
Abstract
Objectives:
This article reports on a case and reviews some articles on acupuncture- induced pneumothorax published in Chinese and English medical journals since 1980.
Case:
A 35-year-old man presented with left chest pain and dyspnea after receiving acupuncture. The patient was later diagnosed with a 12% pneumothorax of the left lung. He was observed in an emergency room for 24 hours while being treated with oxygen, a painkiller, antibiotics, and bedrest. A follow-up computed tomography scan of his chest 1 week later showed complete resolution of the pneumothorax.
Case analysis and discussion:
Details of the case are analyzed. A general review of the incidence, causes, symptoms, and outcomes of acupuncture induced pneumothorax is presented. In addition, improved needling methods including needling depth and angle, together with corresponding precautions are also discussed.
Conclustions:
Pneumothorax caused by acupuncture therapy uncommon, but the consequences can be serious. It is important for practitioners to have adequate knowledge so they can implement better prevention of acupuncture-induced pneumothorax.
Introduction
Report
A 35-year-old male patient, who works as a chef, presented to an institution's acupuncture department complaining of pain in the hypochondriac region (upper laterial abdominal region just below the rib) and chest tightness 1 half hour after an acupuncture treatment received on January 10, 2011. He described the pain as sharp, stabbing, and radiating, and stated that it became worse with movement and deep breathing. This patient denied having any palpitations, cough, recent trauma, and any medical history of pneumothorax.
The patient's vital signs were as follows: temperature, 36.7°C; blood pressure, 110/75 mm Hg; heart rate, 76 beats per minute; and respiratory rate, 19 breaths per minute. His oxygen (O2) saturation was 94% in room air. No abnormal respiration sounds were heard in his chest and his cardiovascular system examination was unremarkable. Medical imaging was performed. A chest X-ray showed a small pneumothorax (Fig. 1) and a chest computed tomography (CT) scan showed a left-sided 12% pneumothorax (Fig. 2).

Chest radiograph showing left pneumothorax.
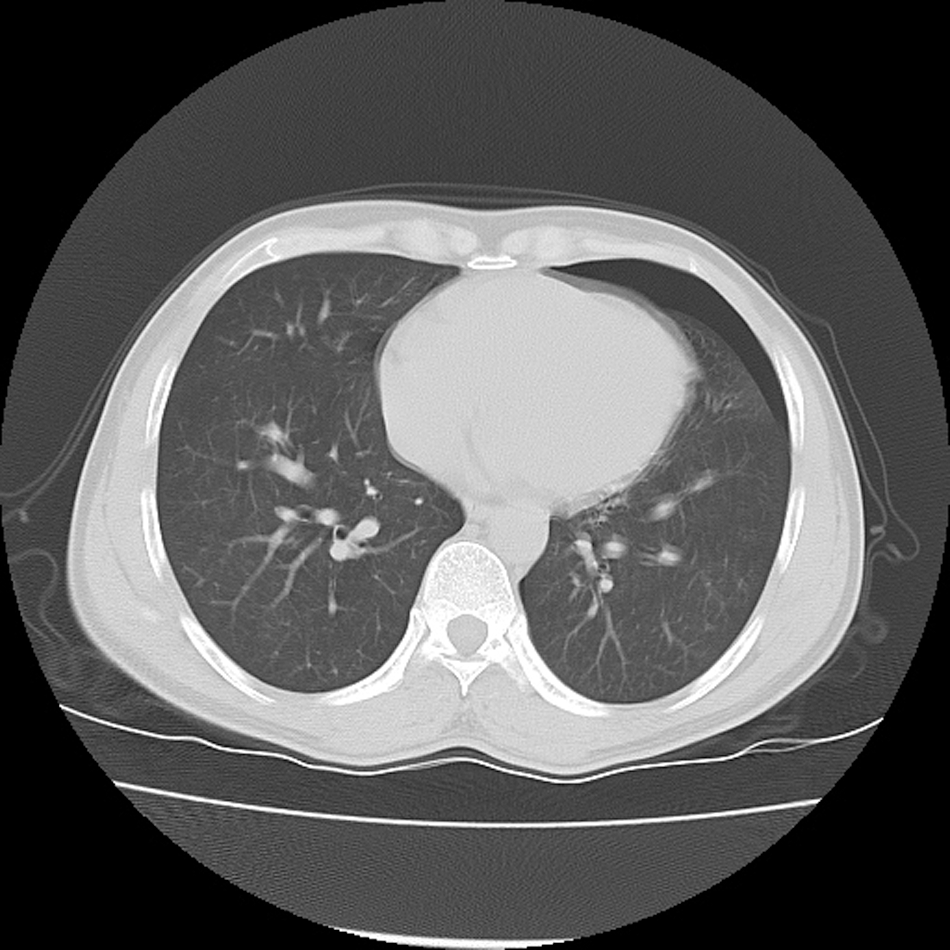
Chest computed tomography scan showing left-sided pneumothorax.
