
Abstract
Objective:
The goal was to review systematically the comparative effectiveness of yoga, compared with other exercise interventions, for older adults as shown on measures of health and physical functioning.
Design:
This was a systematic review with both narrative synthesis and meta-analysis.
Data sources:
Searches were conducted in MEDLINE®/PUBMED, PSYCINFO, CINAHL, Web of Science, and SCOPUS; bibliographies of selected articles; and one systematic review on the effects of yoga on cardiovascular disease.
Methods:
Original studies from 1950 to November 2010 were sought, evaluating the effects of yoga on older adults. The search was restricted to randomized controlled trials of yoga in subjects ≥age 60, and published in English. Data were extracted and evaluated regarding setting, population size and characteristics, intervention type and duration, comparison group, outcome assessment, data analysis, follow-up, key results, and the quality of each study according to specific predetermined criteria.
Results:
The search yielded 18 eligible studies (N=649). The studies reported on older adults across a range of settings, intervention intensity, and outcome measures. The majority of the studies had<35 participants (range 9–77). Quantitative and qualitative synthesis of the studies suggested that the benefits of yoga may exceed those of conventional exercise interventions for self-rated health status, aerobic fitness, and strength. However, the effect sizes were modest, and the evidence was mixed for yoga's effect on depression, sleep, and bone-mineral density. Studies did not find an effect on cognition.
Conclusions:
Small studies with mixed methodological quality suggested that yoga may be superior to conventional physical-activity interventions in elderly people. The precision of the estimates remains low. Larger studies are necessary to define better the intersection of populations, settings, and interventions in which yoga is most beneficial.
Introduction
Yoga is a potentially promising physical activity for older adults. 9 –14 Surveys show that many older adults in the United States are practicing yoga. 9,11,15 Many forms of yoga exist—such as Hatha, Iyengar, and other yoga forms—that aim to promote overall movement, health, and wellness. 10 Iyengar yoga is a form of yoga that uses props such as bolsters, belts and chairs to adapt to an older individual's abilities. 13,16,17
Yoga not only improves health-related quality of life (HRQoL) 18,19 but also enhances walking and balance, 8,16,17,20 muscle strength, 20 –22 cardiovascular health, 23 –25 blood pressure (BP), 23,25 –27 sleep, 12,28 and functioning of other systems. 29 –38 Yoga may also have psychosocial benefits through prevention and control of common health and emotional problems linked with aging. 19,39,40 An emerging evidence base describes the effectiveness of yoga for psychosocial and physical functioning in older adults. 18 The current authors performed a systematic review to compare effectiveness of yoga with other exercises for promoting physical performance and quality of life (QoL). Previous systematic reviews have looked at the effects of yoga in young adults; is effects on patients with insulin resistance syndrome and cardiovascular disease, 24 anxiety, 40 and chronic pain 41 ; and yoga's therapeutic effects on children. 42 None of these reviews have addressed the effects of yoga in older adults.
