
Abstract
Objectives:
The objective was to determine the effect of myofascial techniques on the modulation of immunological variables.
Design:
Thirty-nine healthy male volunteers were randomly assigned to an experimental or control group.
Interventions:
The experimental group underwent three manual therapy modalities: suboccipital muscle release, so-called fourth intracranial ventricle compression, and deep cervical fascia release. The control group remained in a resting position for the same time period under the same environmental conditions.
Outcome measures:
Changes in counts of CD3, CD4, CD8, CD19, and natural killer (NK) cells (as immunological markers) between baseline and 20 minutes post-intervention.
Results:
Repeated-measures ANOVA revealed a significant time×groups interaction (F 1,35=9.33; p=0.004) for CD19. There were no significant time×group interaction effects on CD3, CD4, CD8, or NK cell counts. Intrasubject analyses showed a higher CD19 count in the experimental group post-intervention versus baseline (t=−4.02; p=0.001), with no changes in the control group (t=0.526; p=0.608).
Conclusion:
A major immunological modulation, with an increased B lymphocyte count, was observed at 20 minutes after the application of craniocervical myofascial induction techniques.
Introduction
It has been proposed that three mechanisms—piezoelectricity, myofibroblast dynamics, and viscoelasticity 6 —operate at micro and/or macro levels of body movement and at different time scales, and that each can influence the behavior of the other two. 7 –11 Thus, all signals can interact, according to the response of the fascial system during treatment. 7 Therapy can have the following effects: enhanced circulation of antibodies in the fundamental substance; improved blood supply to areas of restriction through the release of histamine; correct orientation of fibroblasts; increased blood supply to the nervous tissue; and greater flow of metabolites from and to the tissue, thereby accelerating the wound-healing process. 7,12,13 However, little information is available on the effect of myofascial techniques on the immunological system.
Suboccipital and craniocervical release techniques are the most widely applied in manual therapy. 3,7,14 –16 Four small muscles between the occipital and axis (rectus capitis posterior minor, obliquus capitis superior, rectus capitis major, and obliquus capitis inferior muscles) control rotary movements of the head and are also related to eye movements, making them a key group of muscles for controlling posture. 17,18
The fascial system forms a set of compartments that envelop, separate, and support the muscles, bones, viscera, blood vessels, and nervous system, and it can be compared to a system of tubes concentrically placed inside one another. Cervical fasciae, which are longitudinally oriented, connect trunk structures with the head. 6 Any change in the reciprocal tension of the connective tissue forming the meninges is a primary cause of craniosacral system dysfunction. 19 Meninges appear to organize and align as the dura mater is exposed to continuous tensions over time, as observed in cadavers 20,21 and living subjects. 2 –7 The fascial tissue of the craniocervical region is connected not only to the skeletal muscle apparatus but also to neighboring organs and viscera. 19 One case study reported incidental findings of biological modifications in a young woman undergoing deep myofascial release. 22
Numerous studies have demonstrated that myofascial induction techniques can modify the sympathetic nervous system. 23 For instance, Arroyo et al. 29 found a higher salivary flow in individuals treated with myofascial induction versus classic massage after induced stress. Fernández et al. 24 observed changes in systolic blood pressure and heart rate in individuals treated with myofascial induction techniques but not in a “simple-touch” group, evidencing a neurovegetative modulation. In addition, activation of the sympathetic system is known to produce immunological changes, 25,26 and variations in immune functions have been described at a very early stage of acute stress. 27 A recent study reported that the effect of myofascial release techniques on salivary immunoglobulin A (IgA) levels was modulated by the attitude of the patient towards massage. 28 The humoral immunologic effects of this therapy were evidenced by analyses of IgA 29 and α-amylase activity 30 in healthy stress-induced individuals after its application.
Massage therapy was found to improve the cellular immunological function in children with cancer, with a greater reduction in heart rate and anxiety after four weekly sessions of massage sessions than after four weekly sessions of rest. 31 A study of adolescents with HIV infection reported an increase in natural killer (NK) cells after 1 month of massage therapy. 32 However, to our best knowledge, no previous study has addressed the ability of myofascial techniques to modulate the cellular immunity response. We hypothesized that myofascial release therapy may modify the expression of certain immunological markers. The objective of the present study was to determine any immediate changes in CD3, CD4, CD8, CD19, and NK cells in the blood of young healthy adults undergoing myofascial induction therapy.
