
Abstract
Objectives:
Primary dysmenorrhea is a common problem among menstruating adolescents and young women. It may cause physical distress and result in school absenteeism and reduced physical activity. This study aimed to evaluate the effects of auricular acupressure on menstrual pain and distress in adolescents with dysmenorrhea.
Design:
A single-blind, placebo-controlled design was used.
Setting/location:
Participants were obtained from one senior high school in northern Taiwan.
Subjects:
One hundred and thirteen (113) adolescent participants with primary dysmenorrhea were recruited and assigned to the experimental or control group by a coin toss.
Intervention:
The experimental group received auricular acupressure applied to six true acupoints (shenmen, Kidney, Liver, Internal Genitals, Central Rim, and Endocrine). The control group received six sham acupoints without effects on dysmenorrhea. All participants were instructed to press each acupoint for 1 minute, 4 times a day for 2 days.
Outcome measures:
The outcomes were assessed by rating dysmenorrhea severity on a visual analogue scale (VAS) and using the Short-Form McGill Pain Questionnaire (SF-MPQ) and Menstrual Distress Questionnaire (MDQ).
Results:
Between-group differences were found in VAS and MDQ after the interventions. Within-group differences were found in the score changes of VAS, MDQ, and SF-MPQ during the interventions for both groups.
Conclusions:
Auricular acupressure relieves menstrual pain and distress in high-school adolescents. The findings may serve as a basis for using auricular acupressure to treat dysmenorrhea in adolescents. There was pain reduction with sham as well as with true acupoint acupressure, but the latter was significantly greater. The sham acupoint may not be used as a control for auricular acupoint and qualitative evaluation of dysmenorrhea should be added to the evaluation by SF-MPQ in future studies.
Introduction
Nonsteroidal anti-inflammatory drugs (NSAIDs) and oral contraceptive pills are the first-line therapy for dysmenorrhea. 16 –18 However, side-effects of NSAIDs are nausea, vomiting, diarrhea, constipation, rash, headache, drowsiness, allergy, kidney or liver failure, increased risk of bleeding, ulcers, and perforation of the stomach or intestines, 19 while side-effects of oral contraceptives are nausea, headache, breast tenderness, irregular bleeding, and mood changes. 20 Unfortunately, most adolescents experiencing dysmenorrhea self-medicate with over-the-counter preparations, 1 without health professional consultation. 9
Dysmenorrhea can be managed by natural methods without drugs. 21 According to Traditional Chinese Medicine, acupoint stimulation transmits signals to the brain and other organs via nerves and meridians to regulate physiologic reactions. 22 The methods of acupoint stimulation include needle acupuncture, electroacupuncture or laser acupuncture, auriculotherapy, acupressure, and moxibustion. 23 Previous studies have shown that acupoint stimulation may relieve dysmenorrhea. 24 –31 However, the evidence for this is not convincing because of methodological shortcomings, inconsistencies, and small sample size. 32,33 Thus, a more rigorous design to evaluate the effects of acupoint stimulation should be used.
This study was to evaluate the effects of auricular acupressure on menstrual pain and distress in adolescents with dysmenorrhea based on a single-blind, placebo-controlled design. Significant between-group differences in Short-Form McGill Pain Questionnaire (SF-MPQ), visual analogue scale (VAS), and Menstrual Distress Questionnaire (MDQ) scores were hypothesized.
Materials and Methods
Research design and participants
This study was a single-blind, placebo-controlled trial of auricular acupressure for dysmenorrhea in participants recruited from one senior high school in northern Taiwan. Assignment to the experimental group (auricular acupressure at true acupoints) or control group (auricular acupressure at sham acupoints) was by coin tossing for each participant. Only 1 researcher knew the allocation result. Participants and their teachers were not informed about the group allocation. Inclusion criteria were two or more episodes of menstrual cramps in the past 6 months, VAS more than 5 points, holding off taking analgesic medicines or other remedies for dysmenorrhea during the study period, and no ear swelling, infections, or ulcers. Exclusion criteria were pelvic inflammatory disease, endometriosis, and gynecological surgery. Using G Power version 3, the mean±standard deviation of pain (5.26±3.05 in the experimental group and 7.38±3.04 in the control group) was calculated. 3 Each group needed 53 participants to reach a statistical power of 0.80, with the statistical significance of 0.05. Considering an estimated follow-up loss, the required total sample size was estimated at least 112. Data collected before and after the intervention was used to determine efficacy, and efficacy was compared between and within the groups.
