
Abstract
Objectives:
Silver has historically and extensively been used as a broad-spectrum antimicrobial agent. However, the Food and Drug Administration currently does not recognize colloidal silver as a safe and effective antimicrobial agent. The goal of this study was to further evaluate the antimicrobial efficacy of colloidal silver.
Design:
Several strains of bacteria, fungi, and viruses were grown under multicycle growth conditions in the presence or absence of ionic colloidal silver in order to assess the antimicrobial activity.
Results:
For bacteria grown under aerobic or anaerobic conditions, significant growth inhibition was observed, although multiple treatments were typically required. For fungal cultures, the effects of ionic colloidal silver varied significantly between different genera. No viral growth inhibition was observed with any strains tested.
Conclusions:
The study data support ionic colloidal silver as a broad-spectrum antimicrobial agent against aerobic and anaerobic bacteria, while having a more limited and specific spectrum of activity against fungi.
Introduction
In spite of these applications of silver as an antimicrobial agent, there has been recent controversy due to the resurgence of silver products in the medical marketplace. The Australian Therapeutic Goods Administration states that there are no legitimate medical uses for colloidal silver, and there was no evidence to support antimicrobial marketing claims. 4 The U.S. Food and Drug Administration banned colloidal silver venders from claiming any antimicrobial therapeutic or preventive value for over-the-counter products containing colloidal silver or silver salts. 5 Antibacterial studies with ionic colloidal silver (ICS) have yielded variable results. 6 –8 If found effective, silver offers an inexpensive alternative to current antimicrobials as well as increasing the treatment options for antibiotic resistant bacteria. 7
Unfortunately, concerns over the efficacy of silver are justified due to the limited work that has been done on truly characterizing the antimicrobial effects of ICS and its spectrum of activity against microbial threats. The goal of this study was to obtain a better understanding of the activity of ICS against a diverse array of microorganisms including bacteria, fungi, and viruses.
Materials and Methods
Microbes and media
Bacteria and fungi used were obtained from Hardy Diagnostics (Santa Monica, CA). Bacterial cultures were the following: Bacillus cereus ATCC 10876, Bacteroides vulgatus ATCC 29327, Clostridium difficile ATCC 9689, Escherichia coli ATCC 10536, Lactobacillus acidophilus ATCC 314, Mycobacterium smegmatis ATCC 14468, Shigella sonnei ATCC 29930, Salmonella typhimurium ATCC 13311, Staphylococcus aureus ATCC 11632, and Streptococcus pyogenes ATCC 49399. Fungal cultures were the following: Candida albicans ATCC 10231 and Cryptococcus neoformans ATCC 66031. Viral stocks, including reovirus (Type 1 Dearing strain), encephalomyocarditis virus (ATCC VR-129B) and vaccinia virus (Copenhagen strain), were kindly provided by Dr. Bertram Jacobs (Arizona State University). Media were obtained from Hardy Diagnostics (Santa Monica, CA).
Ionic colloidal silver (ICS) preparation
ICS preparation was done as per manufacturer's protocol using a SG6 colloidal silver generator from SilverGen, Inc. (Port Ludlow, WA) under constant current and prepared in distilled water. The ICS suspension was 85%–95% ionic and the remainder colloidal particles 0.001-0.005 μm in diameter (as determined by atomic absorption spectrometry and electron microscopy). The parts per million (ppm) concentration of the solution was determined using a Hanna Instruments PWT meter (Woonsocket, RI).
Bacterial growth studies
For aerobic growth, 18-hour cultures (ranging from 1 to 5×108 colon-forming units [CFU]/mL) were diluted into media (1:1000 dilution; TSB) followed by the addition of indicated concentrations of ICS. The cultures were incubated at 37°C with aeration (by continuous rotation) for up to 24 hours. At the indicated times, samples were removed and the bacterial concentration was determined by serial dilutions on tryptic soy agar (CFU/mL media). For cultures that were treated with fresh ICS every 8 hours, the bacteria were pelleted by centrifugation at each time point and resuspended in fresh TSB containing ICS.
For anaerobic growth, similar procedures were done, except using TSB media that was oxygen depleted and grown under anaerobic conditions. The TSB media was depleted of oxygen by adding 0.1 mL Oxyrase for Broth (Oxyrase, Inc., Mansfield, OH) per 5 mL TSB and incubating at 37°C for 30 minutes. Since this is an enzyme-based reaction, the treated TSB was subsequently boiled for 5 minutes to denature any proteins that may affect the ICS. TSB tubes were flushed with nitrogen before incubation, and plating was done on Brucella blood agar with vitamin K and hemin and incubated in anaerobic chambers.
