
Abstract
Objectives:
This study assessed the importance of the Traditional Chinese Medicine (TCM) pattern on an acupoint-specific effect.
Design:
This was a TCM pattern subdivision analysis of the first intervention data from a multicenter, randomized, controlled trial (ISRCTN24863192) (the main trial).
Settings:
The main trial recruited participants from six hospitals in three provinces in China.
Subjects:
Five hundred and one (501) participants diagnosed with primary dysmenorrhea (PD) were enrolled in the main trial.
Interventions:
The main trial randomly and equally divided participants into three treatment groups with bilateral electroacupuncture at three sites, respectively: Sanyinjiao (SP6), Xuanzhong (GB39), and an adjacent nonacupoint. Participants were diagnosed with TCM patterns before the treatment. The intervention was carried out when the visual analogue scale (VAS) score of participant's menstrual pain was ≥40 mm on the first day of menstruation and lasted for 30 minutes.
Outcome measures:
The immediate improvement of pain was measured with a 100-mm VAS before the intervention, at 5 minutes, 10 minutes, and 30 minutes during the intervention, and at 30 minutes after the completion of this intervention.
Results:
Three (3) TCM patterns (n=320) were eligible for analysis, including Cold and Dampness Stagnation pattern (n=184), Qi and Blood Stagnation pattern (n=84), and Qi and Blood Deficiency pattern (n=52). In Cold and Dampness Stagnation pattern, the SP6 group had a significant reduction in VAS scores compared with the GB39 group (mean difference −7.6 mm) and the nonacupoint group (mean difference −8.2 mm), respectively. There was no difference between the latter two groups. There were no group differences in VAS scores in the other two patterns.
Conclusions:
It suggested that TCM pattern might affect acupoint specific effect on the immediate pain relief obtained for participants with PD.
Introduction
The Traditional Chinese Medicine (TCM) pattern is an organic combination of clinical symptoms and signs, and pattern differentiation is considered crucial for the therapeutic effect according to TCM theory and clinical practice. Acupuncture has been practiced for more than 2500 years in the Western Pacific Region, 9 and the acupoints are derived for and have long been used for curing one or several symptoms and/or signs (e.g., TCM pattern). Thus, understanding the role of the TCM pattern is important both for acupuncture clinical practice and the design of research trials. 10 –12
Although acupuncture has been recommended by the National Institutes of Health as an effective tool for menstrual pain, 13 four systematic reviews, including two Cochrane reviews, concluded that the evidence for the effectiveness of acupuncture for the treatment of PD was insufficient and further research was needed. 14 –17 Since then, three recent published trials from the authors' research group found that acupuncture could immediately relieve the pain of PD and even minimized the influence of pain on daily life. 18 –20
For dysmenorrhea, Sanyinjiao (SP6) is found to be one of the most commonly used points in the clinical practice and research of acupuncture. 21 –24 Two (2) of the authors' previous studies 18,19 suggested that SP6 has a specific effect on immediate improvement of menstrual pain. Therefore, this study presents a TCM pattern subdivision analysis of data from a multicenter, randomized, controlled clinical trial (ISRCTN24863192) (referred as “the main trial or study” in this article) to explore whether pattern differentiation is related to acupoint (SP6)-specific effect.
Two (2) sham acupuncture treatments were designed according to the authors' purpose and a study 25 recommendation. Xuanzhong (GB39), an acupoint rarely connected with dysmenorrhea 18,20 was chosen as an unrelated acupoint control and an adjacent nonacupoint was chosen.
Materials and Methods
This article focuses on reporting a TCM pattern subdivision analysis of data from the first intervention of the main study. The results of the main study are yet to be published.
Subjects and settings for the main trial
Five hundred and one (501) participants were recruited from six hospitals (Dongzhimen Hospital Affiliated to Beijing University of Chinese Medicine, China-Japan Friendship Hospital, Beijing Hospital of TCM affiliated to Capital Medical University, Huguosi Hospital of TCM affiliated to Beijing University of Chinese Medicine, the First Hospital affiliated to Tianjin College of TCM, and Shandong University of TCM) in three provinces (Beijing, Tianjin, and Shandong) in China between December 2008 and September 2009.
