
Abstract
Objective:
The aim of this meta-analysis was to evaluate the effects of yoga on psychologic function and quality of life (QoL) in women with breast cancer.
Design:
A systematic search of PubMed, EMBASE, the Cochrane Library, the Chinese Biomedical Literature Database, and the Chinese Digital Journals Full-text Database was carried out. Randomized control trials (RCTs) examining the effects of yoga, versus a control group receiving no intervention, on psychologic functioning and QoL in women with breast cancer were included. Methodological quality of included RCTs was assessed according to the Cochrane Handbook for Systematic Reviews of Interventions 5.0.1, and data were analyzed using the Cochrane Collaboration's Review Manager 5.1.
Results:
Six (6) studies involving 382 patients were included. The meta-analysis showed that yoga can improve QoL for women with breast cancer. A statistically significant effect favoring yoga for the outcome of QoL was found (standard mean difference=0.27, 95% confidence interval [0.02, 0.52], p=0.03). Although the effects of yoga on psychologic function outcomes—such as anxiety, depression, distress and sleep—were in the expected direction, these effects were not statistically significant (p>0.05). Fatigue showed no significant difference (p>0.05).
Conclusions:
The present data provided little indication of how effective yoga might be when they were applied by women with breast cancer except for mildly effective in QOL improvement. The findings were based on a small body of evidence in which methodological quality was not high. Further well-designed RCTs with large sample size are needed to clarify the utility of yoga practice for this population.
Introduction
Yoga is an ancient Eastern tradition, which is one of six branches of classical Indian philosophy and has been practiced for thousands of years. 19,20 The word yoga is probably derived from the Sanskrit word YUJ that means “to join the mind.” Yoga is traditionally believed to have positive effects on physical, mental, and spiritual health. Yoga's effects have been explored in a number of patient populations, some primarily medical, others psychologic, and others social. 21 –26 Over the last few years, yoga, as one popular form of many CAM adjunctive approaches, 27 has been studied extensively as a potentially beneficial intervention for patients with cancer, exploring a variety of outcomes, including sleep quality, mood, stress, cancer-related distress, cancer-related symptoms, and overall QoL, as well as functional and physiologic measures. 28 –30 Results from this emerging literature has suggested that yoga was a feasible intervention for a wide range of patients with cancer and survivors of this disease.
There has been interest in the therapeutic application of yoga for patients with breast cancer, many of whom have been examined using randomized controlled trials (RCTs). These studies have shown that the yoga-based interventions decreased fatigue, depression, and anxiety, and improved subjective measures of well-being. In addition to studies on the effects of yoga on disease-related symptoms, some researchers reported the effects of yoga on treatment-induced nausea, vomiting, and other related side-effects in patients with breast cancer. 31
Despite the wide clinical use of yoga and positive experiences with this form of treatment, there has been no published quantitative review about the effectiveness of yoga for breast cancer to date. The current meta-analysis was performed to summarize the evidence, specifically examining the effects of yoga on psychologic function and QoL in women with breast cancer, as these are important clinical concerns, and to examine outcomes of cancer treatment for these patients. These results can be useful for practitioners who are making decisions about recommendations for overall treatment.
Materials and Methods
Inclusion criteria
RCTs comparing yoga alone or a yoga-based intervention with a control group receiving no intervention for psychological functioning and QoL in women with breast cancer were included.
The studies had to examine yoga as a main intervention. Studies that included yoga as part of a larger intervention program (e.g., mindfulness stress-reduction training), and/or those that did not provide findings specific to yoga, were excluded.
Literature search
Searches were conducted in PubMed, EMBASE, the Cochrane Library, the Chinese Biomedical Literature Database, and the Chinese Digital Journals Full-text Database from their inception to May 2011, with no language restrictions. This search was conducted according the following strategy: (
Methodological quality assessment and data extraction
Methodological quality of each included study was assessed individually by 2 reviewers for major potential sources of bias using criteria recommended in the Cochrane Handbook for Systematic Reviews of Interventions 5.0.1. 32 When differences existed, a consensus was reached through discussion. Four domains related to the risk of bias were assessed: (1) sequence generation; (2) allocation concealment; (3) blinding of participants, clinical staff, and outcome assessors; and (4) incomplete outcome data.
