
Abstract
Objective:
The goal of this research was to assess the adequacy of blood pressure (BP) control by applying Chinese herbal fomentation (a type of thermotherapy) at the Yongquan point (K1).
Methods:
A total of 102 patients with hypertension, ages 39–55, were included in this study. After a baseline examination, each enrolled patient participated in one session per day lasting 24 hours for 3 continuous days, during which the Yongquan point (K1) on both sides of the body were fomented (given thermotherapy) with a mixture of Chinese herbs. In addition, 24-hour ambulatory BP (ABP) monitoring (ABPM) was repeated at baseline and on the day after the therapy.
Results:
Patients had significantly lower daytime systolic and diastolic BP post-treatment. There were no significant changes in 24-hour, or night-time systolic BP (SBP), diastolic BP (DBP), or mean arterial BP, and in pulse pressure after therapy. The rate of adverse events was 0.98% in these patients.
Conclusions:
The regimen sustained SBP and DBP control during the day for the majority of patients. This study suggested that a Chinese herbal fomentated at the Yongquan point (K1) of both sides of the body has some hypotensive potential.
Introduction
Blood pressure (BP) profile normally includes a fall in BP during sleep and a surge when awakening. Ambulatory monitoring enables recording of the BP throughout the entire day, while patients engage in their activities. 2,3 Guidelines from major organizations have recommended the use of 24-hour Ambulatory BP (ABP) monitoring (ABPM) at home primarily to eliminate most types of observer bias and the “white-coat effect.” 4,5 Compared with clinic readings, ABPM is a better predictor of target organ damage. 6,7 Variations in the 24-hour BP profile, including the absence of the normal fall in BP during sleep (nondippers), or an excessive surge in BP when awakening, provide additional measures of CV risk. 8 –12
Traditional Chinese Medicine (TCM) is a system of healing that originated thousands of years ago. It has evolved into a well-developed, coherent system of medicine that uses several modalities to treat and prevent illness. It has been demonstrated that stimulating the K1 acupuncture point (Kidney 1; Yongquan) in mice could reduce BP significantly. 13 Antihypertensive effects after Yongquan stimulation have also been reported by Inchauspe. 14 The current study was designed to assess the adequacy of BP control, by applying Chinese herbal fomentation (thermotherapy) at the Yongquan point.
Methods
Study site and participants
This one-armed, open-label, self-comparison clinical study was conducted at the First Affiliated Hospital to Changchun University of Chinese Medicine, in Changchun, Jilin, China, between December 2009 and June 2010. Outpatients with essential hypertension were invited to participate.
Study protocol
The study protocol was approved by the First Affiliated Hospital to Changchun University of Chinese Medicine, and approval was also received from the ethics committee of the hospital.
Protocol summaries were reviewed by the participants, and written, informed consent was obtained on the day of the study, after a detailed explanation of the study purpose and methods was given to the participants.
The inclusion criteria included 140 mm Hg ≤ systolic BP <160 mm Hg and 90 mm Hg ≤ diastolic BP < 100 mm Hg. The exclusion criteria were history of coronary artery disease, heart failure, stroke, or transient ischemic attack, left ventricular hypertrophy, diabetes mellitus (type 1 or type 2), and/or renal failure. Use of conventional biomedical therapy (including hypotensive agents) was allowed to continue during this study.
A total of 102 patients with hypertension, ages 39–55, who met the inclusion criteria, were included (Fig. 1). These subjects were enrolled, clinical BP measurements and blood samples were taken, and the ABPM device was attached to each participant at the next visit. The day after completion of a 24-hour BP recording on the ABPM, the device was removed and the data in each device were noted for each participant.
Flow chart of entry and discontinuation by patients during the study.
After a baseline examination, each patient underwent one treatment session per day, lasting 24 hours for 3 continuous days, during which the Yongquan point on both sides of the body were fomented (given thermotherapy) with a mixture of Chinese herbs, which consisted of: 5 g of Fu Zi (radix Aconiti lateralis preparata); 5 g of Wu Zhuyu (fructus Evodiae spp.); 5 g of Chong Yuzi (fructus Leonuri spp.); 5 g of Luo Buma (Apocynum venetum); and 10 g of Tou Gucao (herba Speranskiae tuberculatae) in a dry powdered form dissolved in fresh warm water (20 mL at 35°C). The 30 g of powder were used for all of the 3 therapeutic sessions. The Yongquan point was identified according to traditional methods; it is located on the midline of the sole of the foot, two thirds going forward from the back of the heel. The applications of fomentation were conducted in the clinic.