This systematic review was framed around the following question: Among older adults in community and institutional settings, is yoga superior to other physical activity with respect to its effect on physical functioning measures and health related quality of life (HRQoL)?
Methods
Data Sources and searches
Astandardized protocol was developed and followed for all steps of this review (Appendix 1). Two (2) investigators searched databases to include MEDLINE®/PubMed, PsycInfo, CINAHL, Scopus, and Web of Science; these searches were augmented by hand-searching bibliographies of selected articles and a previous systematic review of yoga and cardiovascular disease on older adults. The search terms included
Study selection
Two (2) investigators independently reviewed the titles, abstracts and/or full-text of manuscripts of retrieved articles to determine if they met eligibility criteria. The inclusion criteria were: (1) randomized controlled trials; (2) participants 60 and older, (3) yoga, compared to another intervention; and (4) English. To evaluate potential subgroup effects, all eligible studies were included regardless of dwelling. There were no restrictions on year of study. Consensus among the investigators occurred through additional review of the original reports (Fig. 1). In one case, the study was excluded because the study design was unclear. 43
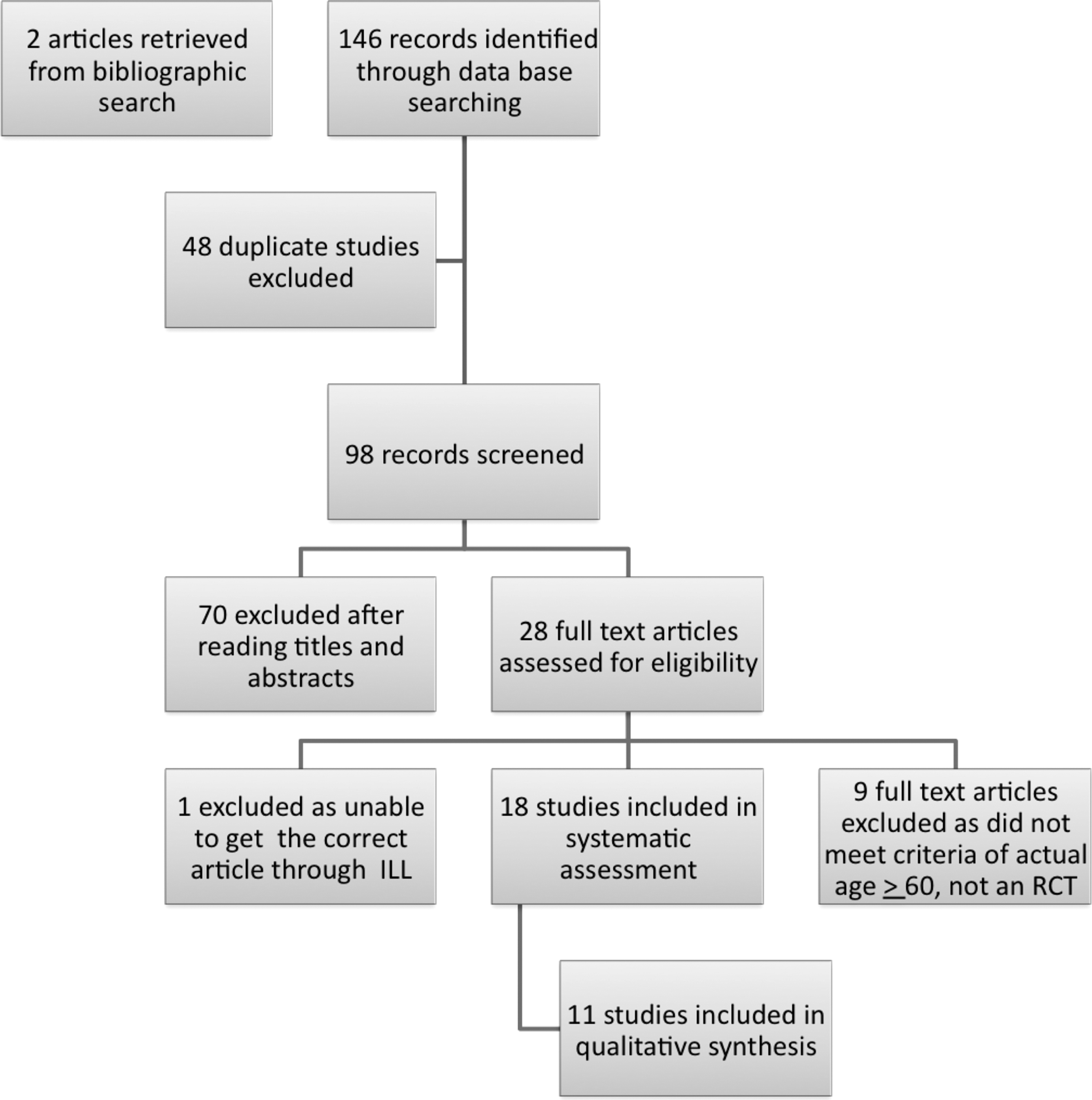
Flow diagram showing the identification, screening, eligibility and those included for the systematic review.
Data abstraction
Two (2) investigators independently abstracted data, using a standardized form that was developed after a series of pilot abstractions and then was verified by a third reviewer. The abstracted data included author/year, database, age range, mean age, % male, sampling strategy, inclusion criteria, exclusion criteria, comorbid conditions, source of participant accrual, overall sample size and numbers in intervention and control groups, type of yoga (description, dose, duration of intervention), if outcome assessment was blinded, outcomes assessed, participant attrition, adverse effects, statistical analysis, conclusions, funding sources, and indicators of study quality.
Quality assessment
A methodological quality assessment (Table 1) was performed to evaluate sources of systematic bias. 44 Ten items used for quality assessment included: (1) source of patients; (2) number of controls; (3) selection description; (4) withdrawals; (5) therapeutic regimens described; (6) prior estimate of sample size; (7) statistical inference; (8) appropriate statistical analysis; (9) handling of withdrawals; and (10) side-effects. Rather than use a summary score of study quality, the effect of key quality measures on study outcomes was evaluated.