Two (2) reviewers used a standard data extraction checklist to extract the data independently from each study, including study characteristics (e.g., first author's name, year of publication, and country where the study was conducted), characteristics of study subjects (e.g., number of participants, age, and breast cancer stage), intervention details (type of intervention, frequency, and duration), and outcome measures. Quantitative data were extracted to calculate effect sizes. Data on effect size that could not be obtained directly were recalculated when possible. If there were many assessment timepoints, the time point of postintervention was chosen.
Data synthesis
For continuous variables, the current authors calculated mean difference (MD) or standard mean difference (SMD) with 95% confidence intervals (CI) in case the units of measurement were not comparable. For dichotomous data, results were presented as risk ratio (RR) with a 95% CI. Heterogeneity was explored using Cochran's χ2 test and the I 2 test (heterogeneity was investigated by evaluating if CIs around the individual effect sizes of pooled studies overlapped sufficiently). A fixed effects model was used to pool the results together unless significant heterogeneity was observed (p<0.1 and I 2>50%), which would have needed a random-effects model. The analysis was performed using Review Manager 5.1.
Results
Studies selection
Figure 1 presents a flow diagram illustrating the studies selection process. The electronic searches identified 86 studies. Among these, 24 duplicates were excluded by using Endnote software, and 39 articles were excluded after initial screening because they were not RCTs, or subjects and interventions were not related to the topic this study was concerned with. Twenty-three (23) full-text articles were maintained for further screening. Of these 23 studies, 17 were excluded for the following reasons: duplicate publications (n=1); non-RCTs (n=1); subjects included other patients with cancer (n=1); interventions of interest not tested (n=8); insufficient data provided and author was not reachable (n=1); and 5 were conference abstracts (as of this writing, it was not possible to find more information about these 5 studies). Finally, 6 RCTs were included in this meta-analysis. 33 –38 References cited in published original and review articles were examined until no further studies were found.
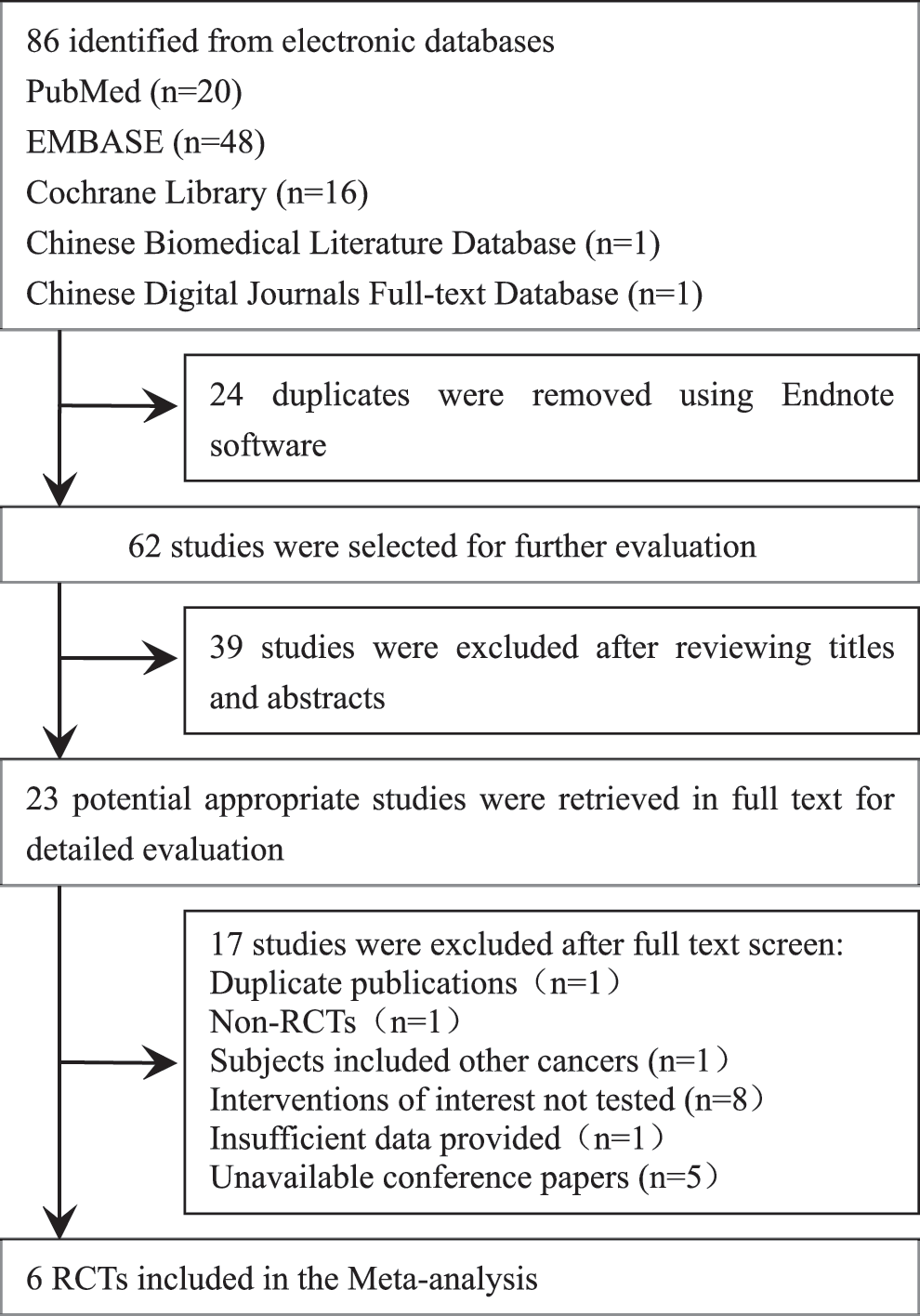
Flowchart of inclusion of studies. RCTs, randomized controlled trials.
Characteristics of included studies
The characteristics of studies included in the meta-analysis are presented in Table 1.
