
Abstract
Objectives:
The objective of this study was to determine whether giving a massage had an impact of the mental state of the massage therapist.
Design:
The design of this study was a randomized, controlled, blinded study with two parallel groups.
Settings/location:
This study was conducted at an accredited school of therapeutic massage in Dallas, Texas.
Subjects:
The study comprised healthy female and male final-term massage students between ages 18 and 65 years.
Interventions:
The participants were randomized into two groups: (1) the experimental group who gave a 1-hour Swedish massage to a massage client (Massage group), or (2) the control group who sat in a room doing normal, daily activities (Control group). Both these activities were a normal part of the daily routine for these massage students.
Outcome measures:
The primary outcomes were the change in the Depression Anxiety and Stress Scale (DASS) scores pre- and postparticipation.
Results:
Twenty-two (22) participants were randomized in this trial. The baseline characteristics were comparable between the two groups. A statistically significant advantage for the massage group was found relative to the control group in subjective anxiety (DASS Anxiety Subscale, p=0.014). There were no significant differences between the groups with regard to total DASS score (p=0.540), subjective depressive symptoms (DASS Depression Subscale, p=0.472) and subjective stress-related symptoms (DASS Stress Subscale, p=0.919). There were no adverse events reported by any participant.
Conclusions:
This study shows that massage therapists themselves may benefit from giving a therapeutic massage by experiencing less subjective anxiety following the giving of a massage.
Introduction
Since ancient times, touch has been used as a healing tool in all cultures. 3 Yet in the mind of the rational, ocularcentric modern Western individuals, it plays an inconsistent and often confusing role in health and well-being, and as a result touch is often disdained. From birth, touch promotes an infant's neuropsychologic, physiologic, and social development. 4 –6 In later stages as well, touch has been shown to be associated with more satisfactory social relations. 7 Paradoxically, in regard to health and well-being, it is arguably the most important of our basic senses, yet it is least understood.
With touch therapies such as massage, it is impossible to touch without being touched oneself. 8,9 It is precisely this quality that makes the sense of touch unique from any other human sense (e.g., I can see you without you seeing me). Furthermore, as Mazzio 10 describes, the experience of touch often eludes adequate verbal description: “When humans touch, there is a reciprocity of sensation at once physical and psychological that may be felt but not fully grasped.”
It is speculated that through this blurred connection, the giver of a touch therapy also receives a therapeutic benefit. The purpose of this study is to investigate whether giving a massage impacts the state of mind of massage therapists.
Materials and Methods
Objectives
The aim of this study was to investigate whether giving a massage impacts the mental state of a massage therapist, including depression, anxiety, and/or stress. It was speculated that the feelings of depression, anxiety, and stress would reduce following the giving of a massage.
Participants
In this single-blinded, randomized, controlled trial, 22 participants were recruited from a population of final-trimester therapeutic massage students. Volunteers were included if they were healthy, mentally and physically, and aged between 18 and 65 years. They were excluded if they currently had any contraindications of giving a massage (e.g., inflammatory arthritides). Of the 22 volunteers enrolled, 11 were randomly allocated to the experimental group and gave one 1-hour massage. The remaining 11 participants served as controls, and sat in a room for 1 hour.
Interventions
No participants in either arm delivered any form of massage or other touch therapy on the day of their participation, nor did they participate in any practical touch training on the day of their participation. Participants in the experimental group gave one 1-hour Swedish massage to a massage client, which was part of the normal routine for these participants. In all cases, plain massage lotion, free of fragrances and other additives, was used. 11 The control participants sat in a classroom for 1 hour, with no other explicit instructions, which is also normal routine for these participants. It is important to note that the normal routines for all participants were kept unchanged, except for completion of questionnaires before and after the allocated 1 hour. All interventions occurred at an accredited school of therapeutic massage.