A 24-hour BP recording was repeated the day after the therapy. The ABPM recording was performed with a SpaceLabs 90202 or 90207 device (SpaceLabs, Redmond, WA). The study was initiated between 08:30
Before inclusion, all patients had continued on conventional therapy (hypotensive agents). No major changes in hypotensive drugs had taken place during the 1 month before the study, and no alteration was made throughout the study.
The primary endpoints for clinical efficacy were the differences between baseline and post-treatment ABPM measurements.
Statistical analysis
Data on 98 patients who fulfilled all eligibility criteria were included in the analysis (there were 4 dropouts; see Results below). Data missing because to BP ineligibility were considered “missing at random” for the purpose of variance estimation. All BP parameters were analyzed according to the time period: day or night. Data were expressed as mean±standard deviation. Comparisons between baseline and post-treatment were made by paired t-tests. All analyses were performed with SAS, version 8.02 (SAS Institute, Cary, NC). p<0.05 was considered statistically significant.
Results
The baseline clinical characteristics of the participants are summarized in Table 1. Four (4) patients who initially enrolled in the study did not complete the 24-hour ABPM recordings. One patient developed a local, red skin rash 12 hours after the first fomentation. This patient discontinued the therapy. Four days after the discontinuation, the skin rash disappeared. The rate of adverse events was 0.98% in the group. The other three participants discontinued for no therapy-related reasons.
SD, standard deviation; yr, years; BMI, body mass index; GFR, glomerular filtration rate; ACE, angiotensin-converting enzyme; ARB angiotensin-receptor blocker; CCB, calcium-channel blocker; MSSBP, mean sitting systolic blood pressure; MSDBP, mean sitting diastolic blood pressure.
The participants' BP parameters at baseline and post-treatment are shown in Table 2 and in Figure 2. There were no significant changes in 24-hour, or nighttime SBP, DBP, mean arterial BP, and pulse pressure after therapy. However, as shown in Table 2 and in Figure 2, the participants had significantly lower daytime SBP and DBP post-treatment.
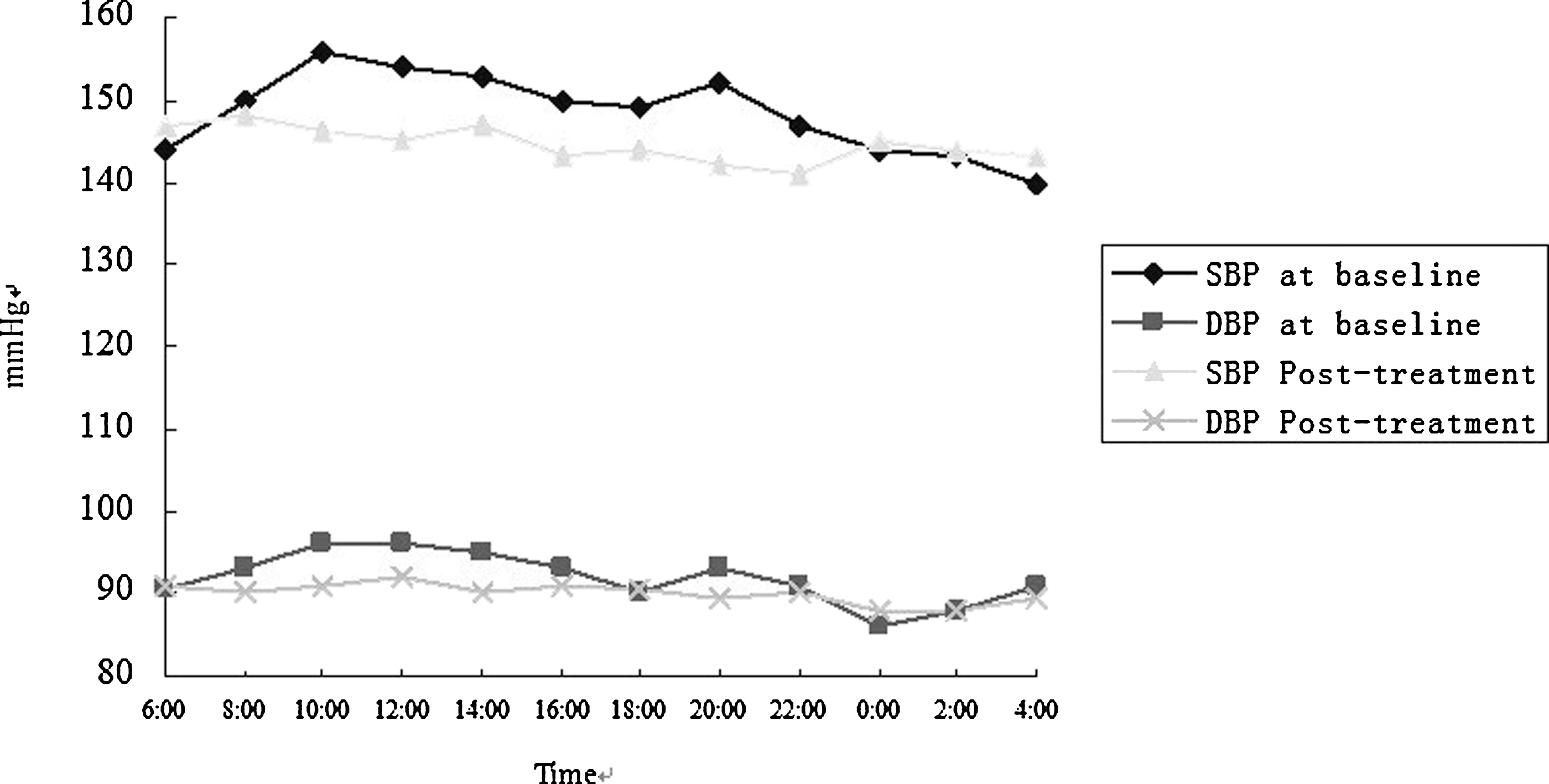
Course of blood pressure (BP) during 24 hours of measurement. SBP, systolic BP; DBP, diastolic BP.
Daytime is when participant was awake.
Night-time is when participant was asleep.
p<0.05.
BP, blood pressure.
Discussion
ABPM has become increasingly important for managing patients with hypertension. 15 –17 Most studies have shown that mean 24-hour ABP is a better predictor of morbidity and mortality than office BP (OBP). 18