Eligible participants were nulliparous women 15–30 years of age in whom PD was diagnosed by physicians (according to the Primary Dysmenorrhea Consensus Guideline 26 ) and who had a global pain score of 40 mm or greater on a visual analogue scale (VAS) for at least 6 months before randomization. Participants were in good general health, had regular menstrual cycles (28 days cycle±7 days) and agreed to refrain from use of any analgesics 24 hours before the first intervention.
Participants were excluded if they were diagnosed as having secondary dysmenorrhea; were pregnant or preparing to become pregnant; reported dangerous diseases or mental illnesses; had previously received acupuncture treatment (to maximize blinding) or reported potential contraindications to aspirin (a medication given to participants for pain relief as needed).
Ethics approval of the main trial was gained from the Medical Ethical Committee of Dongzhimen Hospital Affiliated to Beijing University of Chinese Medicine (approval number ECPJ-BDY-2008-11-10). Each participant signed an informed consent prior to enrollment.
TCM diagnosis
The TCM pattern diagnosis criteria were designed according to Chinese national guideline, 27 which was based on the advice of the first-class experts in this field, and modified to fit this study. First, both Western Medicine and TCM principles were considered. The criteria made a subdivision of PD participants based on TCM pattern differentiation rules. Second, qualitative and quantitative measurements were combined. All the symptoms (signs) of each pattern were divided into two categories (primary and secondary symptoms), and both categories were given varying weights as described below.
The criteria had been used in a questionnaire investigation among 163 female college students with PD to detect TCM pattern distribution. The result was similar with former investigations published by other researchers.
28
It showed some practicability and credibility of the criteria. The next six paragraphs show the criteria, which included five patterns. • Cold and Dampness Stagnation pattern: primary symptoms: (1) cold lower abdominal pain before or during the menstrual period, alleviated by warmth; (2) scanty menses; (3) dark, clotted menses; (4) or menses like black soy bean milk; secondary symptoms: (1) intolerance of cold; (2) lack of warmth in the extremities; (3) profuse vaginal discharge; (4) white and greasy tongue coating; (5) wiry pulse; (6) or deep and tight pulse. • Qi and Blood Stagnation pattern: primary symptoms: (1) distending lower abdominal pain before or during the menstrual period, aggravated by pressure; (2) scanty menses; (3) impeded flow of menses; (4) dark purple menses; (5) with clots and alleviated by discharging of clots; secondary symptoms: (1) distention and pain of breasts before the menstrual period; (2) chest oppression; (3) dark purple tongue with or without purple spots; (4) wiry pulse; (5) or rough pulse. • Damp-Heat Obstruction pattern: primary symptoms: (1) distending or stabbing lower abdominal pain before or during the menstrual period, aggravated by pressure; (2) pain with burning sensation; (3) dark red menses, thick consistency with clots; secondary symptoms: (1) profuse vaginal discharge; (2) yellow and thick vaginal discharge; (3) or with fluctuating low fever; (4) or with distending pain of low back; (5) red tongue; (6) yellow or greasy tongue coating; (7) wiry and rapid pulse; (8) or slippery and rapid pulse. • Qi and Blood Deficiency pattern: primary symptoms: (1) dull lower abdominal pain after the menstrual period; (2) sagging sensation of lower abdomen and vulva; (3) preference for pressure; (4) scanty menses; (5) light-colored menses; (6) thin menses; secondary symptoms: (1) lusterless facial complexion; (2) lassitude of spirit; 3) pale tongue; 4) thready and forceless pulse. • Liver and Kidney Deficiency pattern: primary symptoms: (1) continuous lower abdominal dull pain 1 or 2 days after the menstrual period; (2) scanty menses; (3) dark, pale-colored menses; (4) thin menses; secondary symptoms: (1) dizziness; (2) tinnitus; (3) pain of sacrum and low back; (4) poor memory; (5) insomnia; (6) tidal fever; (7) pale red tongue; (8) deep pulse; (9) or thready pulse.
