
Abstract
Objectives:
This study investigated if nitric oxide (NO) and/or prostaglandin (PG) are responsible for cutaneous vasodilation during warm moxibustion-like thermal stimulation (WMTS).
Design:
For two protocols, two microdialysis membranes were placed in the medial forearm skin. In the first protocol (n=8), the sites were randomly assigned and perfused with NG-nitro-
Settings/location:
The study was conducted in a laboratory at the Kansai University of Health Sciences.
Subjects:
The subjects were 14 healthy male volunteers.
Interventions:
WMTS was applied to the medial forearm skin using an electronic warm moxibustion treatment appliance.
Outcome measures:
SkBF, skin temperature (Tsk), core body temperature (Tc), heart rate (HR), and BP were outcome measures.
Results:
In the first protocol, peak CVC values during WMTS at the site perfused with
Conclusions:
These data demonstrate that NO is involved in the mechanism of cutaneous vasodilation induced by WMTS. Furthermore, increases in CVC despite inhibition of the COX pathway suggest that PG does not contribute to cutaneous vasodilation during WMTS.
Introduction
With respect to the mechanism underlying improvement of local blood flow caused by acupuncture and moxibustion, Jansen et al. 4 reported that local SkBF was increased through the release of vasodilatatory neuropeptides such as calcitonin gene-related peptide (CGRP) or substance P (SP) at an acupuncture stimulation site in anesthetized rats. Noguchi et al. 2 also suggested that the increase in local blood flow caused by acupuncture and moxibustion stimulation occurs because of the release of vasodilatory neuropeptides from afferent nerve endings at the stimulated site. Moreover, Loaiza et al. 5 reported that nitric oxide (NO) was released during electroacupuncture of the quadriceps femoris, resulting in increased local blood flow in knee-joint capsule arterioles in anesthetized rats. Tsuchiya et al. 6 reported that acupuncture increased the NO concentration in plasma from acupunctured arms, compared with that from sham-acupunctured arms in humans. These findings suggest that acupuncture might influence local circulation in the treated area through regulation of NO levels.
Previous research has shown that increased SkBF during heat stress is induced via a neurally mediated active vasodilatory system. 7 Furthermore, NO and prostaglandin (PG) contribute to cutaneous vasodilation during heat stress. 8,9 It may be that similar mechanisms are responsible for the increases in cutaneous vasodilation during warm moxibustion. To the current authors' knowledge, the mechanisms underlying SkBF changes during warm moxibustion have not previously been reported. In normal warm moxibustion, thermal stimulation of the skin is inherently unstable because of the form and properties of the moxa, and quantitative stimulation is difficult to apply. 10,11 Therefore, the present study was performed with warm moxibustion-like thermal stimulation (WMTS) using an electronic warm moxibustion treatment appliance. The objective of the present study was to test the hypothesis that NO and/or PG contribute to cutaneous vasodilation during WMTS.
Materials and Methods
Subjects
Eight (8) men participated in Protocol 1. The mean (±standard error of the mean [SEM]) age, height and weight were 26.8±2.3 years, 169.9±2.0 cm, and 75.6±5.5 kg, respectively. Six (6) men participated in Protocol 2. The mean (±standard error of the mean [SEM)]) age, height, and weight were 28.6±2.2 years, 168.6±1.8 cm, and 67.8±4.1 kg, respectively. All subjects were healthy, normotensive, and nonsmokers. Each subject was informed of the purposes and risks of the study before providing written consent. The institutional review board of Kansai University of Health Sciences approved all protocols and informed consent documents in accordance with the ethical standards established in the 1964 Declaration of Helsinki.