Intervention
The experimental group received auricular acupressure applied to six true acupoints (shenmen, Kidney, Liver, Internal Genitals, Central Rim, and Endocrine) indicated by a review of the literature on relief of dysmenorrhea (Fig. 1). The shenmen acupoint was used to alleviate pain and for sedation; 29 Kidney and Liver to normalize qi and blood and thereby restore organ function; 34 Internal Genitals and Endocrine to harmonize and improve endocrine and uterine function; 35 and Central Rim to dredge the meridian and normalize circulation. 36 The control group received auricular acupressure at six sham acupoints (Wind Stream, Esophagus, Trachea, Pharynx and Larynx, Internal Nose, and Tonsil) without effects on dysmenorrhea (Fig. 2). Adhesive plasters were used to stick cowherb seeds to the specific auricular acupoints that affect menses at the onset of menstrual pain. Two (2) experts (licensed doctors of Traditional Chinese Medicine) confirmed the accuracy and precision of seed placement and execution of the pressing techniques. All participants were instructed to press each acupoint for 1 minute, 4 times a day for 2 days from the onset of menstrual pain. The adhesive patches were removed after pressing 48 hours later. Numbness or mild pain and swelling were adverse effects of the pressing procedure.
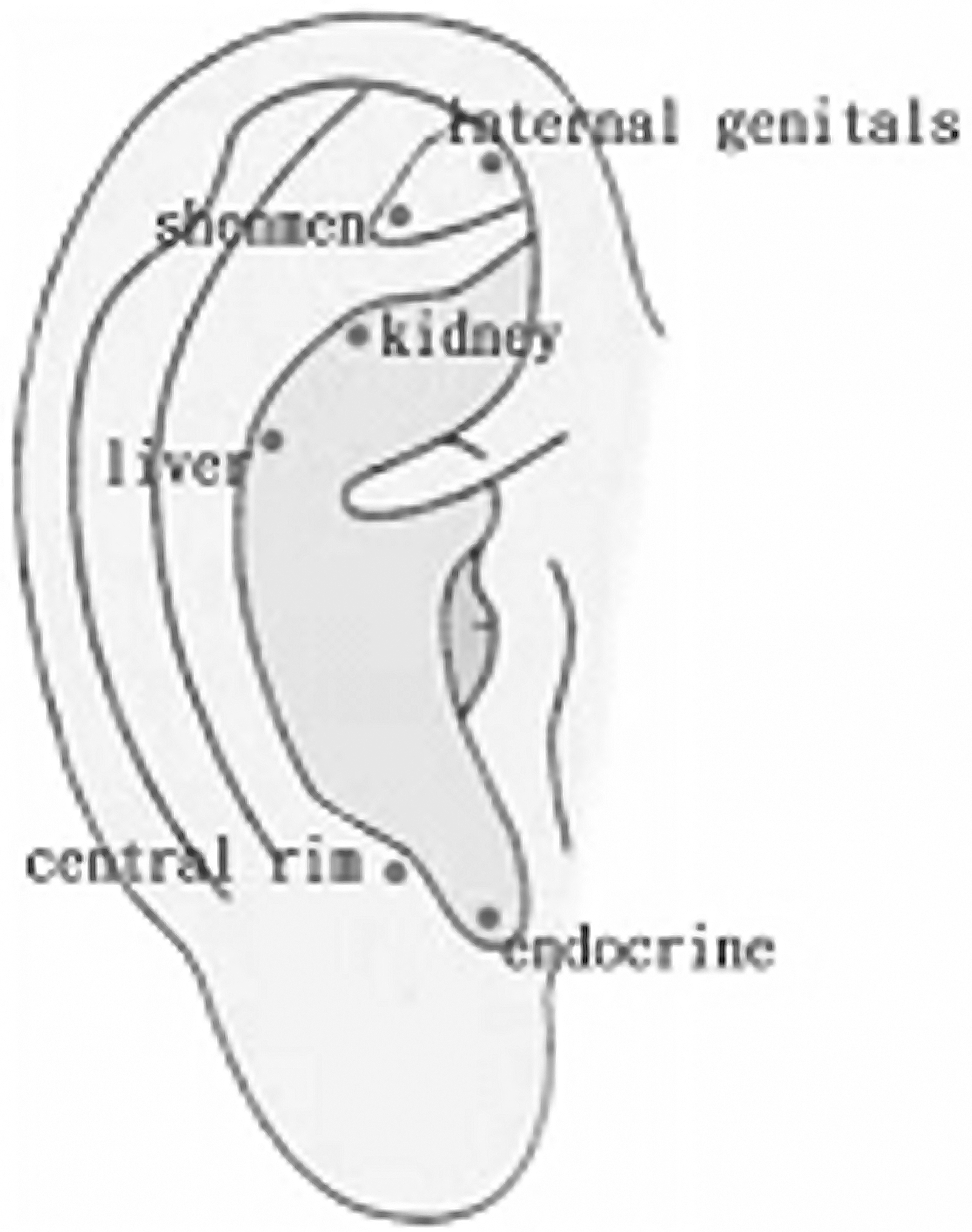
True auricular acupoints for dysmenorrhea.

Sham auricular acupoints for dysmenorrhea.
Measures
Demographic characteristics included age, age at menarche, menstrual cycle duration, menses duration, menstrual regularity, age at initial onset of menstrual pain, and duration of dysmenorrhea. The outcome measures were Short-Form McGill Pain Questionnaire (SF-MPQ), visual analogue scale (VAS) for dysmenorrhea severity, and Menstrual Distress Questionnaire (MDQ) scores. First, the SF-MPQ was used to assess the quality and intensity of pain in 15 descriptive words. 37 This instrument included an 11-item sensory dimension and 4-item affective dimension. Each item was graded on a scale from 0 to 3 (none, mild, moderate, and severe). The maximal score was 45, and higher score indicated menstrual pain of greater intensity. The test–retest reliability was demonstrated for the total, sensory, affective, and average pain scores in patients with osteoarthritis. 38 Cronbach α for internal consistency reliability was 0.84 in this study.