Each primary symptom was scored 2 points while a secondary symptom was scored 1 point. Primary and secondary symptom scores were added together as a total score. A pattern was identified if the total score equaled or more than 6.
Procedures and interventions
Participants were randomly and equally divided into three treatment groups with bilateral electroacupuncture (EA) at three acupoints, respectively: SP6 (located at the posterior border of the medial aspect of tibia, at 3 cun above the medial malleolus), GB39 (located at the anterior of fibula, at 3 cun above the tip of the external malleolus), and an adjacent nonacupoint (located on the lateral side of lower part of the leg, 3 inches above the tip of external malleolus, 1.5 inches behind anterior crest of the tibia, and tested in the authors' previous study 20 ). The participants were given TCM pattern diagnoses before treatment.
For each participant in the SP6 group, the intervention was carried out when the VAS score of menstrual pain was ≥40 mm on the first day of menstruation. Then the participant was asked to lie on the treatment bed in a supine posture. After disinfection, for one leg, the SP6 was punctured perpendicularly with one Ø0.25-mm×40- mm stainless, sterilized, and disposable needle (Hanyi, Beijing Hanyi Medical Instruments Center, Beijing, China) to a depth of 25–40 mm. The needling techniques of lifting-thrusting and twirling were used 3–5 times to induce a needling sensation (de qi) if possible. Then another needle (Ø0.25-mm×25-mm, stainless, sterilized, disposable, and from the same manufacturer) was inserted superficially to 2.5 mm and about 5 mm proximally away from the former needle without de qi (to be used as a stimulation lead of EA). The same procedure was performed on the other leg. Then one electric line with two leads connected two points on the same side. Four (4) points on both sides were stimulated simultaneously with alternating 2/100-Hz waves at the highest intensity each participant could tolerate (Han's Acupoint Nerve Electro-stimulator, HANS-200, Jisheng Medical Science and Technology Co., Ltd., Nanjing, China). The stimulation lasted 30 minutes. Similar acupuncture intervention was performed on each participant in the GB39 and nonacupoint group.
Sample size for the main trial
A sample size of 167 participants per group was calculated with an equation of repeated measures design 29 according to a previous study of our team 20 (two-sided 5% significance level, 80% power, mean difference of 3.2 mm with standard deviations of 21.74 mm on the VAS scores between SP6 group and GB39 group from baseline to 30 minutes during the first intervention and a dropout rate of 15%).
Randomization for the main trial
The randomization list was a computer-generated, complete random-allocation sequence produced by Centre for Evidence-Based Chinese Medicine, Beijing University of Chinese Medicine, Beijing, China. A research coordinator uninvolved with data collection assigned participants and informed acupuncturists of the assignment by telephone.
Blinding for the main trial
Participants were unaware of treatment assignment. Only the acupuncturists knew the allocation but were separated from other research personnel and maintained neutral communications with each participant to avoid providing cues that might reveal which point was inserted.
Researchers for the main trial
TCM pattern diagnosis was made by 10 data collection researchers with 5 years of full-time training in TCM universities and 2–4 years clinical experience. Treatments were performed by 10 licensed therapists with more than 6 years experience. Two (2) supervisors (each monitoring three hospitals) monitored execution of the protocols throughout the study. All the data collection researchers and therapists were trained by 1 of the 2 supervisors, a professor with more than 20 years clinical experience, to increase their comfort (mainly related to accuracy, conforming to the standard and unified practice), and received handbooks of detailed study protocols and standard operation procedures of the main trial.
Outcome measures
In each pattern, demographic and menstrual data were collected at baseline, including age, age of menarche, duration of disease, menstruation, and menstrual cycle. Menstrual pain was measured by 0–100 mm VAS ranging from 0 (no pain) to 100 (worst pain ever) before the intervention, at 5 minutes, 10 minutes, and 30 minutes during the intervention, and at 30 minutes after the completion of this intervention.
Statistic analysis
The aim of this study was to explore whether SP6 was specific for a single TCM pattern so participants with no or overlapping TCM pattern were excluded from analysis.