A clinically meaningful difference in BP reduction is defined as an absolute DBP reduction of≥3 mm Hg. 19 This is the result of inherent variability in measuring BP with sphygmomanometry techniques, as well as the intraindividual variation in BP. The accuracy of cuff measurements in individual patients, as reflected by the reproducibility of measurements, is limited to ∼ 4 mmHg. In this study, the regimen sustained SBP and DBP control during the daytime (awake) period for the majority of the participants. After fomentation, there was a 6.5 mm Hg reduction in systolic BP and a 4.1 mm Hg reduction in diastolic BP during “daytime,” which suggested that Chinese herbal fomentation at the Yongquan point may have some hypotensive effects. Daytime ABP significantly predicts all-cause and CV mortality, coronary heart disease and stroke, independently from OBP and confounding factors. 20 –22 The, the findings of the current study provided significant prognostic information in the patients with hypertension who participated in this study.
In TCM, hypertension is generally believed to be caused by a disorder of the Liver and Kidney meridians, asthenia of Liver and Kidney Yin, and hyperactivity of Liver Yang as well as an imbalance between Yin and Yang. Liver Yang going in a upward direction in the body leads to Excess in the upper part of the body and Deficiency in the lower part of the body. Chinese herbal fomentation is applied to the Yongquan point to treat the resulting Liver Yang symptoms caused by the upward flowing of Yang qi in order to lead the Liver Yang to flow downward.
Conclusions
This study had several strengths. It was performed in a primary care setting—a setting where high BP was most often diagnosed and managed. BP measurements were executed according to clear and well-described protocols that can be implemented easily in daily practice, using existing BP measurement devices. Fomentation is convenient to implement from a physical perspective, may be well-accepted by most patients, and may have a higher response rate than other kinds of treatments.
This study also had limitations. The research showed that Chinese herbal fomentation has some hypotensive effects when patients are awake. BP is more variable during the day than during the night (sleeping period) because of the physical and mental activity that people engage in, so it is possible that intermittent BP measurements may not capture the true average daytime ABP completely. Night-time BP is likely to be more stable, so intermittent BP measurements may be more representative of the true night-time average BP. Thus, the results of this study need to be proven by other research methods (e.g. continuous intra-arterial ABP recordings). 23 Moreover, some BP influence factors could not be overcome in a one-armed, self-comparison clinical protocol. Controlled trials (especially randomized controlled trials) are required. It would also be desirable to follow a larger number of patients for a longer period of time to determine an appropriate target BP to be achieved.
Even so, the current study suggested that Chinese herbal fomentation at the Yongquan point on both sides of the body has some hypotensive potential.
Footnotes
Acknowledgments
The authors thank all of the investigators and patients who participated in this study, and are are grateful to the monitors and the First Affiliated Hospital to Changchun University of Chinese Medicine, China.
Disclosure Statement
No financial conflicts exist.