The treatment, based on the diagnosis of a small pneumothorax, was observation in the emergency room (ER), administration of supplemental O2 inhalation, Fenbid 0.3 p.o., b.i.d., cefadroxil 1.0 po b.i.d., and bedrest. Twenty-four (24) hours later, the patient's symptoms were greatly reduced. He was discharged with advice on how to self-manage his pneumothorax. A new chest CT was scheduled for the following week; that scan showed complete resolution of this patient's pneumothorax (Fig. 3).
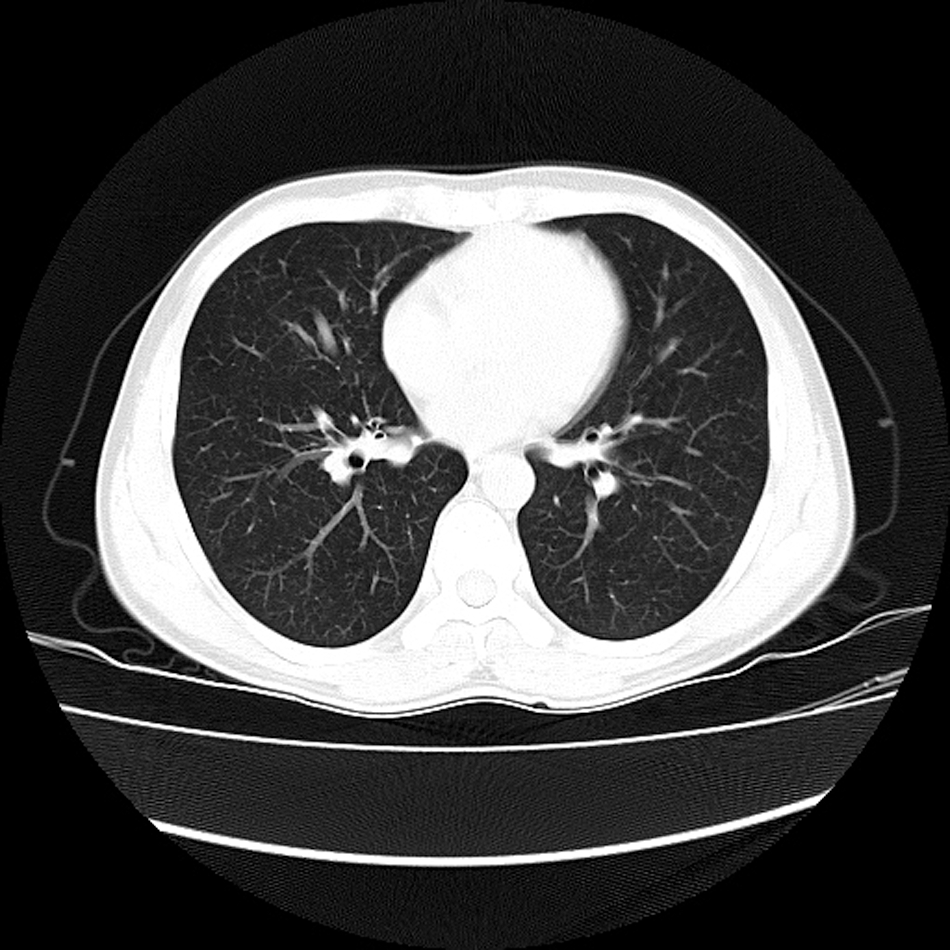
Chest computed tomography scan showed reduction of the pneumothorax.
