2 were African American. The 2 groups were not significantly different on baseline measurements of age, height, weight, body mass index, and years with FM.
Values are means±standard deviation.
BMI, body mass index; FM, fibromyalgia.
Table 2 presents the data for the two groups before and after treatment for FM impact and functionality scores. There were no differences between the two groups in baseline measurements. Two (2) women did not complete the pain question of the FIQ, 1 from each of the 2 groups, therefore only data from 36 women were analyzed. There was a significant interaction for pain measured by the pain subscale of the FIQ (F(1,34)=4.79, p≤0.05, effect size (ES)=12). Pain decreased significantly for the laser and heat therapy group compared to a nonsignificant increase in the sham and heat therapy group. There were no other significant interaction effects for the other measures of FM impact measured by the number of tender points, myalgic score, and the total score of the FIQ between the two groups. There were, however, significant time effects for all measured parameters of FM impact. When evaluating the pre- to post-differences for the total score of the FIQ, only the pre- to post-measurement for the laser and heat group was significant. There was no difference in pre- to post-measurements of the FIQ for the sham and heat group.
Values are means±standard deviation.
p≤0.05, significantly different from pre-test measurements.
Eight tender points were evaluated where treatment was administered and myalgic score was evaluated for those eight tender points.
p=0.07, significantly different from pre-test measurements.
p=0.06, significantly different from pre test measurements.
p≤0.05, significantly different from Sham + Heat Therapy Group.
FM, fibromyalgia; FIQ, Fibromyalgia Impact Questionnaire; FIQ Pain, Question on pain taken from Fibromyalgia Impact Questionnaire; UBS, upper body strength domain calculated from the continuous scale physical functional performance test; UBF, upper body flexibility domain calculated from the continuous scale–physical functional performance test; LBS, lower body strength domain calculated from the continuous scale–physical functional performance test; BALC, balance and coordination domain calculated from the continuous scale–physical functional performance test; END, endurance domain calculated from the continuous scale–physical functional performance test; CS-PFP total, total score for the continuous scale–physical functional performance test; RPE, rating of perceived exertion.
The functionality measurements are also presented in Table 2. There was a significant interaction effect (F(1,36)=9.6, p≤0.05, ES=21) for the upper body flexibility domain. There was a significant improvement in this domain for the laser group compared to the sham group. There were significant time effects for all other measured variables of functionality.
Discussion
There are only a few studies that have used laser therapy to treat pain 16,17,27,37,38 and no studies that have evaluated objective measures of function (CS-PFP test) and laser therapy in women diagnosed with FM. It is known that FM can substantially impair function, negatively impacting the ability to carry out normal activities of daily living, and thereby impact quality of life. 7,39,40 The results of this study are promising in that pain measured by the subscale of the FIQ and the function domain of upper body flexibility as measured by the CS-PFP test significantly improved after laser and heat treatment compared to the sham and heat treatment. There was also a significant pre- to postimprovement of FM impact measured by the FIQ after laser and heat treatment.
Although women with FM have widespread pain across the body, a majority of their tender points and pain are clustered around the upper back and neck regions. The proposed mechanism of pain in this population has been attributed to the central nervous system due to a combination of factors that may include genetic predisposition, neuroendocrine changes, and imbalances in neurotransmitters such as serotonin, dopamine, norepinephrine, substance P, and nerve growth factor. 41 –43 Little attention has been given to peripheral nociceptive inputs in FM. However, research is being completed to evaluate the mechanisms and treatment of localized muscle pain from the myofascial trigger points. 44,45
Class IV lasers may be a noninvasive and nonpharmacological way to initially treat peripheral pain in women with FM before undergoing other treatments. Class IV lasers used for therapy generate high-intensity monochromatic beams of coherent light. The laser used in this study was a dual wavelength laser split at 20% 810 nm, and 80% 980 nm in the infrared spectrum, which helps to treat patients with different skin types since melanin concentrations will absorb light differently. Although there is some thermal effect associated with Class IV laser therapy, the therapeutic effect is due to photochemical reactions in the cells. 46 Studies suggest that Class IV lasers have a beneficial analgesic and anti-inflammatory effect in humans. 47 –50 Therefore, it was hypothesized that the laser therapy would have therapeutic benefits in helping to improve pain and function in women with FM.
