
Abstract
Objectives:
The objective of the study was to investigate the effect of acupuncture on the circadian rhythm of blood pressure (BP) in patients with hypertension.
Design:
The study was designed as a randomized, double-blind, controlled trial. Subjects were randomly divided into an active acupuncture group and a sham acupuncture group. Each patient received real or sham acupuncture treatment twice a week for 8 weeks. Acupuncture needles were inserted at bilateral ST 36 plus PC 6; placebo points.
Subjects:
Thirty-three (33) patients with essential hypertension were the subjects.
Outcome measures:
Twenty-four (24)-hour ambulatory BP was assessed before and after treatment.
Results:
After the treatment period, there was a significant increase in nocturnal diastolic BP dipping compared to that at baseline (10.20±7.56 mm Hg versus 5.21±10.19 mm Hg, p=0.038) in the active acupuncture group but not in the sham acupuncture group. The nocturnal diastolic BP dipping response to active acupuncture treatment was significantly different from the response seen with the sham acupuncture treatment (p=0.041). The number of dippers also increased from 4 to 8 in the active acupuncture group. Average systolic and diastolic BP was not changed significantly except for nighttime diastolic BP (90.32±11.47 mm Hg to 87.83±9.16 mm Hg, p=0.041).
Conclusions:
It is suggested that acupuncture treatment could be useful for improving the circadian rhythm of BP in patients with hypertension.
Introduction
Acupuncture, which has been used for centuries and is thought to be potentially helpful for lowering BP, has been explored both in Western and Eastern literature. 15 –17 Recently, several randomized controlled trials have been conducted on the effects of acupuncture on hypertension. Some studies showed that acupuncture can lower BP in patients with hypertension, 15,16 while another reported contradictory results. 17 Therefore, the effect of acupuncture on hypertension is still controversial. However, little is known about whether or not acupuncture can regulate the circadian rhythm of BP.
Acupuncture has been reported to normalize decreased parasympathetic nerve activity, 18 which is thought to be the cause of the absence of nocturnal BP dipping. 19 It was therefore hypothesized that acupuncture would regulate the circadian rhythm of BP. To test this hypothesis, a randomized, double-blind, placebo-controlled trial of acupuncture treatment was conducted on variation in the circadian rhythm of BP and average BP in patients with hypertension.
Subjects and Methods
Ethical approval
The study was performed in accordance with the ethical standards of the Helsinki Declaration. The Institutional Review Board of the Kyung Hee University Hospital at Gangdong approved the study protocol. Written, informed consent was obtained from all subjects after they were provided with a complete explanation of the study.
Subjects
The study was carried out from July 2009 to June 2010 at the Kyung Hee University Hospital at Gangdong, Korea. Patients were recruited through the website and bulletin boards of the hospital. They were screened for participation if they fulfilled all of the following inclusion criteria: Stage I hypertension (classification and management of BP for adults aged 18 years or older according to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High BP 7, corresponding systolic blood pressure [SBP] ranging from 140 to 159 mm Hg or diastolic blood pressure [DBP] ranging from 90 to 99 mm Hg), aged 18 to 70 years, and no previous use of antihypertensive medication. The exclusion criteria were secondary hypertension, diabetes mellitus, previous use of antihypertensive medication, current smoker, pregnancy, severe heart failure, and acute or unstable coronary artery disease. Patients were eliminated from the study if they missed more than five visits or started taking antihypertensive agents.
Study protocol
The study was a prospective, randomized, controlled clinical trial in which the patients and the observers were unaware of the treatment allocation. Eligible subjects who fulfilled the inclusion criteria were randomly assigned to either an active acupuncture group or a sham acupuncture group (block size 4) in a 1:1 ratio. Consecutively numbered, opaque envelopes containing a sheet with the allocation were prepared and opened after the patients had been included in the study. After randomization, subjects received active or sham acupuncture treatment twice a week for 8 weeks. The 24-hour ambulatory BP level was measured in each patient before and after the 8 weeks of acupuncture treatment.