Second, the VAS (which was developed by Huskisson [1974]) 39 was used to self-assess pain intensity. Pain was evaluated on a 100-mm horizontal line with “no pain” on the left end and “unbearable pain” on the right. All participants were instructed to make a mark on the line to indicate their level of pain intensity. Distance from the left end was used to calculate the pain score in millimeters. Last, the MDQ (which was developed by Moos [1968]) 40 contained 47 items related to eight factors (pain, water retention, autonomic reactions, negative affect, impaired concentration, behaviors change, arousal, and control). This study used the modified 16-item MDQ† to grade pain, water retention, and autonomic reactions during premenstrual and menstrual phases on a 4-point scale from 1 (no symptoms) to 4 (severe symptoms). Higher scores signified high levels of menstrual distress. The internal consistency reliability of the modified MDQ was demonstrated,† and Cronbach α was 0.83 in this study.
Procedures and data analysis
Ethical approval was obtained from the high-school administration. All participants and their legal guardians were informed about data collection and management procedures, that the collected data would remain confidential, and that they were free to withdraw at any time during the study. Written informed consent was obtained from all participants and their legal guardians. Data collection started shortly at the onset of menstrual pain before the intervention and each time after pressing an auricular acupoint. SPSS for Windows version 18.0 was used to analyze the data. The χ2 test and independent t-test were used to test the homogeneity of the groups with respect to their demographic characteristics. Independent and paired t-tests were used to compare the effect of auricular acupressure between and within the groups. After adjusting for pre-intervention between-group differences in MDQ score, the analysis of covariance was used to evaluate and compare the postintervention between-group differences. All p<0.05 were considered as statistically significant.