AE, aerobic exercise; BMI, body mass index; BP, blood pressure; CES-D, Clinical Epidemiological Scale – Depression; CHD or CAD, coronary heart disease or coronary artery disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CVA, cerebral vascular accident; FBS, fasting blood glucose; HDL, high density lipoprotein; HR, heart rate; HRQOL, health related quality of life; HTN, hypertension; LDL, low density lipoprotein; MFI – Multidimensional Fatigue Inventory; OA, Osteoarthritis; POMS, Profile of Mood States; MOS SF-36, Medical Outcomes Study SF-36; STAI, State Trait Anxiety Index; T2DM, type 2 diabetes mellitus; VLDL, very low density lipoprotein; VO2, maximal oxygen consumption.
Data synthesis and analysis
Data were synthesized descriptively, emphasizing methodological characteristics of the studies, such as populations enrolled, definitions of selection and outcome criteria, sample sizes, adequacy of the randomization process, interventions and comparisons, outcome assessment or intervention administration, subjective versus objective measures, and study quality. In addition, a meta-analysis was performed for selected outcomes when they were similarly measured across studies.
Comparisons of yoga and other exercise interventions were based on absolute differences in continuous measures of physical functioning, QoL, or depressive symptoms. The summary measure in this meta-analyses was the standardized mean difference (SMD). The SMD is an effect-size measure computed by dividing the mean difference in outcomes between groups by the pooled standard deviation (SD) of the outcome. Standard cutoffs were used to interpret the effect sizes: 0.6 for modest effect size and 0.8 for large effect size. To evaluate heterogeneity among studies in the meta-analyses, the I 2 statistic, which measures the proportion of variability among studies that cannot be explained by chance, was used. The I 2 statistic ranges from 0% to 100% with values closer to 0 representing less heterogeneity. Typically 25%, 50%, and 75% are used to respectively define low, moderate, and high heterogeneity.
Because the included studies were small, there were imbalances in baseline scores after randomization, so it was not possible to compare outcomes at the endpoint. Change scores for each study arm were therefore computed and compared. Change scores were calculated from baseline and endpoint measures in the studies' data tables. Because none of the studies reported the SDs of the change scores, a procedure in the Cochrane Handbook (Section 16.1.3.2) 45 was used to impute these SDs. A sensitivity analysis was used to how the imputations affected the statistical significance of meta-analytical summary estimates. The results presented here represent the most conservative imputations. Meta-analyses were performed using Stata Version 11.0 (StataCorp, College Station, TX).
Results
Search results and study characteristics
A total of 146 articles, titles and abstracts were retrieved via the search (Fig. 1). Of these, 48 articles were excluded as duplicates; 70 were excluded after determining that their titles and abstracts were not relevant or did not meet inclusion criteria; 9 were excluded after full-article review as not meeting inclusion criteria; and 19 articles met eligibility criteria. It was not possible to retrieve 1 eligible article as a full text. 34 Thus, 18 articles were included in the systematic review. The 18 studies included 11 unique cohorts of participants, as 7 of the articles reported on different outcomes variables for cohorts previously described in other articles. The 11 cohorts thus represented the sample for the qualitative analysis of the various outcomes (Fig. 1).
The mean age of participants across the studies ranged from 63.5 to 77.5, and the majority (71%) were women (Table 2). The included studies represented four different countries—the United States, 19,23,26,32,36,46 –49 Cuba, 31 Taiwan, 12,20 and India. 28,33 Thirteen (13) studies were conducted in community settings, 19,23,26,29 –32,36,45 –49 4 studies were in institutional/residential or senior communities, 12,20,28,33 and 4 studies reported on stable patients from the community with either chronic obstructive pulmonary disease (COPD) or coronary heart disease (CHD) or diabetes. 30,31,46,47 Ten (10) studies were designed to evaluate yoga as the primary intervention, 12,19,20,28,30 –33,36,49 whereas 8 studies were designed with aerobic exercise as the primary intervention and yoga as the active control. 23,26,29,36,46 –48,50 The yoga intervention varied in frequency from once to twice a week, for 12 weeks to 14 months. The studies assessed various primary outcomes, maximum aerobic capacity (VO2 max), 23,26,36,50 depression, 12,19,23,33 sleep, 12,19,28 measures of cognition, 19,50 HRQoL, 12,19,31,32 upper- and lower-extremity strength BP, total cholesterol, body mass index (BMI), 19,20,23,26,30,31,46,48 bone density, 32,46 –48 dyspnea intensity, 30 and kyphosis. 32
Methodological quality of studies ranged from 6 to 9 of the quality elements present (Table 1). Half of the studies had well-defined inclusion and exclusion criteria. Only one study determined sample size a priori, 19 and another study 32 reported that outcome assessors were blinded. The intervention and control groups were well-described. There was poor reporting on allocation concealment. Baseline imbalances were evident between study arms for different HRQoL outcomes. 19,30,46,47 Presence or absence of adverse events was not reported by most of the cohorts (7 of 11).