SD, standard deviation; YIDL, Yoga in Daily Life; QoL, quality of life; FACIT-F, Functional Assessment of Chronic Illness Therapy—Fatigue; FACT-G, Functional Assessment of Cancer Therapy—General; CES-D, Center for Epidemiologic Studies—Depression; FACT-F, Functional Assessment of Cancer Therapy—Fatigue; PSQI, Pittsburgh Sleep Quality Index; FACT-B, Functional Assessment of Cancer Therapy—Breast; STATE, Speilberger state anxiety inventory; BFI, Brief Fatigue Inventory; RSCL, Rotterdam Symptom Checklist; PSS-14, Perceived Stress Scale—14.
The combined sample size across six included studies was 382 participants. Of the included studies, five were performed in America, 33 –36,38 and one in Slovenia. 37 All participants were women with breast cancer age ≥30. The patient samples of 3 studies consisted of patients with nonmetastatic breast cancer, 35 –37 whereas 3 studies 33,34,38 included a mix of patients with nonmetastatic and metastatic cancer. All studies compared yoga with a wait-list or no treatment control condition. Although these studies used various forms of yoga, training mainly consisted of physical stretches and poses, breathing exercises, and meditation. The intervention programs ranged from 4 weeks to 6 months, and the frequency of classes varied from one session per week to five sessions per week.
Methodological quality of included studies
Table 2 shows the quality assessment of the studies in this meta-analysis. All 6 of the included studies were stated to be randomized, but only 2 35,37 specified the method of randomization. Allocation concealment was not reported in any of the trials. To the current authors' knowledge, it is not possible to blind participants and therapists to intervention in these trials. Only the blinding of assessors is possible. However, only one trial 37 reported blinding of assessors. The number of withdrawals was clearly reported in all included trials 32 –35,37 except for 1 37 that apparently had no dropouts. The reasons for the dropouts were also given in all these trials.
Effects of interventions
There were 6 studies that compared yoga with wait-list or “no treatment” control condition. The data measured at postintervention were used for all outcomes. Results in these studies involved participants included by the researchers in their analyses, many of whom excluded participants for many reasons, including dropouts or uncollected data. Statistical heterogeneity was examined for each outcome. A negative direction for MD or SMD of bad outcomes indicates that the intervention condition produces more improvement in outcomes than the control condition, and vice versa. Table 3 provides a summary of the results of the overall meta-analysis for each of the outcomes.