In the present study, the women had an average FIQ score of 61±16 units with a mean tender point score of 14±3. On average, individuals afflicted with FM score about 50 units, while a severely impacted individual may score above 70 units. 29 The average total functionality score of the women in the present study was 44±15 units, which is lower than what is reported for older adults (>70 years at 54±11 units) living in the community. 32 The total functionality score of the women in the present study is similar to what has been reported in residents living in a retirement community of 42±15 units. 32 Therefore, the women in the present study were suffering from the effects of FM and having limitations in their routine ADL.
After the intervention, only the laser and heat therapy group significantly improved rating of pain from the subscale of the FIQ. Pain ratings decreased by 12.7% in the laser and heat group and increased by 5.1% in the sham and heat group. The laser and heat therapy group also had a significant pre- to post-improvement of the FIQ by 9.5%, while the sham and heat group had a nonsignificant improvement of 4%. The laser and heat group as well as the sham and heat group both significantly increased total function scores by 19.5% and 8.2%, respectively, as well as improving the domains of the CS-PFP test of upper body strength (18.2% versus 10.5%), lower body strength (21.9% versus 12.8%), balance and coordination (20.9% versus 9.8%), and endurance (20.9% versus 8.2%). Although there were no significant differences between treatments, the laser and heat group did have slightly greater improvements than the sham and heat group. This could be due to the baseline scores of the laser and heat group being lower, although baseline values were not significantly different between groups. Nevertheless, there was a significant improvement in upper body flexibility for the laser and heat group by 9.9% compared to no change in the sham group. This has important health implications since women with FM have a great deal of limitations from their disease in upper body movement.
One of the reasons that greater changes may not have been seen between the laser and heat and sham and heat groups was due to the sham group also receiving heat over the tender points. Heat has been shown to have therapeutic properties in women with FM. 51 –54 Fioravanti et al. 51 found that 12 sessions of mud packs and thermal baths over a 2-week period significantly decreased FIQ scores, visual analog scale scores of headache, fatigue, sleep disturbances, and gastrointestinal symptoms as well as the number of tender points. Balneotherapy, which is practiced at spas, involves treatments that use heated mineral water, massage through moving water, and relaxation; this has also been shown to improve FM symptoms. 53,54 Evcik et al. 54 found that after balneotherapy, women with FM had decreases in FIQ, pain intensity, and number of tender points. Thus, the heat that was generated from the air warmer may have helped to decrease the scores of the FIQ and tender points by increasing blood flow, relaxing the muscle, and decreasing the pain felt in the tender points. However, the women in the laser and heat treatment group had additional benefits with greater reductions in FIQ from pre- to post-testing as well as reduction in pain measured from the subscale of the FIQ and upper body flexibility measured by the CS-PFP test.
Greater changes between the laser and heat and the sham and heat groups may also have been seen if the frequency of therapy was greater or if the duration of treatment was longer. In both studies by Gur et al., 16,17 they used Class IIIb lasers with a 2-week treatment period of 5 days/week for a total of 10 treatments for their patients with FM. Each tender point was exposed to 3 minutes of laser treatment. Both studies had reductions in pain, tender points, and FIQ sores. In a review of Class IIIb laser therapy for neck pain, Chow et al. 15 presented treatment durations lasting 1.5–7 weeks with treatments ranging from twice a week to 5 times/week. Total treatments sessions for the reviewed studies ranged from 5 to 15. The participants in the current study received twice-a-week treatment for a period of 4 weeks totaling 8 treatment sessions. This study's eight treatment sessions fall in the middle of number of treatments in the reviewed studies of Class IIIb lasers. Perhaps increasing the number of sessions would have enhanced this study's outcome measures. More research is needed to evaluate the optimal treatment period and frequency of treatment for Class IV laser therapy. Research is also needed to determine once treatment is terminated how long benefits in function and reduction in pain will continue and whether intermittent treatment can maintain these benefits.
Conclusions
The use of a Class IV laser and/or heat therapy reduces pain and improves functionality in women with FM. In addition, Class IV laser therapy significantly reduced FM impact by decreasing pain measured by the subscale of the FIQ and increased the upper body flexibility domain of functionality compared to the sham and heat group. These data suggest that the use of a Class IV laser may be another treatment option for women suffering with FM.
Footnotes
Acknowledgments
This study was funded by Litecure.
Disclosure Statement
No competing financial interests exist for any of the authors.