Instrumentation and measurements
Upon entering the laboratory, each subject rested in a supine position during placement of two intradermal microdialysis probes in the dermal space of the medial aspect of the left forearm. The two microdialysis sites were placed at least 6 cm apart. The membrane window for each probe was 10 mm. For placement of the probes, a 25-gauge needle was used to pierce the dermal space without local anesthesia, exiting 20–25 mm from the point of entry. The microdialysis probe was threaded through the lumen of the needle, and the needle was then removed, leaving the probe in place. After membrane placement, the microdialysis probes were taped in place, and Ringer's solution was perfused through the fibers at a rate of 2 μL/minute, using an infusion pump (Pump 11, Harvard Apparatus, Natick, MA; Fig. 1A). Two stimulus probes (external diameter, 40 mm; internal diameter, 6 mm) of a clinical electronic warm moxibustion treatment appliance (CS-2000, Kanaken, Yokohama, Japan) were positioned over each microdialysis membrane (Fig. 1B). The warm moxibustion treatment appliance reproduces the temperature curve of traditional moxibustion. The heating element comprises a chrome-plated copper sheet that transmits far infrared waves to the skin. Highly sensitive sensors are incorporated into the heat-generating component to improve the responsiveness of temperature control. In a preliminary study, skin temperature (Tsk) was unchanged at a site 2 cm from the stimulus probe. Thus, stimulus probes were placed ≥ 2 cm apart. WMTS was performed by placing the stimulus probe on the skin, with a heating temperature of 41°C (heating 15 seconds, rest 15 seconds). Markings on the polyimide tubing that indicated the center of the membrane portion of the microdialysis probe were used to facilitate accurate placement of the stimulus probes. Each stimulus probe housed a laser-Doppler flow probe (model OP, ALF-21D; ADVANCE, Tokyo, Japan) such that SkBF was assessed from the same location directly over the microdialysis membrane (Fig. 1A). Thermocouples were placed between the skin and stimulus probes to monitor local Tsk. Heart rate (HR) was obtained from the R–R interval of the electrocardiogram (ECG) and arterial pressure was measured manually by auscultation. The mean arterial pressure (MAP) was calculated from the diastolic BP (DBP) and systolic BP (SBP) as MAP=DBP+(SBP-DBP)/3. An oral thermistor was also used to measure oral temperature (under the tongue) for each subject throughout the experimental period as an index of core body temperature (Tc).

Protocol 1
Protocol 1 examined if cutaneous vasodilation in response to WMTS would be attenuated by NO synthase (NOS) inhibition. After allowing at least 90 minutes for the hyperemic response associated with membrane placement
12
to subside, one microdialysis probe was perfused with 20 mM of N
G-nitro-
Protocol 2
This protocol was designed to test whether cutaneous vasodilation to WMTS would be altered by cyclo-oxygenase (COX) inhibition. Two microdialysis membranes were placed in medial forearm skin as described for Protocol 1. One site was perfused with 10 mM of ketorolac (Keto) dissolved in Ringer's solution at a perfusion rate of 2 μL/minute, a nonselective COX-1/COX-2 inhibitor meant to block the production of PGs. The dose of Keto was based on prior studies in which successful blockade of PG synthesis was achieved in human skin. 8,16 The second microdialysis probe (control site) was perfused with Ringer's solution. The experimental setup was identical to that of Protocol 1. All other parameters were recorded in the same manner as in Protocol 1.
Data analysis
Data were continuously obtained and digitized at a sampling rate of 50 Hz (Power Lab 8/30; AD Instruments, Sydney, Australia). Data from Protocols 1 and 2 were averaged at 2-minute intervals for analysis. Cutaneous vascular conductance (CVC) was calculated from the ratio of SkBF to MAP. For both protocols, a repeated measures two-way analysis of variance (ANOVA) was used to detect differences in CVC between drug-treatment sites. For the two-way ANOVA, Tukey's posthoc analysis was used. Peak CVC values were compared between drug-treatment sites to the normothermic baseline or during WMTS, using a paired Student's t-test. Values were the mean±SEM. The significance of difference was accepted at p<0.05.