Outcomes
The primary assessment measure was the Depression Anxiety and Stress Scales (DASS). The DASS is a set of three self-report scales measuring the affective states of depression (“D”), anxiety (“A”) and stress (“S”). 12 Each of the 21 items is scored from “0” (Did not apply to me at all) to “3” (Applied to me very much or most of the time”). 12 A template was used to score the test, and the total score and three subscores were calculated for each of the subcategories. Subscores can range from 0 to 28+, with normal being at the lower end of the range. 12 The DASS was found to have adequate convergent and discriminant validity 12 and good reliability, including test–retest reliability. 12,13
Sample size
Sample size estimation was performed based on the primary outcome measure, the DASS (total score). The minimum change in the total DASS score of 10 points was predicted using the results from a similar effectiveness studies. 14,15 Using the DSS Research Sample Size Calculator Software and 5% level of confidence, a total of 22 subjects (11 per group) would be required from a statistical power of 0.81. There was no anticipation of any loss-to-follow up and thus no further adjustment for attrition was made.
Randomization and blinding
Participants meeting the eligibility criteria were pooled and randomly allocated to a group by an independent assistant. Randomization took place using sealed opaque envelopes containing group allocation, which was selected for each participant upon enrollment. Only the principal investigator had prior knowledge of the contents of each of the envelopes. Another independent assistant who was blind to the group allocation administered the assessment questionnaires. While it is difficult to blind study participants when hands-on therapies are allocated, in this study this was accomplished because the participants' normal routines were not disrupted. More explicitly, the normal daily activities of these massage students (who were in the phase of their education in which they were actively seeing clients) involved coming in at the start of a shift, and sitting in the student lounge to wait for walk-in clients. Therefore, some of these students were assigned a massage (a normal activity) and some of these students were not assigned a massage (also a normal activity). Due to the normality of these activities, it is believed that all participants were blind to group allocation for the duration of their participation in the study.
Statistical methods