Narrative Summary
Physical functioning, exercise, and yoga
Substantial improvements were reported on household activities, such as floor sweeping, vacuuming, laundry loading/unloading, and bed making in both the resistance training and yoga groups with no significant difference between groups. 47 Oken et al. 19 demonstrated that the yoga group had improvements in physical measures such as timed one leg standing and forward flexibility as well as QoL measures related to sense of well-being, energy, and fatigue, compared to an aerobic exercise control group. The effects on kyphosis were evaluated by Greendale et al., 32 who found that the yoga group experienced a 4.4% improvement in flexicurve kyphosis angle and 5% improvement in kyphosis index, compared with the monthly luncheon groups that served as controls.
Physiologic measures and yoga
There were no significant changes in body weight, BMI, % body fat, fat-free mass, appendicular muscle mass, or bone mineral density (BMD) for either the resistance training or the yoga group. 46 The resistance-training group increased in leg and arm strength as measured by a single repetition maximal (1RM). 46 Blumenthal et al. 26 confirmed that older adults had little objective improvement in physical strength. An increase in bone density occurred in men after 14 months of participation in both the exercise and yoga programs, but no change was found for women. 48 Body flexibility had significantly improved in both the upper and lower body in the yoga group, with improved lower-limb muscle endurance and walking speed, but there were no significant changes in body weight or BMI. 20
Ades et al. 26 and Blumenthal et al. 46 found that dyspnea-related distress and heart rate were decreased at the end of a 6-minute walk test in the yoga group, but there were no significant changes in pulmonary function as measured by forced expiratory volume at 1 minute (FEV1) and forced vital capacity (FVC).
The concentrations of fasting blood glucose and cholesterol decreased for older adults with diabetes in the yoga and exercise groups. 31 Lipid peroxidation, as indicated by malondialdehyde, decreased significantly in the Hatha yoga and the physical training groups. There was no significant difference from baseline to 6 months in protein oxidation. 31
Psychosocial measures and yoga
Yoga was compared with control or wait-list control groups for cognition (N=142), 19,50 however, no differences were found after yoga training (n=74), compared with a control group (n=68). No changes in cognition, as measured using the Wechsler Adult Intelligence Scale—Digit symbol and vocabulary test, were reported to be related to aerobic exercise or yoga. 50 Nor were there effects of yoga on cognition, as demonstrated by subjects using the Wide Range Achievement Test. 19 Similarly, no changes were found for alertness and attention, as measured by the Stroop color and word testing.
A significant decrease in sleep latency and increase in number of hours slept were found after 6 months of yoga intervention. 28 Sleep outcomes, using the Pittsburgh Sleep Quality Index (PQSI), and depression, using the Taiwanese Depression Scale, were reported after 6 months of yoga decreased sleep latency, daytime dysfunction and depression decreased, while subjective sleep quality, physical health perception, and mental health perception improved. 12 Subjective scales—the Stanford sleepiness scale and Profile of Mood States—used to measure sleep and mood, showed no change among groups. 19
Sleep and depression (N=286) were evaluated by three researchers, using a subjective assessment or a questionnaire to determine sleep quality. 12,19,28 None of the differences were statistically significant; however, the change scores may have been clinically meaningful as reported by Manjunath 28 (N=23), Chen, 12 (N=128), and Oken 19 (N=135). In contrast, depression, measured with the Geriatric Depression Scale (GDS), 15 was reduced in a yoga group at 3 and 6 months. 33 In older adults with COPD, however, there were no significant changes in depressive symptoms, anxiety, or general disease-specific HRQoL. 30
Adherence to yoga
Flegal et al. 49 correlated adherence to yoga with baseline measures of depression, fatigue, and physical components of HRQoL. These researchers reported that adherence was not related to age, gender, or educational level.
Meta-Analysis
We performed a meta-analysis for selected outcomes for reports with similar outcome measures: (1) VO2max; (2) depression (Center for Epidemiological Studies—Depression Scale (CES_D) and GDS); and (3) HRQOL (both physical and mental scales; (Fig. 2A–D).