Results
Protocol 1
At the initiation of heating, Tsk at the heating probe–skin surface interface increased from 34.0°C (baseline period) to 41.0°C and remained stable throughout the WMTS application. None of the subjects reported feeling any sensation of pain during WMTS at either site. Average Tc, HR, and MAP remained unchanged throughout the protocol. Figure 2 shows CVC responses to WMTS when

Effect of nitric oxide synthase inhibition (with N
G-nitro-
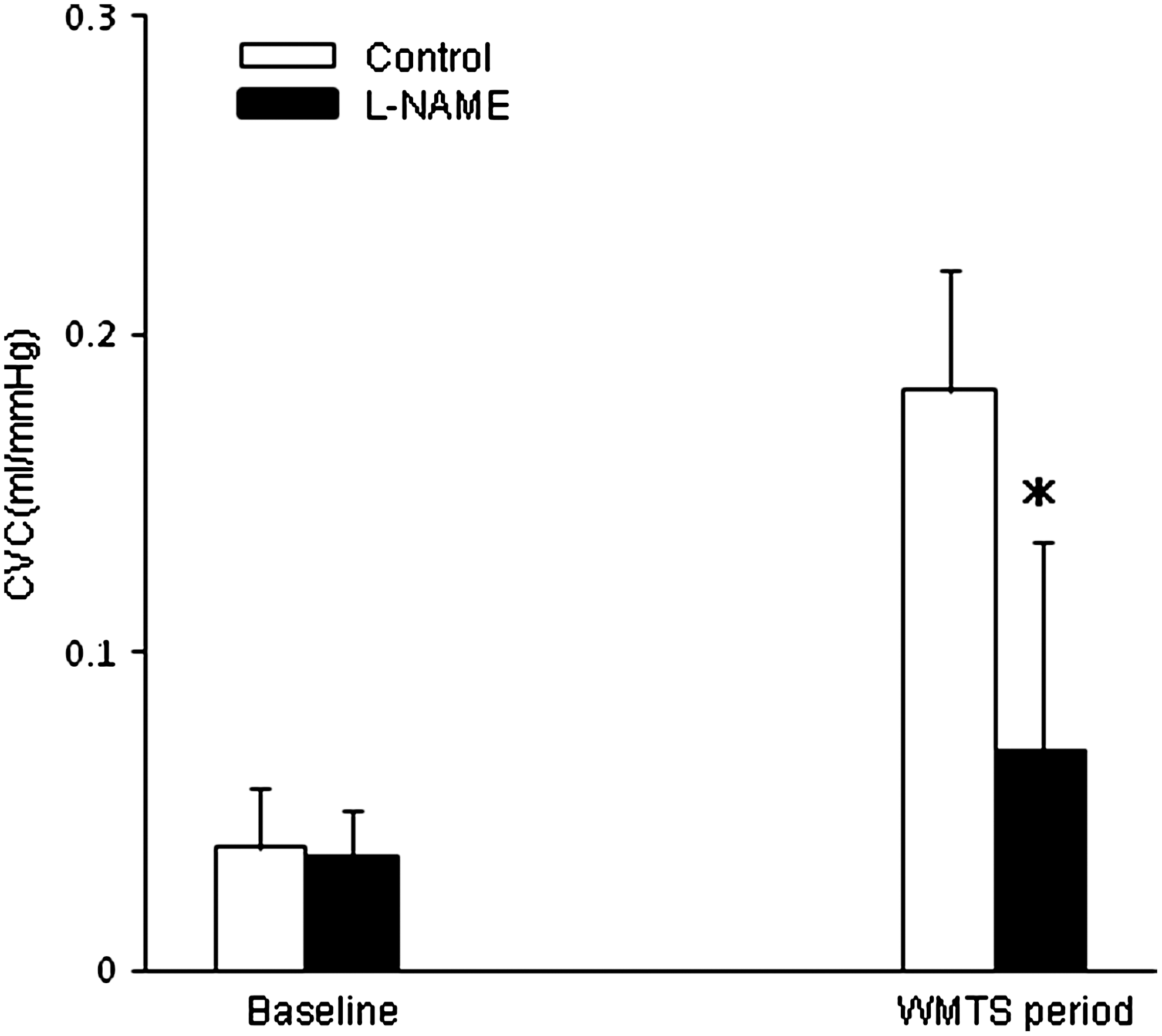
Peak cutaneous vascular conductance (CVC) values at thermoneutral baseline and during warm moxibustion-like thermal stimulation (WMTS) at control and nitric oxide synthase-inhibited (with N
G-nitro-
Protocol 2
As in Protocol 1, mean Tc, HR and MAP remained unchanged throughout the protocol.
Table 1 summarizes mean cardiovascular and thermal data from Protocols 1 and 2 during the baseline and WMTS periods. HR, BP, Tsk, and oral temperature recorded in Protocol 2 did not differ significantly from those monitored during the corresponding periods of Protocol 1. CVC did not differ between the two microdialysis sites (p>0.05, Fig. 4). There was no significant difference between CVC response in Keto (0.06±0.02 mL/mmHg) and control sites (0.05±0.02 mL/mmHg) during baseline measurements (p>0.05, Fig. 5). In addition, there was no significant difference between peak CVC values in Keto (0.22±0.04 mL/mmHg) and control sites (0.23±0.05 mL/mmHg) during WMTS (p>0.05; Fig. 5).