The data were analyzed using SPSS 17.0. The change in DASS subscores pre- and postintervention between the two groups was performed using the nonparametric Mann–Whitney U-test statistics 16,17 to test whether the difference in medians of the two groups is statistically significant. When a difference in the direction of the test statistics is a priori anticipated, a one-tail procedure is implemented. Otherwise a two-tailed procedure is indicated.
Standard protocol approvals, registrations, and patient consents
This protocol received ethics committee approval by the Parker University Institutional Review Board (Approval #R07_10). Also, this study was registered with a clinical trials registry: ClinicalTrials.gov (Identifier #NCT01169480). Written informed consent was obtained from all participants, and all other tenets of the Declaration of Helsinki were upheld.
Results
Twenty-five (25) people were screened, 22 were randomized, and 22 were included in the analysis (Fig. 1, Consolidated Standards of Reporting, or CONSORT, Diagram). The most frequent reason for exclusion was scheduling difficulties (12%). The differences between the groups at baseline were not statistically significant (Table 1). In addition, all participants scored in the “normal” range for all DASS scores.
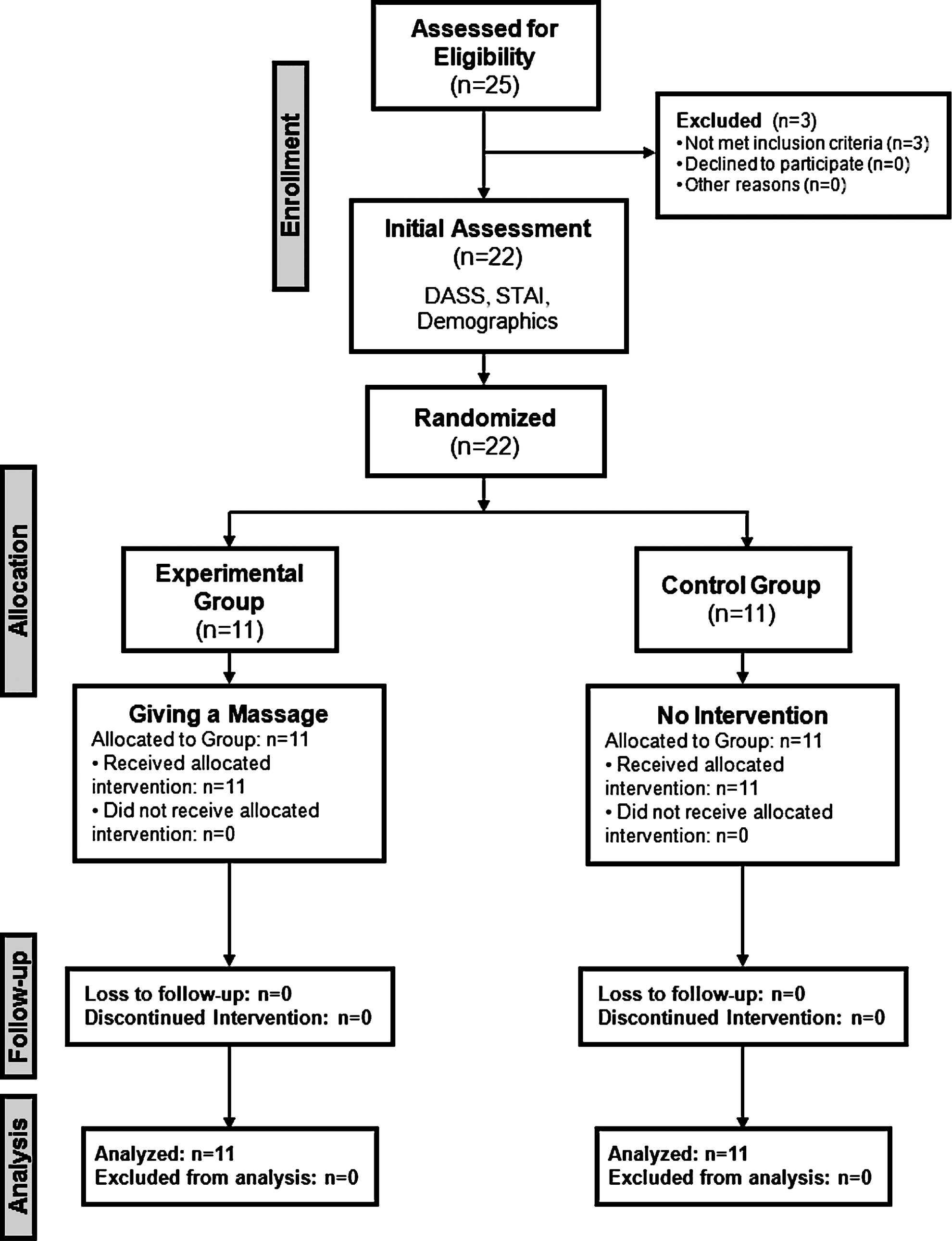
CONSORT Diagram (Consolidated Standards of Reporting Diagram). DASS, Depression Anxiety and Stress Scales; STAI, State–Trait Anxiety Inventory.
p-Value from two-sample test for equality of proportions with continuity correction. Otherwise p-value was calculated using Mann–Whitney test statistics with exact conditional distribution of test statistics. All p-values reported in this table are based on two-sided hypothesis testing.
SD, standard deviation; DASS, Depression Anxiety Stress Scales.
The primary analysis was intention-to-treat and involved all participants (N=22) who were randomly assigned to both groups. Table 2 summarizes the changes in scores from baseline to second assessment (before and after giving a massage or rest). Secondary analyses identified a statistically significant advantage for the massage group relative to the control group in subjective anxiety (DASS Anxiety Subscale, p=0.014). There were no significant differences between the groups with regard to total DASS score (p=0.540), subjective depressive symptoms (DASS Depression Subscale, p=0.472) and subjective stress-related symptoms (DASS Stress Subscale, p=0.919). See Figure 2 for a boxplot of the changes in DASS scores (plus p-values) by DASS category and group, and Figure 3, by group and gender. There were no adverse events reported by any participant.

Boxplot of changes in Depression Anxiety and Stress Scales (DASS) scores by DASS category and group. One value of the p-value from Mann–Whitney test statistics between massage group and controls for each DASS category is shown in parentheses.