For participants with only a single TCM pattern, the baseline data were presented as means and standard deviations (SDs) and were tested comparability. In the VAS scores analysis, for each pattern, repeated-measures analysis of variance (ANOVA) was used and the group pairwise comparisons were employed if there was a significant group effect. Mean difference (MD), 95% confidence interval (CI), and corresponding p values as well as means and SDs of each group were presented. Level of significance was set to p<0.05. All analyses were performed using SPSS 17.0 (SPSS Inc., Chicago, IL).
Results
Participants
Of all the 501 participants, 323 participants were diagnosed as single TCM pattern, 168 as overlapping TCM pattern, and 10 were not diagnosed as any one pattern of five mentioned patterns. No participants got a five-patterns diagnosis.
In 323 eligible participants in this study with single TCM pattern, the most common pattern was Cold and Dampness Stagnation pattern (n=184), followed by Qi and Blood Stagnation pattern (n=84) and Qi and Blood Deficiency pattern (n=52). Few participants were diagnosed as Obstruction of Damp-Heat (n=2) pattern or Deficiency of Liver and Kidney (n=1) pattern, so analysis of the former three patterns was done. There were no significant differences of the baseline data among all three groups of all the three analyzed patterns (data shown in Table 1).
SD, standard deviation; y, years; m, months; d, days.
In participants with overlapping TCM pattern, 83.3% (140/168) were identified as two patterns simultaneously, 16.1% as three patterns, and 0.6% as four patterns (data shown in Fig. 1) Moreover, the majority of participants with overlapping patterns were diagnosed as Cold and Dampness Stagnation pattern (91.1% [153/168]), Qi and Blood Stagnation pattern (72.0% [121/168]), and Qi and Blood Deficiency pattern (44.0% [74/168]), which were quite similar to the pattern distribution in eligible participants (data shown in Fig. 2).
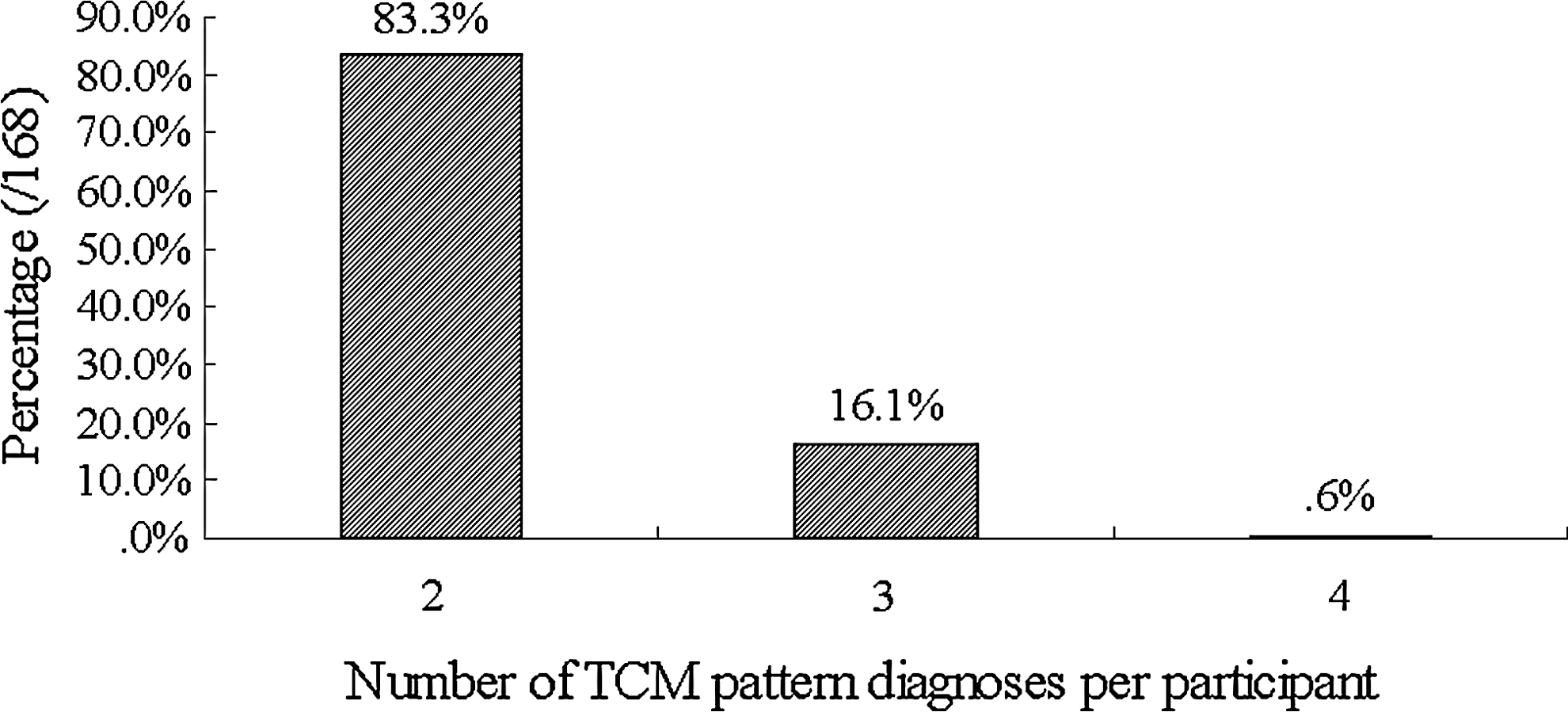
Number of Traditional Chinese Medicine (TCM) patterns per participant in the 168 participants with overlapping TCM patterns.

Distribution of Traditional Chinese Medicine (TCM) patterns in the 168 participants with overlapping TCM pattern diagnoses. Diagnoses: 1, Cold and Dampness Stagnation pattern; 2, Qi and Blood Stagnation pattern; 3, Qi and Blood Deficiency pattern; 4, Obstruction of Damp–Heat pattern; 5, Deficiency of Liver and Kidney pattern.