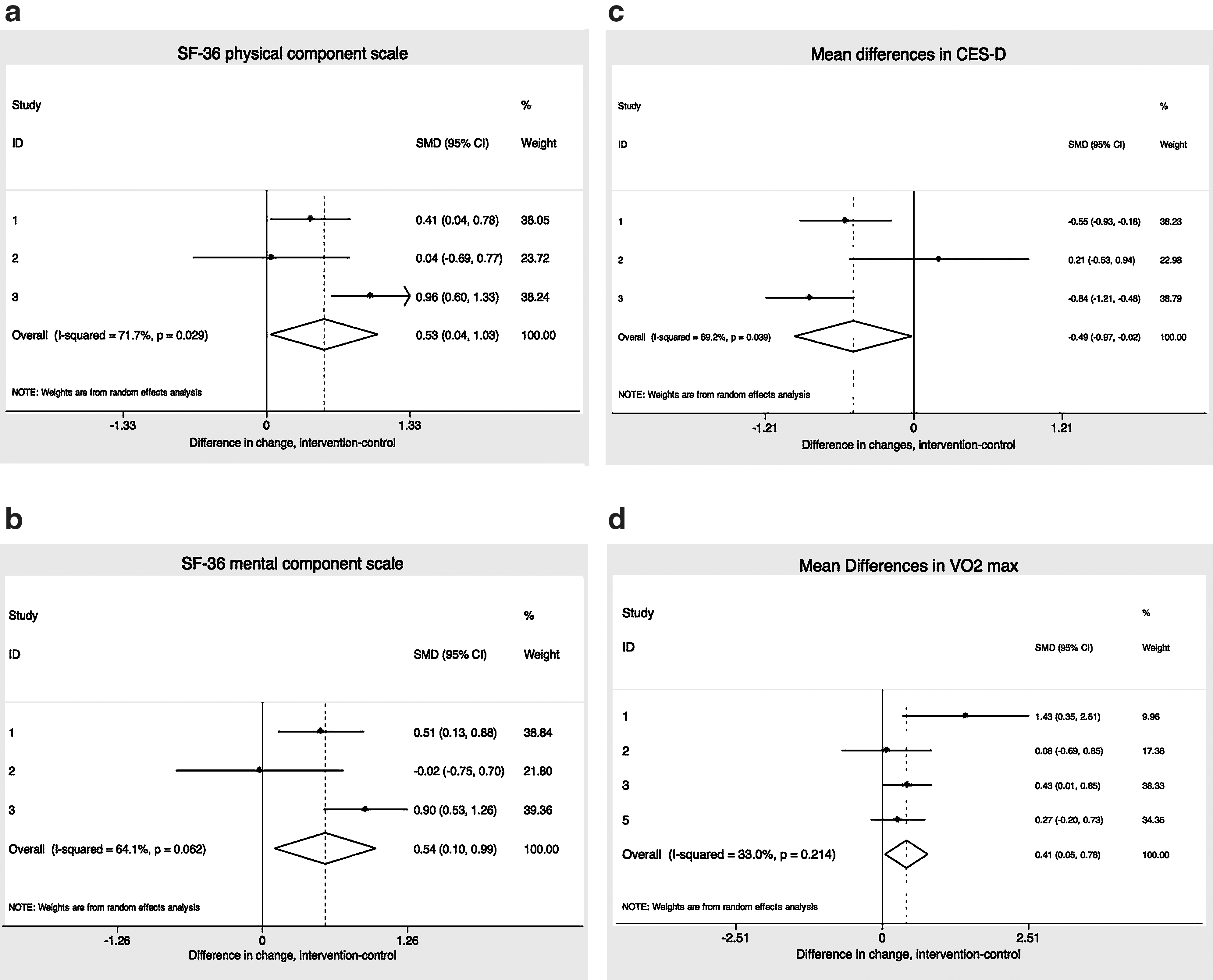
Showing the forest plots of the primary outcomes of the included studies.
Maximal aerobic consumption capacity (VO2max; Fig. 2A; N=282) was measured in several studies using aerobic exercise (AE), compared with a control group who performed yoga. 26,29,46,50 The summary standardized mean difference for VO2max was 0.54 (0.08–1.00), which was a moderate effect size favoring yoga over comparison activities. Heterogeneity among studies was modest.