Results
Of the 113 participants recruited (59 experimental and 54 in the control group, respectively), 13 failed to complete the postintervention evaluation process (9 in the experimental and 4 in the control group). Fifty (50) participants remained in each group. The attrition rate was 11.5%. The average age was 17.94±0.84 and 17.78±0.89 at the time of the study and 12.18±1.56 and 11.94±1.11 at menarche in the experimental and control groups, respectively. The mean length of the menstrual cycle was 29.7±4.02 days and the mean duration of menses was 5.24±1.12 days for the experimental group, and 30±3.50 days and 5.72±1.26 days for the control group. In 66%, 35%, and 83% of participants, respectively, menstruation was regular, menstrual pain began one half to 1 year after menarche, and menstrual pain occurred within the first 2 days of menses. Table 1 summarizes the demographic characteristics and shows the similarities between the groups. Table 2 summarizes the results of SF-MPQ, VAS, and MDQ analysis. First, there was a significant between-group difference in SF-MPQ score change (p=0.02) but not in SF-MPQ scores before and after the intervention (p=0.54 versus 0.09). Within-group differences of SF-MPQ were significant in both the experimental (p<0.001) and control (p<0.001) groups. Second, the between-group difference was significant in VAS score after the intervention (p<0.006) and in VAS score change (p<0.002) but not in VAS score before the intervention (p=0.56). A within-group difference in VAS score was significant in the experimental (p<0.001) and control (p<0.001) groups. Last, the between-group difference in MDQ score was significant before the intervention (p=0.03). Thus, adjustment for the pre-intervention MDQ score before analysis resulted in a significant between-group difference in MDQ score after the intervention (p=0.01) and MDQ score change (p=0.001). The within-group difference in MDQ score was significant in the experimental (p<0.001) and control (p<0.001) groups.
n=50 in each group.
n=50 in each group.
Experimental group.
Control group.
SD, standard deviation; diff, difference.
Discussion
In this study, the average age was 12 years at menarche, and the lengths of the menstrual cycle and menses were 29–30 days and 5–6 days, respectively. Most participants had regular menstruation and suffered pain on the first 2 days of the menstrual period. These findings agree with findings of other studies in Taiwan, 41 –44 India, 21 Turkey, 10,45 and Malaysia. 7 In 35% of participants in this study, menstrual pain first started 6–12 months after menarche, which coincides with the onset of regular ovulatory menstrual cycles. 46 Therefore, it is necessary to treat pain in adolescents after menarche as needed.
VAS score analysis found that auricular acupressure has high efficacy in adolescents as a component of treatment for menstrual pain and distress. Similarly, the efficacy of auricular acupoint stimulation to alleviate dysmenorrhea was found to be 99.66% by Xin and 91.7% by Wu et al. 29,30 In addition, Wu et al. found that auricular acupressure for pain in primary dysmenorrhea was more effective than taking pain killers. 29 Kim and Lee also concluded that auricular acupressure provided significant low abdominal and low back pain relief, and relief from autonomic nervous system reactions and negative emotions during menstruation. 47 As previously mentioned, stimulation of the shenmen, Kidney, Liver, Internal Genitals, Central Rim, and Endocrine acupoints can restore qi and blood flow, harmonize endocrine function, dredge meridians, improve circulation, and alleviate pain. In Traditional Chinese Medicine, acupoint stimulation by acupressure is the same as acupoint stimulation by acupuncture. 44,48
With regard to SF-MPQ in this study, the post-test change was less. It was previously used to evaluate phantom limb pain in diabetic patients with amputation due to foot gangrene; the pains of tabes dorsalis and reflex sympathetic dystrophy 49 ; and dysmenorrhea pain. 3,41,50,51 The current findings indicate that SF-MPQ score can serve as a qualitative composite measure of dysmenorrhea severity in future studies.