Fungal growth studies
For yeast growth, 18-hour cultures (ranging from 1 to 5×108 CFU/mL) were diluted into Sabouraud dextrose broth followed by the addition of indicated concentrations of ICS. The cultures were incubated at 37°C with aeration for up to 24 hours. At the indicated times, culture samples were removed and the yeast cell concentration determined by serial dilution on Sabouraud dextrose agar (CFU/mL media). For cultures that were treated with fresh ICS every 8 hours, the yeast were pelleted by centrifugation at each time point and resuspended in fresh Sabouraud dextrose broth containing ICS.
Viral growth assays
HeLa cells (ATCC) were maintained as monolayers in Dulbecco's minimum essential media supplemented with 50 μg/mL gentamicin sulfate and 10% fetal bovine serum (Hyclone) (Complete media) in a 37°C incubator containing 5% CO2. Cell monolayers were infected at a multiplicity of infection (MOI)=0.01. At 1 hour postinfection, the inoculum was removed, the monolayer washed, and the Complete media replaced (with the indicated concentrations of ICS). For multiple treatments with ICS, fresh ICS was added to the media every 12 hours. Since virus particles will be present both intracellularly and extracellularly, the addition of fresh ICS was done into the previously treated media rather than replacing the media. Therefore, the indicated ICS concentrations reflect the initial dose. Virus was harvested at the indicated times postinfection by scraping the cells into the media. The virus was released from cells by three cycles of freeze–thawing. Virus titers (plaque forming units/mL media) were obtained by serial dilution of the virus-containing cell lysate and performing a standard plaque assay.
Cell toxicity assays
HeLa cells were maintained as described above. Cell monolayers were treated with the indicated concentrations of ICS. For multiple treatments with ICS, the media was removed every 8 hours and fresh media with the same concentration of ICS added. At 24 hours post-treatment, the media was removed and the cells were treated with trypsin. The cells were stained with trypan blue (HyClone) as per manufacturer's recommended procedure. Cell viability was determined by counting the number of stained cells and the number of total cells using a hemocytometer.
Results
Previous experiments testing the antibacterial properties of colloidal silver were carried out using disk diffusion techniques and did not show silver to be an effective bactericide. 6 This type of assay is limited since it relies on the ability of the substance tested to diffuse into the agar medium, does not allow for continuous monitoring of microbial growth, and does not permit effective retreatment of the sample. For this reason, the assays done in this study looked at the effect of ICS on microbial growth using growth curves in a liquid medium environment. These studies allowed evaluation of the microbial-cidal and/or microbial-static effects of ICS, and application of multiple dosing studies. To obtain a standard curve on the effective antibacterial concentration of ICS using this method, Salmonella typhimurium and Streptococcus pyogenes were treated with various concentrations of ICS. The results demonstrated that ICS was effective at inhibiting the growth of S. typhimurium between 0.75 and 3 ppm for 6 hours after treatment (Fig. 1). By 9 hours, the bacteria were beginning to overcome the inhibitory effects of the ICS at the 0.75 ppm and 1.5 ppm levels. However, at 3 ppm, bacterial replication was still inhibited. For S. pyogenes, similar results were observed. Bacterial growth was substantially inhibited between 0.75 ppm and 3 ppm, but by 9 hours post-treatment, bacterial growth was occurring at 0.75 ppm (Fig. 1). Notably, for both bacteria, at 3 ppm ICS, an approximate 4-log reduction in the bacterial concentration (CFU/mL) was observed out to 9 hours post-treatment.