Analysis
The patient's height is 175 cm and his weight is 50 kg. He smokes 2–3 cigarettes per day. He is a chef at a small roadside restaurant, serving Sichuan style food. The kitchen he works in is ∼ 6 square meters with only a small fan for ventilation. He lives right next to the restaurant, which is 1500 meters away from the hospital.
The patient had chronic back pain, which may have been related to long hours of standing at work. He had been coming to the hospital for acupuncture therapy three times per week for more than 2 weeks. The practitioner who treated this patient had more than 15 years of clinical experience. The acupuncture points selected were usually on the back in the paraspinal region. The patient's back pain was significantly reduced, and 2 more treatments were scheduled for that treatment course. On the day of the incident, the treatment was similar to prior treatments this patient had undergone. The points selected were BL 13 (Fei Shu), BL 17 (Ge Shu), BL 20 (Pi Shu), BL 23 (Shen Shu), and BL 25 (Da Chang Shu) in prone position. The needle size was 0.30 [[[times sign]]] 40 mm (Fig. 4). Insertion was oblique toward the spine, with a depth of 0.5–0.8 cun (13–20 mm). These needles were retained for 30 minutes. After removal of needles, cupping was also performed on these same points, and the cups were retained for 5 minutes. The patient did not complain of any discomfort during the treatment. After treatment, he went directly to work, which took him 5 minutes.
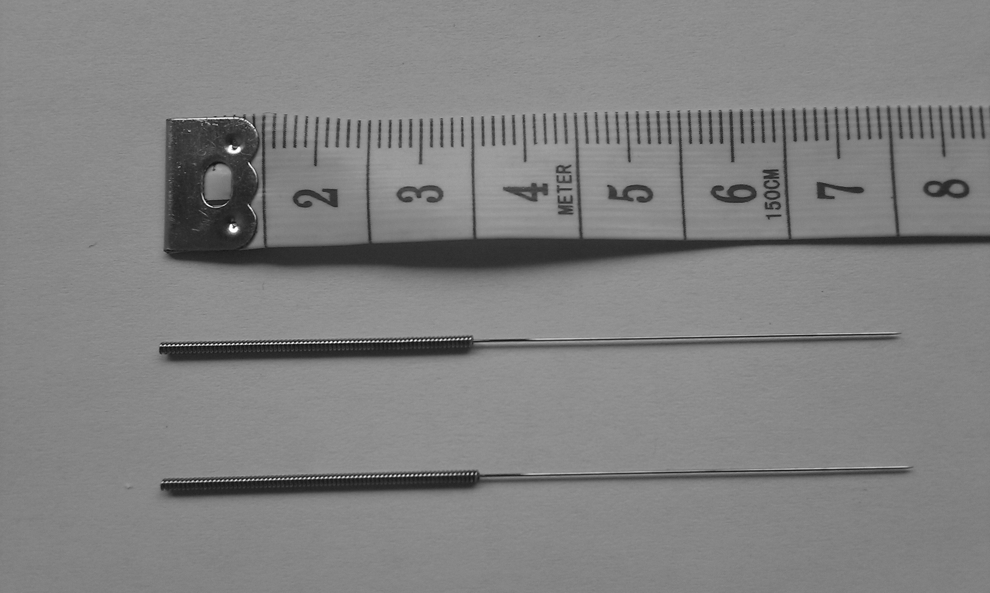
Acupuncture needles.
One half hour later, the patient returned to hospital's acupuncture department. He recalled that, during the acupuncture session, he had felt soreness in his hypochondriac region. He did not tell the acupuncture doctor because he thought that the sensation was normal Qi sensation. After going to work, he started to feel a stabbing pain, which worsened while tossing the wok as he was cooking.