In this study, auricular acupressure on either the true acupoint or the sham acupoint relieved menstrual distress, but the former was significantly more effective than the latter. Likewise, Wan et al. found superior menstrual distress relief by auricular acupressure at true acupoints compared to acupressure at sham acupoints, 51 whereas Huang et al. 43 showed similar relief of dysmenorrheic symptoms when sham and true acupoints acupressure was compared. Comparing nonspecific auricular acupressure with auricular acupuncture for dysmenorrheic symptoms, Pan found that acupressure had a 90.00% efficacy, 36 and Li and Do found that acupuncture had a 77.78% efficacy. 52
Acupuncture at sham acupoints can elicit a placebo or nonspecific physiologic response; therefore, this study attempted to show that real, not placebo, auricular acupressure is effective. Acupressure at the true acupoints was more effective, although the treatment at either acupoint relieved menstrual pain and distress. Hróbjartsson and Gøtzsche wrote a systematic review of 114 randomized studies in various clinical conditions. 53 They found that placebos seldom had significant, powerful clinical effects, although there was a possible effect on pain treatment as compared with no treatment. The outcome was self-report measures and the result had a possible bias related to the effects of small sample sizes. In addition, treatment expectations and context, prior beliefs, and interactions with therapists seem to contribute to the placebo effect. 44 This study was single-blind and placebo-controlled (i.e., participants were blinded to the procedure assignment and the true and sham procedures were the same in all respects except acupoint location). One more explanation may be that the sham and true acupoints were located very close to each other, and therefore sham and true stimuli may be subject to the same meridian transmission processing. Yeh et al. demonstrated that auricular stimulation at both true and sham acupoints reduced serum cotinine levels, carbon monoxide exhalation levels, and daily tobacco consumption. 23 However, Yeh et al. also found that acupoints stimulation at sham acupoints was significantly less able to reduce pain. 44 Karst et al. found that real and sham acupuncture reduced the perception of pain (which is more or less regarded as a placebo effect), but only real acupuncture increased the pressure pain threshold. 54 Thus, the use of the sham acupoint design in the present study may not have been appropriate. These effects need further study.
This study had some limitations. First, the participants recruited from one school site were not representative of all adolescents experiencing dysmenorrhea in senior high schools, and thus to extensively generalize the results should be of some concern. Second, the improvement in menstrual pain and distress was demonstrated in the short term of current menstrual pain, but nothing can be inferred about this improvement in the long term, such as the next menstrual pain. Third, the data are from self-reports and objective physiologic measurements were lacking. These limitations suggest that studies exploring the effect of this intervention at various sites and for longer periods in adolescents are needed. A more rigorously designed randomized, controlled, double-blind trial is also suggested.
Conclusions
This study concluded that auricular acupressure relieves menstrual pain and distress in high-school adolescents with primary dysmenorrhea. In addition, use of a sham group design showed a clear distinction between true and placebo effects. The effectiveness of acupressure at true acupoints was superior to that of acupressure at sham acupoints. These findings may justify the use of auricular acupressure as treatment for dysmenorrhea in adolescents. Therefore, instead of using sham points, real treatment should be compared to other treatments (e.g., drug or herbal remedies) in future studies of auricular acupressure. Moreover, SF-MPQ was not intended for assessment of dysmenorrheic symptoms alone, because it might not be a sensitive enough instrument for measuring menstrual pain in dysmenorrhea. The use of dysmenorrhea descriptions in combination with SF-MPQ score is suggested in future studies.
Footnotes
Disclosure Statement
None of the authors has any potential conflicting interest in this study.
*
Chang WH. The use of complementary and alternative medicine in the management of dysmenorrhea among female dormitory students [Unpublished master's thesis]. Chiayi, Taiwan: Nanhua University, 2008.
†
Wang H. Study on the factors of menstrual physiological distress of junior and senior high school female students in Hsin-Chu City [Unpublished master's thesis]. Taipei, Taiwan: National Yang-Ming Medical College Institute of Public Health, 1991.