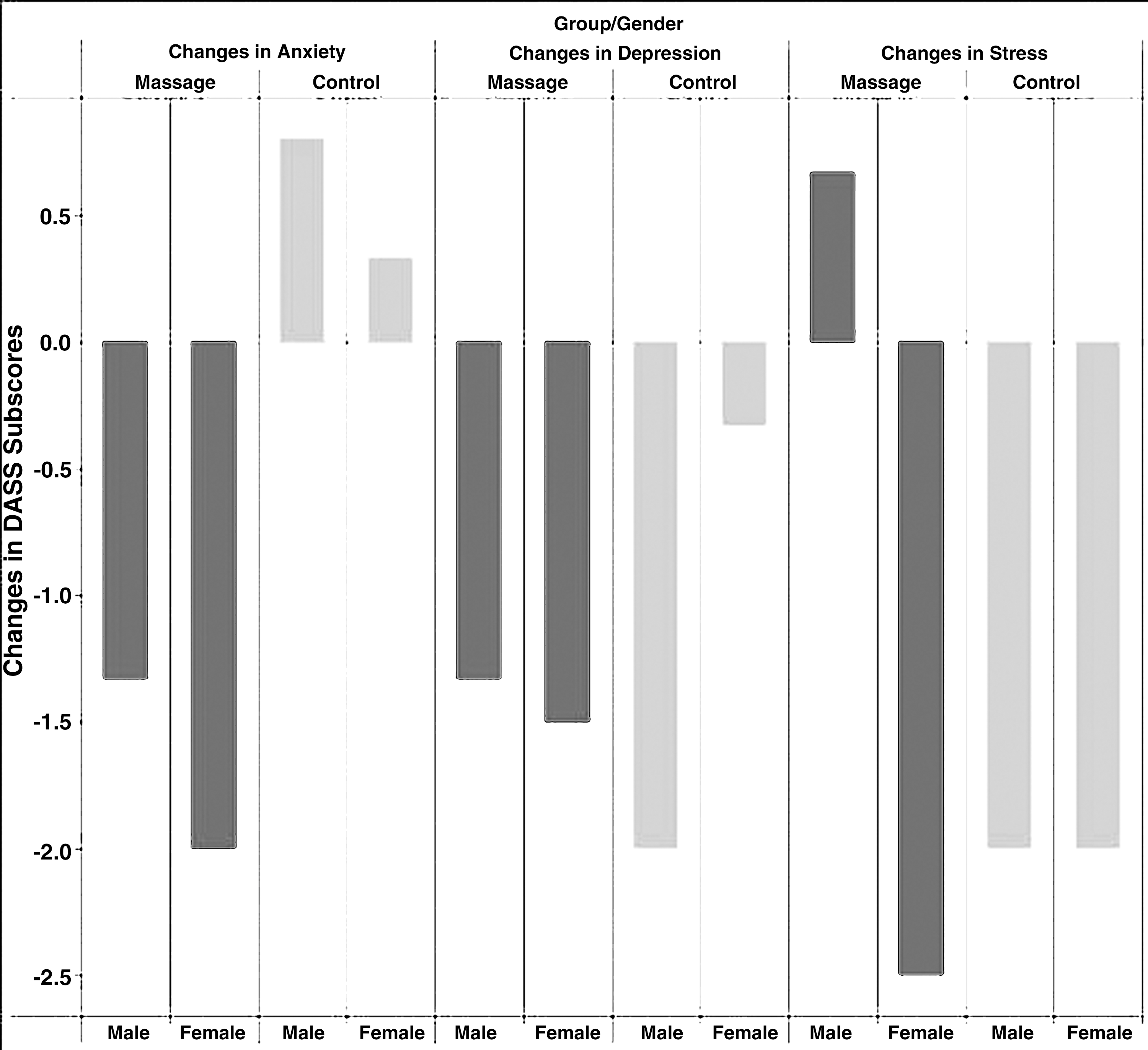
Changes in Depression Anxiety and Stress Scales subscores by group and gender.
Effect size is calculated using Hedges' adjusted g formula which gives an unbiased estimate with small samples sizes.
p-Value from Mann–Whitney test statistics using exact conditional distribution of test statistics. The p-values were calculated under one-sided hypothesis testing for superiority of massage.