A consultation group (comprised of experts from the acupuncture, respiratory care and radiology departments of the hospital) was involved in the diagnosis and treatment of this case. The diagnosis for this case was small pneumothorax. The causes and or complications of the pneumothorax were considered to be: 1. Acupuncture-induced, caused by: (a) needles being too long and insertion being too deep for this patient; and (b) cupping after needling changed the pressure at the needle insertion areas, which might have aggravated a possible existing pneumothorax. 2. Spontaneous pneumothorax was not excluded because: (a) the patient was tall and thin, thus he was in a population more likely to have spontaneous pneumothorax; and (b) the patient's occupation as a chef involved moving the muscles of the chest, back, and intercostal space forcefully and repetitively while tossing the wok as he was cooking, which might aggravate a potentially existing pneumothorax.
This patient was given the choice of going home for bedrest or staying in the ER for observance while receiving supportive treatment. The patient stayed for 24 hours' observation and supplemental treatment, which were successful. A follow-up chest CT scan 1 week later showed complete resolution of his pneumothorax. The patient still complained, however, of intermittent chest tightness and pain, presumably resulting from the trauma of his pneumothorax.
Discussion
Pneumothoraces can be broadly classified by their etiologies: spontaneous; traumatic; and iatrogenic. A pneumothorax occurs when a sufficient amount of air enters the pleural cavity to disrupt the surface tension adhering visceral to parietal pleura. 1 The incidence of pneumothorax varies in different health care systems and in different countries.
The incidence of primary spontaneous pneumothorax in men is 7.4 per 100,000 people per year in the United States and in women this incidence is 1.2 per 100,000 people per year. In the United Kingdom, it is 37 per 100,000 people per year in men and, in women, it is 15.4 per 100,000 people per year. 2 Bense et al. 3 reported that the annual incidence of first spontaneous pneumothorax in the County of Stockholm in Sweden was 6 per 100,000 people for women and 18 per 100,000 people for men.
Some researchers compared the incidence of different types of pneumothorax. Weissberg and Regaely 4 reviewed and analyzed records of 1199 patients with pneumothorax in a university-affiliated metropolitan medical center between 1980 and 1997. Primary spontaneous pneumothorax occurred in 218 patients, secondary spontaneous pneumothorax occurred in 505 patients, traumatic pneumothorax occurred in 403 patients, and iatrogenic pneumothorax occurred in 73 patients. Despars et al. 5 reviewed cases of pneumothorax that occurred between October 1983 and December 1988 at the Veterans Administration Medical Center, in Long Beach, CA. During that time period, 90 patients were diagnosed as have spontaneous pneumothorax and 106 patients were diagnosed as having iatrogenic pneumothorax. Celik et al. 6 reviewed records of patients who were treated for iatrogenic pneumothorax between December 1998 and December 2006 in the researchers' hospital. Among 12,010 invasive procedures 164 patients (1.36%) developed iatrogenic pneumothorax.
According to Celik, the most frequently involved invasive procedures in the etiology of iatrogenic pneumothorax are: transthoracic lung biopsy; transbronchial needle biopsies and pleural biopsies; thoracentesis for diagnosis or treatment; central venous catheterization; mechanical ventilation; intercostal nerve blockage; tracheostomy; and pacemaker replacement. Acupuncture is also one of the reasons for iatrogenic pneumothorax.
Acupuncture is among the most popular of all complementary and alternative therapies. It is an invasive therapy and is not free from risks. Articles were reviewed that were published in Chinese and English medical journals since 1980 on acupuncture-induced pneumothorax. Among these articles, some reported single cases and some reviewed general adverse events (AEs) following acupuncture.
Norheim 7 reviewed the adverse events reported in Europe and United States of America during 1981–1994. Of 162 cases, 22 were pneumothoraces. Zhang et al. 8 reviewed three Chinese databases that included literature between 1980 and 2009 on the subject of acupuncture-related AEs, and 201 cases of pneumothorax were reported. The total number of acupuncture treatments practiced over the study period was unknown, but the authors assumed that the annual number of acupuncture treatments would total from 50 to 100 million. Yamashita et al. 9 reviewed 89 articles published in Japan during 1987–1999 on AEs after acupuncture. Of 124 cases, 25 were pneumothorax. Eleven occurred during or immediately after needling. One case was accompanied by cardiac arrest. In Australia, a major survey of 3700 practitioners revealed that pneumothorax comprised 64 of 3222 AE. 10 Giles et al. 11 reported that there was only 1 significant complication (pneumothorax) in 7831 acupuncture treatment sessions, representing 0.01% of patients and 0.006% of a total of 16,936 examinations and treatments administered at the researchers' multidisciplinary spinal pain syndrome unit in Australia. Melchart et al. analyzed the data of a total of 97,733 patients, and there were only 2 cases of pneumothorax. 12 Witt et al. 13 reported the results of a prospective observational study of 229,230 patients who received 10.2±3.0 acupuncture treatments, and only 2 patients experienced pneumothorax.