BP measurements and patient classification
Ambulatory BP measurements were performed with an oscillometric device (Tonoport V, GE Medical System Information, Germany) programmed to collect 38 measurements during each 24-hour monitoring period. Measurement intervals were 30 minutes during the day (8:00
In most people, BP drops by 10%
Interventions
All acupuncture therapy was given by a single physician trained in traditional Korean medicine. Sterile, disposable, stainless-steel needles (length 4 cm, diameter 0.25 mm) were used. In the active group, acupuncture needles were inserted at bilateral ST 36 and PC6. After being inserted to a depth of about 2 cm, they were manually stimulated until achieving de qi, a situation in which patients experience a radiating sensation considered to be indicative of effective needling. After achieving de qi, the needles were left in place for 20 minutes without manipulation and then removed. In the sham acupuncture group, nonacupuncture points (which are 1 cm lateral from ST 36 and PC6) were needled superficially and bilaterally. De qi and manual stimulation of the needles were avoided. The duration of needle insertion was the same in the sham treatment as for the active acupuncture group. For each session, any adverse event related to acupuncture was recorded using a checklist that included bleeding, hematoma, dizziness, infection, neurological symptoms, fainting, nausea, and pain.
Outcomes
The primary endpoints were the average nocturnal BP dipping levels of SBP and DBP according to 24-hour ambulatory BP monitoring. The secondary endpoints were the nocturnal BP dipping patterns, average SBP and DBP levels, and average daytime and nighttime SBP and DBP levels.
Statistical Analysis
All results were expressed as mean±SD unless otherwise stated. Data were analyzed using one-sample t-test, two-sample t-test, and χ2 test. A value of p<0.05 was considered significant. All calculations were performed using SPSS for Windows, version 13.0 (SPSS Inc., Chicago, IL).
Results
Subjects
A total of 72 interested subjects contacted the trial coordinator; 39 were not enrolled because they either were not interested after further information or did not meet the inclusion criteria. Therefore, 33 subjects were randomized into either the active acupuncture group or the sham acupuncture group. Five (5) subjects in the active acupuncture group withdrew or were lost to follow-up by week 8 (Fig. 1). One (1) patient was eliminated because he drank alcohol several hours before follow-up 24-hour ambulatory BP measurement. The others dropped out because of personal reasons (distance, personal work, etc.). Data from the 12 subjects in the active acupuncture group and the 16 subjects in the sham acupuncture group who completed the follow-up assessment after the 8 weeks of treatment were included in the primary analysis. The baseline characteristics of the subjects are summarized in Table 1. There were no significant differences in age, gender, body–mass index, average SBP and DBP levels, serum glucose, or lipid levels except for high-density lipoprotein cholesterol (Table 1).