Materials and Methods
Subjects
This study included 39 healthy male adult volunteers, all university students on Health Sciences or Physical Education courses. The mean age was 21.15 years (SD=2.28 years), and the mean number of years of schooling was 13.05 years. Inclusion criteria were male sex, age 18–25 years, performance of sports activity for ≥1 hour at least three times a week, and no previous experience of myofascial treatment. Exclusion criteria were female sex (to avoid bias due to hormonal cycle), receipt of hormone or pharmacological therapy, presence of disease that impedes or contraindicates induction or manipulation techniques or affects study variables (e.g., tumor, fracture, luxation, vertebrobasilar insufficiency, bone disease, skin disorder, fever, cardiovascular disease, or neurological or psychological disorder), any treatment for psychological dysfunction or disease, and the presence of anxiety or depression (see following section for tests and scores applied).
All participants gave their informed consent to participate in this study, which was approved by the ethics committee of our institution. They were randomly assigned to an experimental group for application of myofascial induction techniques or to a control group for a period of rest under the same conditions.
Measurements
Venous blood (20 mL) was collected into heparin-containing (60 USP units of sodium heparin/tube) Vacutainer tubes (Becton Dickinson, Franklin Lakes, NJ) before and after treatment and processed within 3 hours. A flow cytometer (Immunocap®, Uppsala, Sweden) was used to count CD3, CD4, CD8, CD19, and NK cells. Venous blood was drawn immediately before the intervention and at 20 minutes after its completion. The State-Trait Anxiety (STAI) Questionnaire 33 was used to measure state and trait anxiety. The STAI is a 20-item common trait and state anxiety scale developed by Spielberg et al. 33 Respondents use a 4-point scale ranging from 1 (not at all) to 4 (mostly), and higher scores are associated with greater feelings of anxiety. It contains two separate self-evaluation scales and was developed to study anxiety in adults without psychiatric disorders.
Depression was evaluated by using the Beck Depression Inventory (BDI), 34 which is a self-applied questionnaire of 21 items with a greater focus on cognitive than behavioral or somatic components of depression. It is not a diagnostic instrument but provides a measure of the depth of depression in any type of patient (score of 0–9=no depression; 10–18=mild depression; 19–29=moderate depression; and >30=severe depression).
Treatment
The treatment protocol included suboccipital myofascial release (Fig. 1), the so-called “CV4 compression” technique (Fig. 2), 14 and deep anterior cervical fascia release (Fig. 3) as proposed by Pilat in 2003. 7,35 The treatment session lasted for 15 minutes and was performed with the patient in supine position and the therapist at the patient's head. 7 The protocol used is presented in Table 1.

Suboccipital myofascial release technique.

So-called CV4 compression.

Deep anterior cervical fascia release.
Procedure
After randomization of participants into the experimental or control groups, they were instructed to fast during the morning before the intervention and to avoid strenuous exercise for 24 hours before the session. Participants were excluded if they presented with an inflammatory condition that could affect tympanic temperature (e.g., otitis or pharyngitis). Individuals in the experimental group consecutively underwent the three techniques described above. Control subjects remained at rest on the bed for the same time period under identical temperature, humidity, and light conditions.
Statistical analysis
SPSS version 15 (SPSS Inc,, Chicago, IL) was used for the statistical analyses. Data were expressed as mean (±standard deviation [SD]). A multivariate analysis of repeated measures (2 times×2 groups) was applied, based on the general linear model and applying the Grenhouse-Geisser correction, in order to compare the effects of the experimental and control treatments on CD3, CD4, CD8, CD19, and NK cell counts. Based on these results, intergroup comparisons were performed at each time point by means of two ANOVAs, with treatment as independent variable and CD19 count as dependent variable; p<0.05 was considered significant in all tests.
Results
Characteristics of the sample
Table 2 exhibits the main sociodemographic and psychological characteristics of the experimental (n=19) and control (n=20) groups; all subjects were male. No intergroup difference was found in any variable.