Most patients reported in these articles recovered uneventfully. 14 –29 However, fatalities did occur. 30,31
Among the cases reviewed for the current study, the reasons for acupuncture-induced pneumothorax included: 1. The practitioners lacked anatomical knowledge or were not cautious during the treatment. 2. The needle insertion was too deep or the needle angle was incorrect. 3. The patients coughed, sneezed, or breathed too deeply during needle retention. 4. Thin patients or patients with long-term respiratory diseases had an increased risk of pneumothorax.
After the puncture of the lung by acupuncture, the time of symptom occurrence varied from patient to patient, it might be during acupuncture treatment, immediately following the removal of an acupuncture needle, or several hours or days after an acupuncture treatment. The severity of the symptoms was related to the severity of the lung injury. The progress and prognosis was related to each patient's general health condition, age, underlying disease condition, and complications.
It is important for acupuncturists to be aware of the severe outcomes of acupuncture-induced pneumothorax, to be familiar with the anatomy involved, to be cautious when needling points close to the lungs, to be aware of at-risk populations, and recognize the early signs and symptoms of pneumothorax.
The surface projection of the apex of the lungs is ∼ 1″ (2.5 cm) above the clavicle. The lower border of the lung has an excursion of as much as 2″–3″ (5–8 cm) in the extremes of respiration, but in the neutral position (midway between inspiration and expiration), the border lies along a line that crosses the sixth rib in the midclavicular line and the eighth rib in the midaxillary line, and reaches the tenth rib adjacent to the vertebral column posteriorly. The acupuncture points within this range should be needled shallowly and cautiously. The needle angle needs to be mostly oblique or transverse.
When the following symptoms happen during acupuncture, the possibility of a pneumothorax needs to be considered and emergency help should be sought: 1. Acute onset of chest tightness or chest pain 2. Acute onset of dyspnea and gradual aggravation 3. Acute onset of nonproductive cough, dizziness, and cold sweating 4. Aggravation of wheezing in patients with chronic respiratory diseases, such as asthma or pulmonary emphysema 5. Acute onset of heart palpitation 6. Acute onset of shock; when a patient goes into shock, two possibilities need to to considered: acu-shock (needle fainting) or shock resulting from a tension pneumothorax.
More care should be taken when needling patients who are prone to spontaneous pneumothorax. Sometimes, very tall thin people are prone to spontaneous pneumothorax. In this condition, the lung collapses after minimal or no trauma. Other risk factors are cigarette smoking and recreational drug use or abuse. Patients who are older, debilitated, and/or who have chronic respiratory diseases, such as pulmonary emphysema, should also be given more attention. Usually, these patients' lungs are weak or superficial, making them more susceptible to pneumothorax 32 or making it harder for such patients to recover once pneumothorax occurs.
Conclusions
Serious AEs caused by to acupuncture therapy are rare. Pneumothorax is not a common risk in an acupuncture clinic. However, pneumothorax does happen. This case described in this current report was a mild case, and the patient recovered quickly. However, in some cases, the consequence can be serious, especially for elderly or debilitated patients. The practitioner in this report is an experienced Chinese medicine doctor who had more than 15 years' of hospital work experience. Even an experienced practitioner may cause incidents. It is important for both experienced and beginner practitioners alike to be aware of the possibility of pneumothorax in acupuncture clinics and to improve clinical knowledge and practice for better prevention of acupuncture-induced pneumothorax.
Footnotes
Disclosure Statement
No financial conflicts exist.