VAS scores
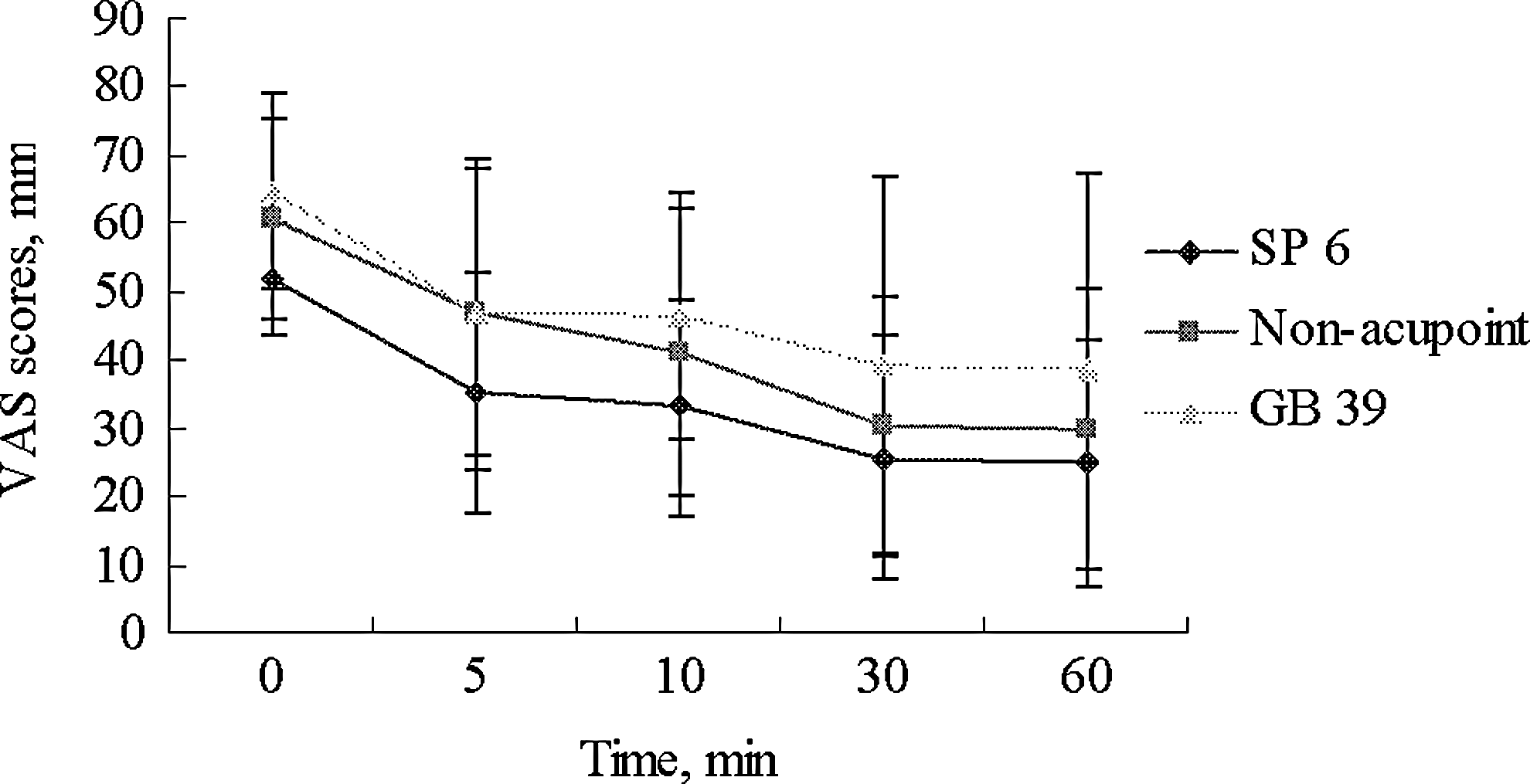
In Cold and Dampness Stagnation pattern, for VAS scores throughout the 1-hour monitoring period, the repeated-measures ANOVA showed significant effects of time and group and a significant group–time interaction. The SP6 group had a significant reduction in VAS scores at five measurement times compared with the GB39 group (MD −7.6 mm, 95% CI −12.7 mm to −2.6 mm, p=0.003) and the nonacupoint group (MD −8.2 mm, 95% CI −13.5 mm to −2.9 mm, p=0.002), respectively, in group pairwise comparisons. However, there were no significant differences between the GB39 group and the nonacupoint group (MD −0.6 mm, 95% CI −5.5 mm to 4.3 mm, p=0.81), whereas for Qi and Blood Stagnation pattern and Qi and Blood Deficiency pattern, there were significant effects of time without group differences and group–time interactions (data shown in Table 2 and Figs. 3 –5).

Development of the mean visual analogue scale (VAS) scores before the intervention, at 5 minutes, 10 minutes, and 30 minutes during intervention, and at 30 minutes after the completion of this intervention of Cold and Dampness Stagnation pattern. Points: SP 6, Sanyinjiao; GB 39, Xuanzhong.