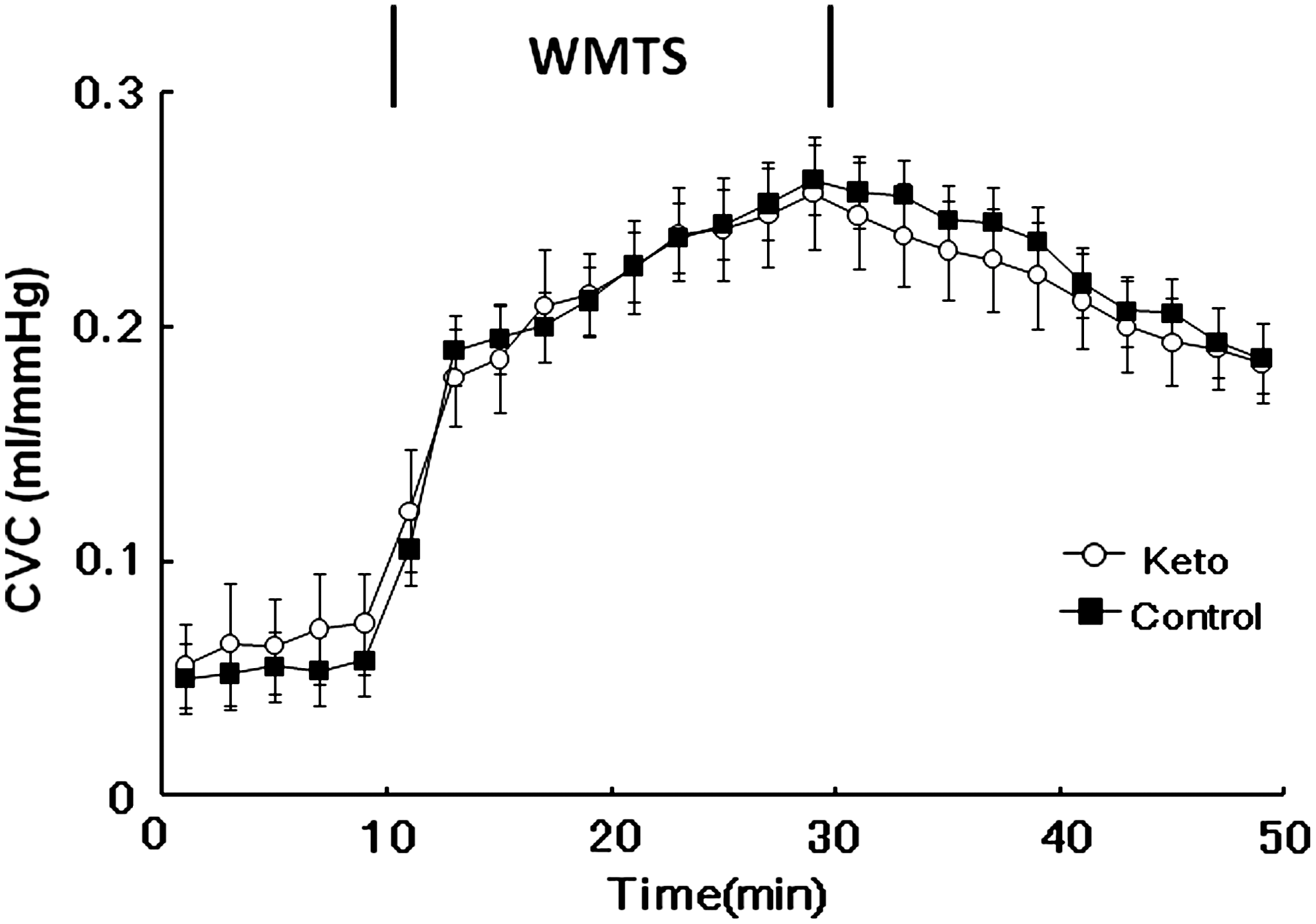
Effect of cyclo-oxygenase inhibition (with ketorolac [Keto]) on cutaneous vascular conductance (CVC) during warm moxibustion-like thermal stimulation (WMTS). CVC did not significant differ between Keto and control sites (p>0.05). Values are mean±standard error of the mean.