MD, mean difference; SMD, standard mean difference; CI, confidence interval.
Anxiety
Two (2) studies involving 186 participants were included in this comparison. 33,35 A fixed-effects model was applied, because no statistical heterogeneity was indicated (p=0.75, I 2=0%). The result of the meta-analysis showed that there was no significant difference between yoga and the control groups (SMD=−0.24, 95% CI [−0.54, 0.06], p=0.11; Fig. 2).

Anxiety assessment after intervention with yoga versus control. SD, standard deviation; CI, confidence interval.
Depression
Two (2) studies reported depression involving 85 participants. 34,35 A random-effects model was used, because the heterogeneity test showed an I 2 of 59% among the studies (p=0.12, I 2=59%). No significant difference was observed between yoga and the control groups (MD=−4.12, 95% CI [−13.05, 4.81], p=0.37; Fig. 3).

Depression assessment after intervention with yoga versus control. SD, standard deviation; CI, confidence interval.
Distress
Two (2) trials involving 160 participants reported this outcome. 33,37 Heterogeneity analyses revealed substantial heterogeneity across studies (p<0.00001, I 2=98%), and therefore, a random-effects model was used. No significant difference was observed (SMD=−3.05, 95%CI [−8.63, 2.53], p=0.28). This indicated that yoga did not reduce distress perceived by patients with breast cancer in the treatment groups, compared to such patients in the control groups. (Fig. 4).

Distress assessment after intervention with yoga versus control. SD, standard deviation; CI, confidence interval.
Perceived stress
Only 1 study assessed the effect of yoga on perceived stress, 37 and, thus, a summary of effect size could not be calculated; the current authors just described that trial's results. In this RCT, 32 patients with breast cancer were randomly assigned to an experimental or a control group. After the intervention, patients receiving yoga practice showed less stress than those patients receiving no intervention (MD=−15.75, 95% CI [−18.80, −12.70], p<0.01).
Fatigue
Five (5) 33 –36,38 of the 6 studies included fatigue as an outcome measures. There was no heterogeneity between trials (p=0.56, I 2=0%), so a fixed-effects model was used to pool the estimate. The pooled data from these studies indicated that there was no significant difference between the yoga groups and the control groups (SMD=0.11, 95%CI [−0.12, 0.35], p=0.35; Fig. 5).
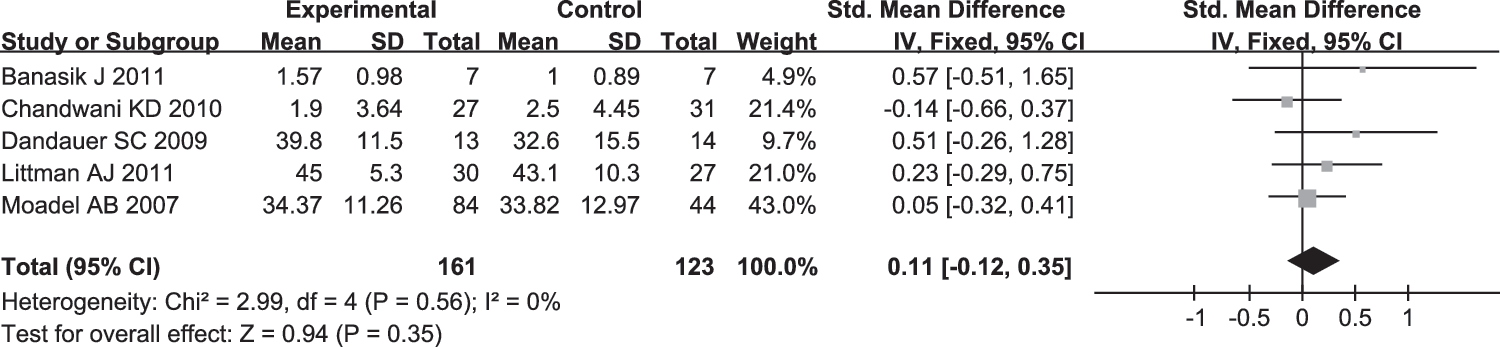
Fatigue assessment after intervention with yoga versus control. SD, standard deviation; CI, confidence interval.