SD, standard deviation; CI, confidence interval; DASS, Depression Anxiety Stress Scales.
Discussion
Many studies have examined the therapeutic effect of receiving a massage, and in general have found some benefit. The results of this study suggest that the giver of a massage, the massage therapist, also receives a therapeutic benefit from the experience, in the form of reduced subjective anxiety. The difference compared with a no-intervention control group was large and clinically relevant.
One strength of this study is its uniqueness in the literature. No study published to date has investigated the therapeutic effects for the therapist of giving a massage or other touch therapy. Another strength was its zero-dropout rate. Other strengths are its simple and pragmatic randomized, controlled study design, the careful and clever blinding of assessors and study participants, and faithful adherence to protocols. However, this study also has a number of limitations that must be taken into account.
The main limitation of this study was that it might have been underpowered. Because no prior research on this topic could be found, an adequate estimation of sample size was difficult. It is noted that DASS subscores dropped for both groups, with only the DASS Anxiety subscore achieving significance. In addition, sample size was estimated using only the total DASS score. If estimations using the individual subscores were made and the largest sample size estimation was used, statistical significance might have been reached in other DASS categories as well.
Another limitation of this study is the lack of follow-up assessment, which would have given an indication of the durability of effect. Inclusion of longer-term data would have strengthened the study; however, its feasibility in this or a similar setting is questionable. In a therapeutic massage practice, a therapist would normally massage several people per day for days in succession, and not one in isolation, confounding the long-term effects of giving one massage. Future research may want to investigate the durability of effect.
Finally, the participants were massage students in their last term of training, and therefore, had limited practical experience. They also may have lacked self-confidence. As a result, for some participants, the act of giving a massage may have been stressful, and therefore may have negatively impacted the therapist's mental state. In addition, all massages were also assessed by the massage client, which is also part of the normal routine. However, this may have evoked distress, or a “test anxiety” state. Future research should control for these potential confounders or use experienced therapists. In addition, while the measure used in the study (the DASS) is considered sound, future research may also wish to choose different measures of mental state, such as a different psychometric, or even a physiologic measure, such as a biomarker of stress.
This study may attract criticism for not monitoring or limiting the activities of the control group. However, the activities assigned to both arms of this study (“giving a massage” or “sitting in a room waiting”) were normal daily activity for all participants, and therefore, should not confound results. On the other hand, the addition of an active control condition would have helped tweeze out the therapeutic effects of attention or a specific activity from that of the massage, and therefore, strengthened this study. Such an active control group could simply have observed a massage taking place, had some other nontherapeutic interaction with a client, or attended a lecture.
Other health professionals, such as chiropractors, osteopaths, nurses, and physical therapists, also offer touch therapies. These results may not be generalizable to other groups. Future research on the therapeutic effects of offering touch therapies targeting other health professionals is also warranted.
The purpose of this study was to investigate whether giving a massage impacts the mental state of the therapist. Since these results support the authors' hypothesis and also support anecdotal evidence, speculation about the causation of the benefits is warranted.
The skin is considered the most primitive sense organ, 18 playing an important role in communication and facilitating social relationships. The therapeutic effect of touch is undeniable in all stages of life and for varying conditions. 4,5,19,20 Tactile sensations, as compared to the other senses, are unique in two important ways: (1) They are spread throughout the body, and (2) whoever is touched, touches back. 9 This link between object and subject affords a communication that is nonverbal, allowing each to experience the other's disposition. 9 It is precisely this connection 21 that is speculated to be the basis for the promising results of this trial, the beneficial effect of giving a massage.
Conclusions
This study shows that massage therapists may themselves benefit from giving a therapeutic massage by experiencing less subjective anxiety following the giving of a massage. Additional research is warranted to explore other potential benefits for touch therapists.
Footnotes
Acknowledgments
The authors would like to thank Dr. Lavada Smith for her enthusiasm and her important contributions to this study.
Disclosure Statement
No competing financial interests exist.