BDI, Beck Depression Inventory; STAI, State-Trait Anxiety questionnaire.
Effects of techniques on immunological variables
At baseline, experimental and control subjects did not differ in CD3, CD4, CD8, or NK counts (Table 3). The repeated-measures ANOVA showed a significant time×groups interaction (F 1,35=9.33, p=0.004) for CD19 but not for CD3 (F 1,35=1.75, p=0.2), CD4 (F 1,35=0.81, p=0.38), CD8 (F 1,35=0.04, p=0.83), or NK (F 1,35=0.015, p=0.9) (Table 3). Intragroup analysis showed a higher CD19 count in the experimental group post-intervention versus baseline (t=−4.02, p=0.001), with no changes in the control group (t=0.526, p=0.608) (Fig. 4).
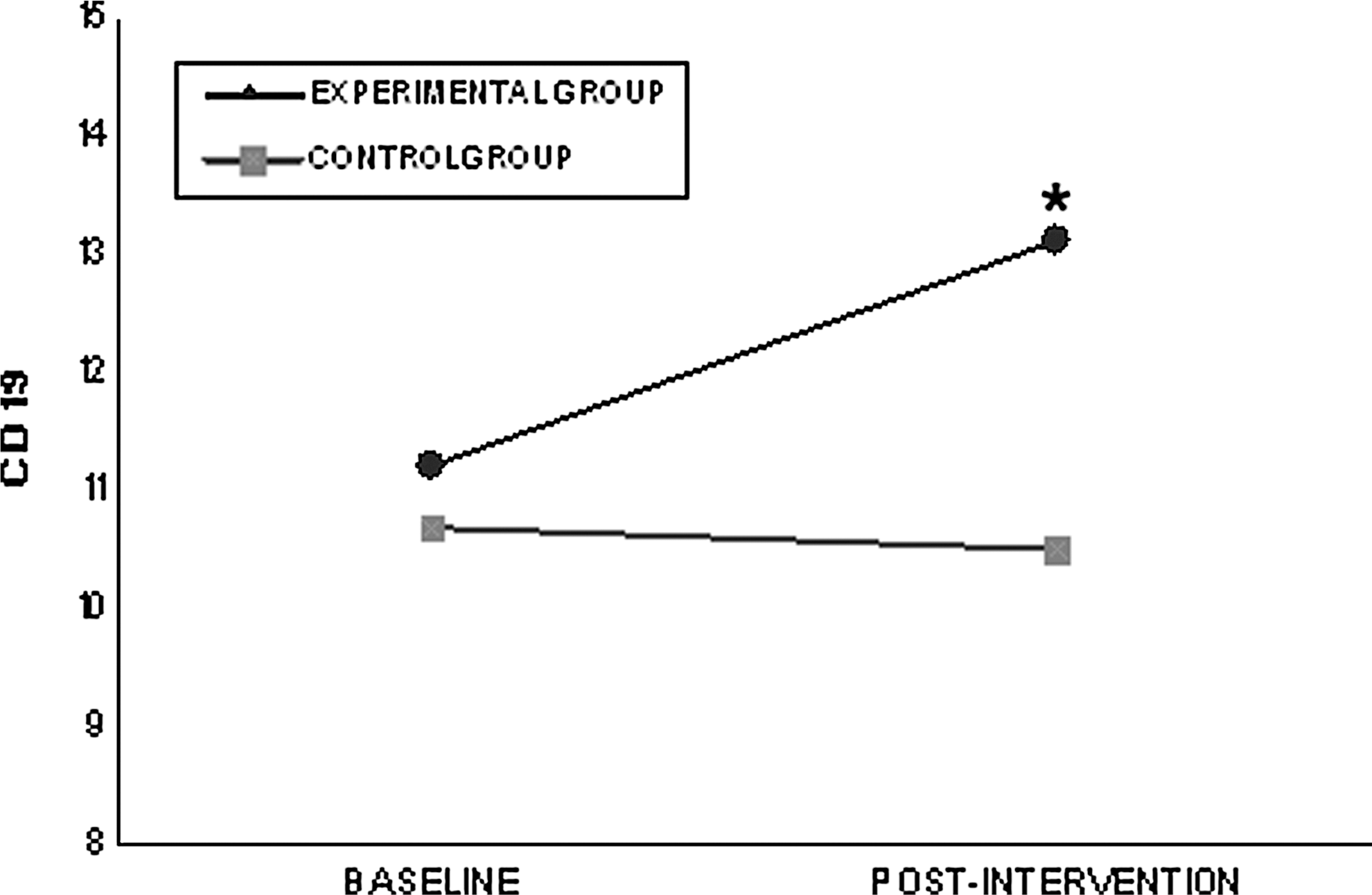
CD19 changes from before to after intervention; *p<0.05 ANOVA.