Sleep
Two (2) trials involving 85 participants measured the sleep state of women with breast cancer. 34,35 A fixed-effects model was applied, because no statistical heterogeneity was indicated (p=0.71, I 2=0%). No significant difference was observed between the groups (MD=−0.44, 95% CI [−2.54, 1.66], p=0.68; Fig. 6).

Sleep assessment after intervention with yoga versus control. SD, standard deviation; CI, confidence interval.
QoL
Five (5) studies involving 288 participants examined the impact of yoga on QoL, 33 –36,38 but the data from Banasik et al. 38 were not available in a format to pool with other studies, so only 4 studies 33 –36 were included in the data pooling. A fixed-effects model was applied, because no statistical heterogeneity was indicated (p=0.83, I 2=0%). The results of the meta-analysis revealed that yoga had a positive effect on QoL, compared with control conditions; this effect was statistically significant (SMD=0.27, 95% CI [0.02, 0.52], p=0.03; Fig. 7).
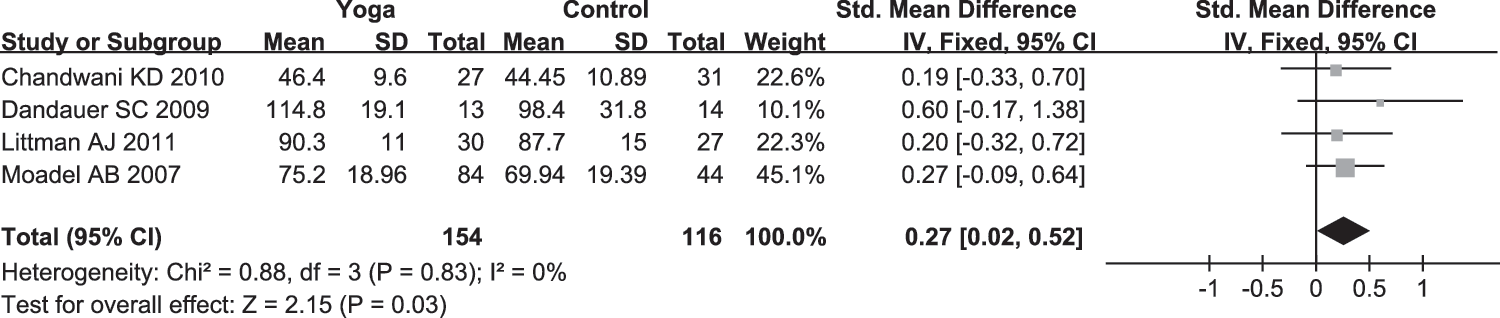
Quality-of-life assessment after intervention with yoga versus control. SD, standard deviation; CI, confidence interval.
Sensitivity analysis
Given the contradictory result of heterogeneity testing on depression, a fixed-effects model was used instead of a random-effects model to assess the robustness of conclusions about the quality of data. After sensitivity analysis, no change was found in the results (MD=−2.81, 95% CI [−7.94, 2.33], p=0.28).
Discussion
General findings
This meta-analysis provided a comprehensive summary of the currently available RCTs exploring the effects of yoga on psychologic parameters and QoL in patients with breast cancer and survivors of the disease. The combined results showed that a statistically significant difference was found for the effect of yoga on QoL; and effects on anxiety, depression, distress, and sleep were in the expected direction; but no statistically significant differences were observed. Only 1 study assessed the effect of yoga on stress, and, thus, a summary of the effect size could not be calculated.
In the studies reviewed for the current article, various forms of yoga were used. However, no matter which kind of yoga was tested, it used postures, breathing practices, meditation, or a combination of all these. These practices are known to build inner awareness and attention to mental phenomena, which contributes to the improvement of QoL. 35 In addition, staying physically active during and after treatment for breast cancer, and the relaxation response produced by yoga—which encompasses an integrated set of changes including increased breath volume and decreased heart rate—were also beneficial for maintaining QoL. 39,40
Yoga is known to have been associated with some reduction in symptoms, especially negative emotions in psychologic disorders. In the current meta-analysis, no statistically significant effects were observed from pooling data on psychologic outcomes. However, discussion of some trends was possible. As expected, there was a tendency toward decreases in the outcomes of anxiety, depression, distress, and sleep at postintervention. The minimal impact of yoga on these outcomes may be explained by several factors, including the small number of studies included in the review, differing measures used across the included studies, and limitations of available measures. In addition, another possible explanation is that being on a wait-list for treatment had a “holding” positive influence, decreasing the apparent effects of the yoga intervention. It is known that a wait-list is frequently used as an ethical “no treatment” condition to ensure that all participants eventually receive the “active” treatment. The analysis always treated “usual care” and “wait-list” controls as equivalent to “no treatment.” However, previous studies have suggested that effects in usual care may be significantly lower. 41 It should be noted that, the current results did not show a positive direction for yoga on fatigue. Consistent with a previous study, 42 insufficient data exist at present to recommend any specific CAM modality for cancer-related fatigue.