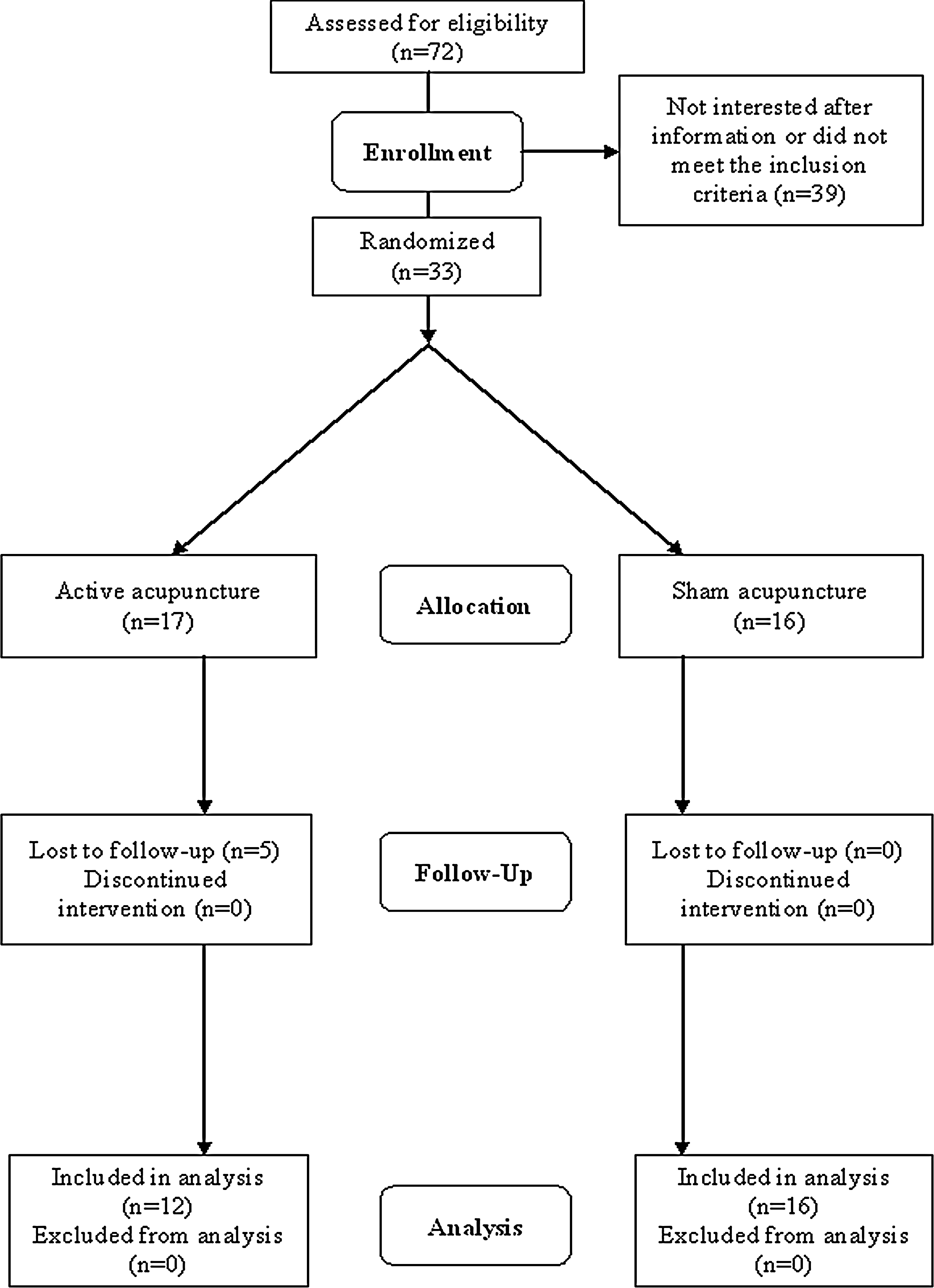
Patient flow chart.
p<0.05 in two-sample t-test versus sham acupuncture group.
BMI, body–mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBS, fasting blood sugar; Total-chol, total cholesterol; HDL-chol, HDL cholesterol.
Nocturnal BP dipping
After the 8-week treatment, there was a significant increase in nocturnal DBP dipping compared to that at baseline (10.20±7.56 mm Hg versus 5.21±10.19 mm Hg, p=0.038) in the active acupuncture group but not in the sham acupuncture group. The nocturnal DBP dipping response to active acupuncture treatment was significantly different from the response seen with the sham acupuncture treatment (p=0.041). In contrast, nocturnal SBP dipping was unchanged after acupuncture treatment in both groups (Table 2).
Nocturnal dipping (%): [(daytime SBP - nighttime SBP)/daytime SBP)]*100.
Δ1, differences before and after treatment in active acupuncture group.
Δ2, differences before and after treatment in sham acupuncture group.
p<0.05 in one-sample t-test versus baseline; ** p<0.05 in two-sample t-test versus sham acupuncture group.
SBP (mm Hg), systolic blood pressure; DBP (mm Hg) diastolic blood pressure.
At the baseline BP assessment, there were 8 (67%) nondippers in the active acupuncture group and 6 (38%) in the sham acupuncture group. After acupuncture treatment, the number of nondippers in the active acupuncture group decreased to 4 (33%), while the number in the sham group increased to 8 (50%).
Average BP levels
There were no significant changes in the average SBP and DBP levels or average day and nighttime SBP. The nighttime DBP was significantly decreased in the active acupuncture group (p=0.041), but not in the sham treatment group. The active group experienced a decrease from 90.32±11.47 mm Hg to 87.83±9.16 mm Hg after the 8-week treatment (Table 3).
Δ1, differences before and after treatment in active acupuncture group.
Δ2, differences before and after treatment in sham acupuncture group.
p<0.05 in two-sample t-test versus sham acupuncture group.
SBP (mm Hg), systolic blood pressure; DBP (mm Hg), diastolic blood pressure.
Adverse events of acupuncture
No serious adverse events (AEs) were reported. Observed AEs were related to the insertion of the needles, such as: transient slight injection-site pain and small bleeding.