TG, treatment group; CG=control group.
p<0.05 in between-groups analysis.
p<0.05 in within-group analysis.
p<0.02 in within-group analysis.
The CD count did not significantly differ between the groups at baseline (F 1,36=0.075, p=0.785) but was significantly higher in the experimental (13.1) versus control group (10.5) post-intervention (F 1,36=4.48, p=0.041).
Discussion
This study contributes novel data on the immunological effects of myofascial therapy. Despite the wide application of myofascial techniques in physiotherapy and reports on their effectiveness and physical and mechanical impact on the connective tissue, 5,7,19,36 there has been little research on this therapy from an immunological standpoint. In an earlier study, our group demonstrated that the autonomous nervous system was activated by indirect manipulations believed to compress certain neurological centers (e.g., the fourth ventricle) via suboccipital muscles and anterior cervical fascia. 24 This sympathetic modulation is consistent with the variations in systolic blood pressure and heart rate observed during myofascial treatment. 24 In the present study, we measured T lymphocyte (CD3, CD4, CD8) and B lymphocyte (CD19) differentiation antigens and NK cells to determine whether myofascial therapy also produces modifications in the immune system. We found a higher CD19 count in treated patients than in controls, but no significant differences in any other marker studied. CD19 can amplify or reduce signals generated through the B cell antigen receptor complex in vitro and may be a critical regulator of B cell function. 37 A specific and immediate response of CD19 without the stimulation of other lymphocytes may be associated with a preferential stimulation of B cells, which is a previous step to plasma cell activation. Elucidation of the relationship between the IgA response 29,30 and this CD19 response to myofascial release techniques would improve our understanding of the effects of this therapy. Further research into cell and humoral immunologic responses is warranted to develop our knowledge of the global response of the immune system to myofascial techniques.
B lymphocytes fulfill multiple functions in favor of the immune state and against re-exposure to viruses, bacteria, and certain parasites. They originate and mature in the bone marrow and are then localized in the lymph nodes, where they are activated by the presence of a foreign agent with the assistance of CD4 lymphocytes and/or helper T lymphocytes. However, this assistance may not be necessary under certain circumstances, 38,39 as may be the case in the present study. In addition, immunological values can be modified by a cascade of effects, given that this therapeutic technique stimulates the connective tissue, which in turn modulates the heart rate, systolic blood pressure, and the sympathetic nervous system, 24 suggesting an immediate sympathetic activation with this treatment. 25,27
Given the known relationship between activation of the sympathetic nervous system and immunological modulation, the increase in B-lymphocytes in our experimental group may be due to activation of this system, as evidenced by previous reports of decreased heart rate and systolic blood pressure after application of this myofascial technique. 24
One limitation of our study was the absence of a control group receiving some type of intervention involving physical contact (“simple touch” group). Furthermore, no females were included, and only short-term effects were studied. Finally, caution should be taken in generalizing our results, which were obtained in healthy individuals. Further studies that include females and both touch and nontouch control groups are warranted to investigate the long-term effects of myofascial therapy on a wider range of immunological markers in patients with different diseases.
In this population of healthy young adults, we observed a major immunological modulation, with an increased B lymphocyte CD19 count, at 20 minutes after the application of craniocervical myofascial release techniques.
Footnotes
Acknowledgments
This study was supported by a grant from the Precompetitive Projects of the Vice-Rectorate of Scientific Policy and Research of the University of Granada, Spain.
Author Disclosure Statement
No financial conflicts exist.