Depression (Figure 2B; N=543), as measured by the CES-D (3 of 4 researchers) 12,19,30 or the GDS (1 of 4 researchers) 33 did not change in any of the 4 studies abstracted (exercise [n=99] versus yoga [n=173] versus control [n=162])].
The SMD for depression was −0.57 (−1.17 to 0.04), which was a moderate effect size in the direction of yoga reducing depression scores to a greater extent than comparison activities did, although this reduction was not statistically significant. Study heterogeneity was large (I 2 80%).
HRQoL was evaluated separately for the Short Form–36 (SF-36) physical and mental component scales (Fig. 2C and D; N=422). 12,19,30, 33 On the physical component scale of the SF-36, the estimated SMD (0.65 [0.02–1.28]) favored the yoga intervention. Study heterogeneity was large (I 2 82%). On the mental component scale of the SF-36, the estimated SMD again favored yoga (0.66 [0.10–1.22]). Study heterogeneity was large (I 2 77%). These effect sizes for the SF-36 mental and physical scales are classified as moderate.
Discussion
The current systematic review suggests that yoga may be superior to aerobic exercise interventions to improve self-rated physical and mental health status (measured by SF-36), flexibility, and aerobic fitness (measured by VO2max). Mixed evidence was found for strength, BMD, sleep and depression. Cognitive function did not seem to improve after yoga intervention.
Consistent with a field in its early stages of development, the findings are based on a relatively small number of trials with little statistical precision and significant methodological weaknesses. Innes et al. 24 reported limitations in the yoga studies and methodological quality of the studies such as limited numbers of participants, lack of reporting of adverse effects, and no sample size justification. Other systematic reviews showed promising results but had similar limitations with studies and the methodological quality. 40,42,51
The current review indicated several limitations in the available evidence base. First, there was wide variability in the interventions. Many different types of yoga regimens were prescribed. The diversity in yoga intervention was not surprising, as there are many different types of yoga practiced based on each teacher's training and philosophy. The duration of intervention and frequency of intervention also varied widely among the various trials, as did the study outcomes and measurement methods. Second, poor adverse-event (AE) reporting in most of the studies limited any conclusions about the safety of yoga as an exercise. It was unclear if there was lack of reporting of adverse effects or no actual AEs occurred. Third, sample sizes were small, which limited the precision and generalizability of the estimates. Fourth, the interventions' durations varied considerably across studies.
The current authors recommend that researchers design clinical trials with well-specified yoga interventions that take into account the differences in approaches based on training and philosophy. The yoga intervention for any study should be described in more detail, in terms of frequency, intensity, and the duration of sessions to allow for determination of exercise dose–response. Investigators should specify clinically meaningful effect sizes. Future trials should formally monitor and report the incidence of AEs and reasons for dropouts, such as musculoskeletal injuries. Standardized, objective measurements of physical, psychosocial, and spiritual well-being are recommended, such as self-reports of pain (visual analogue scale), quality of life (SF-36) and sleep (questionnaire), and objective measures of functional ability (Short Physical Performance Battery), function (walking speed), balance (single-limb stance), flexibility (functional reach or sit and reach), and muscle strength (sit to stand and hand grip). These outcome measures are recommended based on the importance of early identification of people at risk for decline in function and frailty. 2,52,53 Given the low number of participants, it is important to assess barriers to participation. The current authors recommend that future research focus on assessing barriers, perceived benefits, and cues to action for participation in, and adherence to, yoga exercise regimens in addition to exploring ways of recruiting and retaining participants. For example, one of the reasons for low participation may have been the religious beliefs of the participants. 54
Conclusions
In summary 18 studies (11 cohorts) were systematically reviewed. The outcomes studied were diverse, thereby limiting a meta-analysis of all the studies. Limited evidence supports yoga's benefit for strength, flexibility, physical and mental health status, and aerobic fitness. Its effect on other important outcomes—household functioning, depression, sleep, and others—remains uncertain. Very little has been reported about potential adverse events. Overall, the current authors recommend yoga for older adults with careful observation and monitoring of side-effects.
Footnotes
Acknowledgments
This work was supported by the Department of Health and Human Services (D01 HP08795), Health Resources and Services Administration, Bureau of Health Professions, and The John A. Hartford Foundation Center for Excellence in Geriatrics Education. The authors wish to thank Michael L. Parchman MD, MPH and Valerie A. Lawrence MD, MSc for their contributions to the development of this article. This study would not have been possible without the support of the Department of Family and Community Medicine, University of Texas Health Science Center at San Antonio, Texas.
Disclosure Statement
No conflicts of interest exist.
Appendix