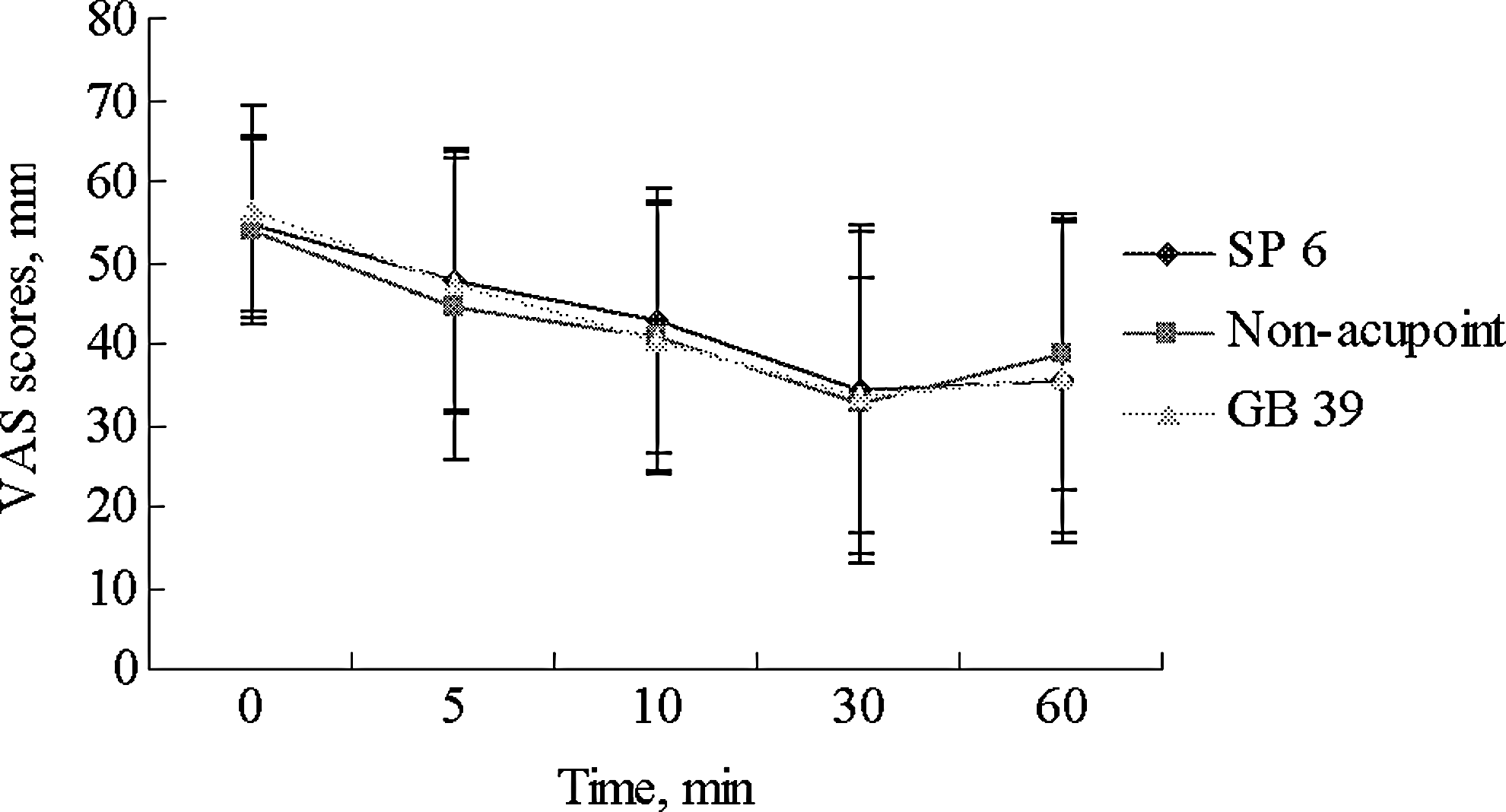
Development of the mean visual analogue scale (VAS) scores before the intervention, at 5 minutes, 10 minutes, and 30 minutes during intervention, and at 30 minutes after the completion of this intervention of Qi and Blood Stagnation pattern. Points: SP 6, Sanyinjiao; GB 39, Xuanzhong.
Development of the mean visual analogue scale (VAS) scores before the intervention, at 5 minutes, 10 minutes, and 30 minutes during intervention, and at 30 minutes after completion of this intervention of Qi and Blood Deficiency pattern. Points: SP 6, Sanyinjiao; GB 39, Xuanzhong.
Discussion
This reanalysis of data sought to examine whether TCM pattern and acupoint-specific effect were related. In comparison to EA at GB39 and the nonacupoint, EA at SP6 significantly reduced VAS scores in Cold and Dampness Stagnation pattern. It suggested that the SP6 was specific for pain relief in PD subjects with this pattern. Furthermore, no group differences in the Qi and Blood Stagnation pattern and Qi and Blood Deficiency pattern implied that TCM pattern differentiation might affect acupoint-specific effect.