Limitations
To reach a high internal validity, only RCTs were included to explore the effects of yoga on psychologic function and QoL, which has become increasingly important for patients with breast cancer who may experience sequelae related to cancer diagnoses and treatments. However, several important limitations of the current studies and this meta-analysis should be noted.
First, there were a small number of studies and small sample sizes within studies in this review. The power of the studies was low because of these small sample sizes. In many cases, the CIs in the outcomes measured were so wide that the interval encompassed negative effects. Moreover, because of the small number of studies eligible for the review, funnel plots to assess publication bias were not created according to recommendations.
Second, methodological limitations of the studies influenced the overall effect size. All 6 studies mentioned randomization, but only 2 reported randomization methods. No studies made reference to whether or not any process of concealment of allocation was used. In these cases, selection bias may have existed in these studies. In addition, there were large or severe imbalances in terms of numbers of attrition in 3 studies, 33,34,38 which may have caused a high risk of attrition bias. The difficultly of blinding ratings of outcomes may have resulted in these studies being prone to observation bias. All of these affected the strength of evidence.
Third, differences did exist in various studies. The yoga sessions varied in frequency and duration, and many different outcome measures were used in these studies. This meant that many comparisons from these studies were included in the same analysis, which may have resulted in an artificial reduction of heterogeneity. The failure to identify effects for the psychologic outcomes measured may be particularly vulnerable to this criticism. In view of existing heterogeneity, random-effect analyses were used, resulting in wider CIs and relatively more weight being given to smaller studies.
Finally, the main limitation of the meta-analysis came from the relative lack of data for combination. An effect on psychosocial functioning or QoL was frequently accompanied by a change in behavior. One has to comply with a training program to achieve the desired reduction in bad outcomes and improvement in good outcomes. But very few studies provided complete information to allow this to be incorporated. To overcome problems involving missing data, the current meta-analysis was based only on cross-sectional data, which were likely to produce a lack of power to detect genuine effects that may have arisen from the interventions.
Implications for research
Further high-quality RCTs are needed to evaluate the effect of yoga on symptom management in patients with breast cancer. Although formal blinding of participants and clinicians to treatment arms is not inherently possible in these trials, blinding of investigators may reduce observer bias. It would be ideal if the records were maintained by blinded observers. In addition, when attrition in the study is severe, a correct intention-to-treat analysis would be needed, which would provicd a pragmatic estimate of the benefit. What is more, the current authors wish to emphasize standardization of instruments for assessing outcomes. If possible, decisions about which measures to assess outcomes should be made according to the methods of existing trials, aiming to add to aspects of which some data have already been accrued. The data integrity also requires attention in future studies.
Conclusions
At present, there was insufficient evidence to advocate that yoga should be offered routinely to women diagnosed with breast cancer. However, it may be an acceptable intervention to improve QoL for these women, and pooling data also showed potential benefits of yoga for releasing of negative emotions. The findings were based on only 6 RCTs, some of which were relatively small, so more methodologically rigorous, large-scale, randomized controlled trials are required to confirm these preliminary estimates of effectiveness. Meanwhile, evidence for yoga, compared with other CAM therapies, such as relaxation or support therapy, is also needed to make conclusions about superiority of one intervention over others.
Footnotes
Acknowledgments
The authors gratefully acknowledge Jean Glover, MD, lecturer and Jinbing Bai, MD, lecturer of Tianjin Medical University for helping in revising this article.
Disclosure Statement
No competing financial interests exist.