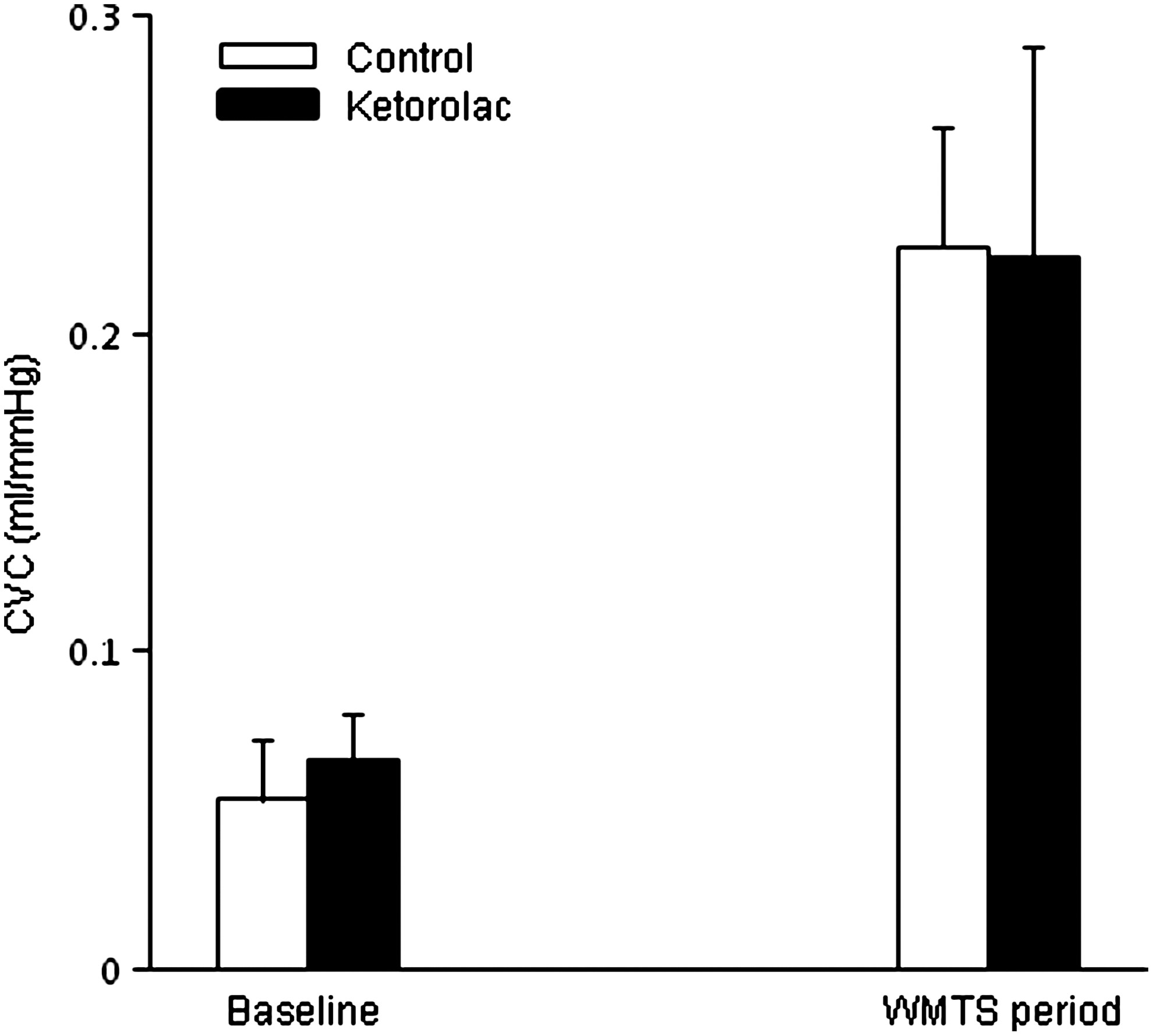
Peak cutaneous vascular conductance (CVC) values at thermoneutral baseline and during warm moxibustion-like thermal stimulation (WMTS) for control and cyclo-oxygenase–inhibited (with ketorolac [Keto]) sites. There were no differences in peak CVC values between Keto-treated and control sites at thermoneutral baseline or during WMTS. Values are mean±standard error of the mean.