The VAS score reductions in the SP6 group were −7.6 mm and −8.2 mm on a 100-mm VAS in comparison to the GB39 group and nonacupoint group, respectively, in Cold and Dampness Stagnation pattern. The group difference resulted from the needling site, since the acupuncture rationale, details of needling (except locations of points used), treatment regimen, practitioners' background, following the STRICTA (STandards for Reporting Interventions in Controlled Trials of Acupuncture) recommendations 30 were identical in the three groups. Besides, the method used in this study was consistent with a recommended method for studying acupoint specificity by a systematic review of acupoint specificity for diseases. 12 Compared with the GB39 and nonacupoint group, the better effect of the SP6 group suggested both the general and the specific effect of SP6 according to International Acupuncture Research Forum (IARF) 2001 recommendations. 31
Nevertheless, the results were not clinically relevant, since a consensus report defined a 10-mm reduction as representing a “minimal” change or “little change.” 32 There might be two reasons. One was limitation of the effect of a single acupoint. The use of several acupoints was commonly used in real clinical practice instead of a single point due to synergistic action. The other reason was both sham treatments with therapeutic effects.
However, to the authors' knowledge, this design was most specifically testing the hypothesis that the TCM pattern had an acupoint-specific effect. Although the use of a prescription was more prevalent in clinical practice, an optimal prescription was not possible since the synergistic action among acupoints had not been clear yet. In addition, understanding the exact specificity of a single acupoint had important significance for prescription research and acupuncture practice. Thus the design of a single acupoint was the better choice for acupoint specificity research. The two control procedures were in accordance with IARF recommendations. 31
These findings were more reliable for two reasons: (1) the main trial from which the data were taken employed rigorous methodology; (2) the diagnosis criteria for TCM patterns were relatively conformed to the national standard in China. However, this study was a reanalysis of the main trial data, and the unequal proportion of each pattern in patients with PD 33 resulted in a small sample size (≤49) 34 in Damp-Heat Obstruction pattern and Liver and Kidney Deficiency pattern, which lowered the findings power.
To further investigate the acupoint-specific effect on TCM pattern, a prospective subdivision design (to recruit participants of a disease, subdivide into TCM patterns, and randomly assign participants of every pattern into treatment and control groups) and power analysis are recommended.
In addition, the TCM pattern differentiation criteria for PD in this report may be improved in three ways: (1) summarizing the distributing rule of TCM syndrome elements (that is, basic elements made up of a pattern, mainly, including location syndrome elements and nature syndrome elements) through literature searches; (2) using a clinical epidemiologic method to analyze the TCM pattern and syndrome element; (3) employing data-mining methods to explore the complicated relationship between the TCM pattern (and syndrome element) and symptoms and signs. 35,36
Conclusions
This article, as a secondary analysis, suggested but did not prove that the TCM pattern had some effect on an acupoint-specific effect and was substantial for an acupuncture trial and clinical practice. The findings also contributed to supporting the choice of SP6 for PD in Cold and Dampness Stagnation pattern and provided evidence from which to build an acupuncture protocol.
Footnotes
Acknowledgments
We sincerely thank the research staff at Dongzhimen Hospital Affiliated to Beijing University of Chinese Medicine (Ji-ping Zhao), China-Japan Friendship Hospital (Shi-liang Li), Beijing Hospital of Traditional Chinese Medicine affiliated to Capital Medical University (Lin-peng Wang), Huguosi Hospital of Traditional Chinese Medicine affiliated to Beijing University of Chinese Medicine (Wei Zhou), The First Hospital affiliated to Tianjin College of Traditional Chinese Medicine (Jing-xian Han), and Shandong University of Traditional Chinese Medicine (Shu-zhong Gao). We also sincerely thank the National Basic Research Program of China (973 Program) (No. 2012CB518506), the National Natural Science Foundation of China (No. 30973793), and the Doctoral Program of Higher Education of Ministry Education of China (No. 20090013110005) for funding this study.
Disclosure Statement
No competing financial interests exist.