Discussion
To the best of the authors' knowledge, this is the first randomized double-blind clinical trial to evaluate the efficacy of acupuncture on the circadian rhythm of BP in patients with hypertension. In this study, acupuncture significantly increased nocturnal DBP dipping and decreased nighttime DBP. Relevant to these findings, the number of nondippers in the active treatment group decreased from 8 (67%) to 4 (33%). These results are of interest because there is increasing evidence that nocturnal dipping may be an important predictor of both target-organ damage and cardiovascular events, independent of 24-hour average BP level. 3 –6,21
Circadian rhythm of BP refers to the diurnal variation in BP, which is generally higher during the day than at night. Most people experience a decline in arterial BP in the range of 10%–20% during the night. These people are called dippers, while people who lack this nocturnal reduction in BP are called nondippers. 4
Various factors such as abnormal neurohormonal regulation, lack of physical activity, increased sodium intake, and smoking can cause a person to become a nondipper. 22 Among these factors, growing evidence indicates that nondipping is related to an imbalance between the tone of the sympathetic nerve system and that of the parasympathetic nerve system, particularly the failure to shift from sympathetic to parasympathetic activity during sleep. 19,23 –25 In general, plasma and urine catecholamines are lower during the night than they are during the day, 26 and direct recordings from the muscle sympathetic nerves have also shown decreased levels of activity during slow-wave, but not rapid eye movement, sleep. 27 In contrast, it was reported that catecholamine levels were significantly higher in nondippers compared to those in dippers, 28 and that nondippers had impaired function of the autonomic nervous system, characterized mainly by decreased parasympathetic system activity. 29
A decrease in nocturnal BP dipping was reported to have a linear relationship with cardiovascular mortality. On average, each 5% decrease in the decline in nocturnal systolic/diastolic BP was associated with an approximately 20% greater risk of cardiovascular mortality. 4 A significant association between cerebrovascular events and the absence of a nocturnal dip has also been reported. 3 –6 Thus, the antihypertensive agents that have been shown to affect nocturnal BP dipping have recently started to be emphasized. There are many studies about the nocturnal dipping effects of antihypertensives such as amlodipine, verapamil, doxazocin, nilvadipine, and barnidipine. 7 –14 In those studies, the effects of antihypertensives on nocturnal dipping ranged from 0.7 mm Hg to 12 mm Hg. In the present study, nocturnal dipping increased by 4.98±7.34 mm Hg (5.21±10.19 mm Hg to 10.20±7.56 mm Hg, pretreatment to post-treatment) after acupuncture treatment, indicating its potential to improve the circadian rhythm of BP in patients with hypertension.
The manner in which acupuncture improves the circadian rhythm of BP is not clear at the present time. There are many studies showing that acupuncture regulates the autonomic nervous system. 28,30 –34 In particular, ST 36 and PC 6, the acupoints used in this study, have been shown to balance the autonomic nervous system, 30 suppress heart rate and low-frequency/high-frequency ratio, 33 and normalize high-frequency power. 34 Hence, one can speculate that the effect of acupuncture on nocturnal BP dipping might result, in part, from suppression of the sympathetic tones and increased parasympathetic activities.
Whether acupuncture can lower BP is still controversial. 15 –17 Two (2) recent randomized controlled trials showed that acupuncture lowered BP, 15,16 but another study indicated the opposite. 17 Among these studies, only one was conducted using 24-hour ambulatory BP measurement, 16 while the others used the mean BP of three to five casual BP measurements. 15,17 Those studies with casual BP measurements could have missed the nighttime BP changes after acupuncture treatment. In this study, there were no significant changes in average SBP and DBP levels except for nighttime DBP. Without 24-hour ambulatory BP measurement, the nighttime changes might not have been detected. The authors agree that nighttime BP changes alone are not sufficient to conclude that acupuncture has a BP-lowering effect. However, to determine how acupuncture affects BP, it is suggested that 24-hour ambulatory BP measurements should be used.
Conclusions
Several limitations of this study should be noted. First, this study was a small trial, and the authors did not continue to measure BP changes after acupuncture treatment was discontinued. Therefore, a concrete conclusion cannot be drawn from this study. Furthermore, the autonomic function of the patients in this study were not measured, so the data are insufficient to indicate a direct correlation between the effect of acupuncture on diurnal BP change and the autonomic nervous system. A trial with a larger patient population, long-term follow-up, and measurement of autonomic function is needed to more conclusively determine the efficacy of acupuncture on BP reduction and to elucidate the duration of its effects.
Footnotes
Acknowledgments
This work was supported by the Korea Research Foundation Grant funded by the Korean Government (MOEHRD, Basic Research Promotion Fund) (KRF-2008-331- E00438).
Disclosure Statement
All authors declare no competing financial interests exist.