Values are mean±standard error of the mean. HR, MAP, oral temperature, distal Tsk and proximal Tsk did not differ significantly between the corresponding periods of Protocal 1 (P1) and Protocol 2 (P2) for baseline values for warm moxibustion-like thermal stimulation).
HR, heart rate; bpm, beats/minute; MAP, mean arterial blood pressure; Tsk, skin temperature, NS, not significant.
Discussion
The primary finding of the present study is that WMTS provoked cutaneous vasodilation in human skin by mechanisms that involve NO production. This finding is based on the observation that inhibition of NOS production of NO by
Warm moxibustion is widely used clinically; however, the exact mechanism by which SkBF increases during warm moxibustion is unknown. The increase in SkBF during WMTS indicates that WMTS increases circulation in treated regions. Moreover,
Regarding changes in local blood flow caused by acupuncture and moxibustion stimulation, a previous study by Jansen et al., 4 using anesthetized rats, found that electroacupuncture to a dermal flap caused an increased cutaneous blood-flow response similar to that occurring with administration of SP or CGRP. This suggests that either SP or CGRP is involved in the increased cutaneous blood-flow response at sites stimulated by electroacupuncture. Sato et al. 17 reported that, in anesthetized rats, an increased blood-flow response occurred not only in the skin but also in skeletal muscle, and that the disappearance of this response with the administration of CGRP receptor blockers suggests the involvement of CGRP. Noguchi et al. 2 recently reported that the local muscle blood-flow increase in response to moxibustion stimulation lasted a few minutes, and that this response was induced via an axon reflexlike response that involves CGRP. These studies suggest that the blood-flow increase in response to acupuncture and moxibustion is induced through an axon reflex, and that CGRP is implicated in this process.
Attention has also been directed in recent years to the involvement of NO released from vascular endothelial cells in the cutaneous vasodilation response to acupuncture stimulation. NO is clearly an important element in neurogenic vasodilation in the skin.
18,19
Loaiza et al.
5
reported that NO is involved in the increase in local blood flow caused by electroacupuncture applied for 30 minutes. Higher NOS activity has been found at meridians and acupoints, compared to other cutaneous regions in rats.
20
Li et al.
21
reported an increase in blood NO levels after warm needling. Furthermore, Tsuchiya et al.
6
demonstrated a significant correlation between the increase in blood flow and the increase in NO level in human arms receiving acupuncture. These findings suggest that acupuncture stimulation might increase local blood flow via an increase in NO. Data from the present study are consistent with these findings with respect to the effects of NOS inhibition on the cutaneous vasodilator responses during WMTS. However, in the present study, NOS inhibition by
It has been reported that PGs contribute to cutaneous vasodilation during heat stress induced cutaneous vasodilation. 8,16 Both NO and PG have been reported to contribute to cutaneous vasodilation during exogenous administration of acetylcholine. 13 Sympathetic cholinergic nerves recognized to induce cutaneous vasodilation during heat stress release acetylcholine as well as other cotransmitters. 22 Given these observations, if cutaneous vasodilation during WMTS is induced by the sympathetic cholinergic system, then one may likewise expect an NO and PG component mediating vasodilation during WMTS. However, the absence of an effect of COX inhibition on vasodilation during WMTS raises the possibility of different mechanisms of cutaneous vasodilation relative to that which occurs during heat stress.
Finally, none of the participants in this study reported feeling pain during WMTS, and neither HR nor BP increased during WMTS in this study. Regarding this, Noguchi et al. 2 reported that local blood-flow response at the moxibustion stimulation site does not depend on BP change in anesthetized rats, because moxibustion stimulation does not cause any change in systemic BP. Uchida et al. 3 also observed that there was no significant increase in BP during moxibustion stimulation in anesthetized rats. Similarly, the SkBF increase in response to WMTS in this study is considered to represent a localized response at the stimulated site that is not dependent on a blood pressure response.
Conclusions
The present study demonstrated that blockade of NOS with
Footnotes
Acknowledgments
The authors are grateful to the subjects for their participation in this study.
Disclosure Statement
The authors declare that they have no conflicts of interest related to this article.