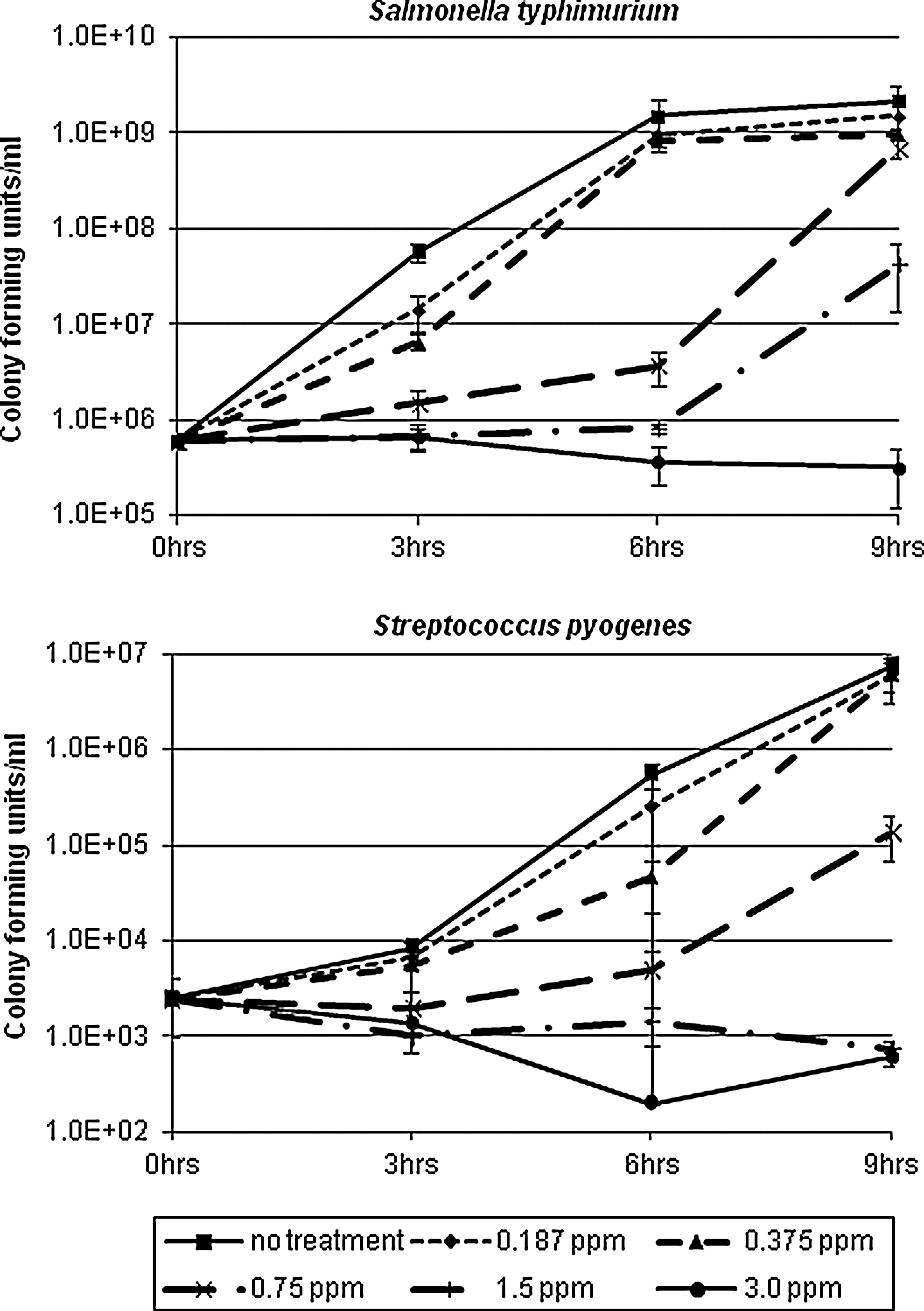
Inhibition of bacterial growth in the presence of increasing concentrations of ionic colloidal silver (ICS). Diluted (1000-fold) bacterial cultures (Salmonella typhimurium and Streptococcus pyogenes) were treated with the indicated concentrations of ICS. The cultures were incubated at 37°C with continuous aeration (by rotation) and colony-forming units/mL media were determined every 3 hours. Assays were repeated in duplicate.
In order to assess the spectrum of antibacterial activity associated with ICS, various bacterial species were chosen based on Gram reactivity, acid-fast positivity, and the ability to form endospores. All assays were done at 2.5 ppm, based on data from Figure 1, and the cultures were treated with either single or multiple-doses of ICS (see Materials and Methods). In all the bacterial species tested under these conditions, an inhibition in bacterial growth was observed with either the single-dose- or multi-dose–treated samples (Fig. 2A). For S. typhimurium, S. sonnei, S. aureus, and S. pyogenes, multiple treatments were necessary to keep bacterial replication inhibited. In the case of M. smegmatis, both the single-dose and multi-dose treatments inhibited replication and yielded similar growth curves. By 24 hours, this bacterium was the only bacterium to show growth in the multi-dose treatment group. For S. typhimurium, S. aureus, S. pyogenes, B. cereus, and S. sonnei, ICS appeared to have a bactericidal effect as indicated by the reduction in bacterial titers at the later time points relative to the initial titer. This effect was most evident following multiple treatments with ICS and ranged from a 10- to over a 1000-fold bactericidal effect (Fig. 2A). This bactericidal effect can be seen more clearly in Figure 2B, where bacterial colonies are observed on the 103 and 105 dilutions for S. sonnei at 0 hours post-treatment, but no colonies are observed on similar dilutions at 16 and 24 hours post-multiple treatments.
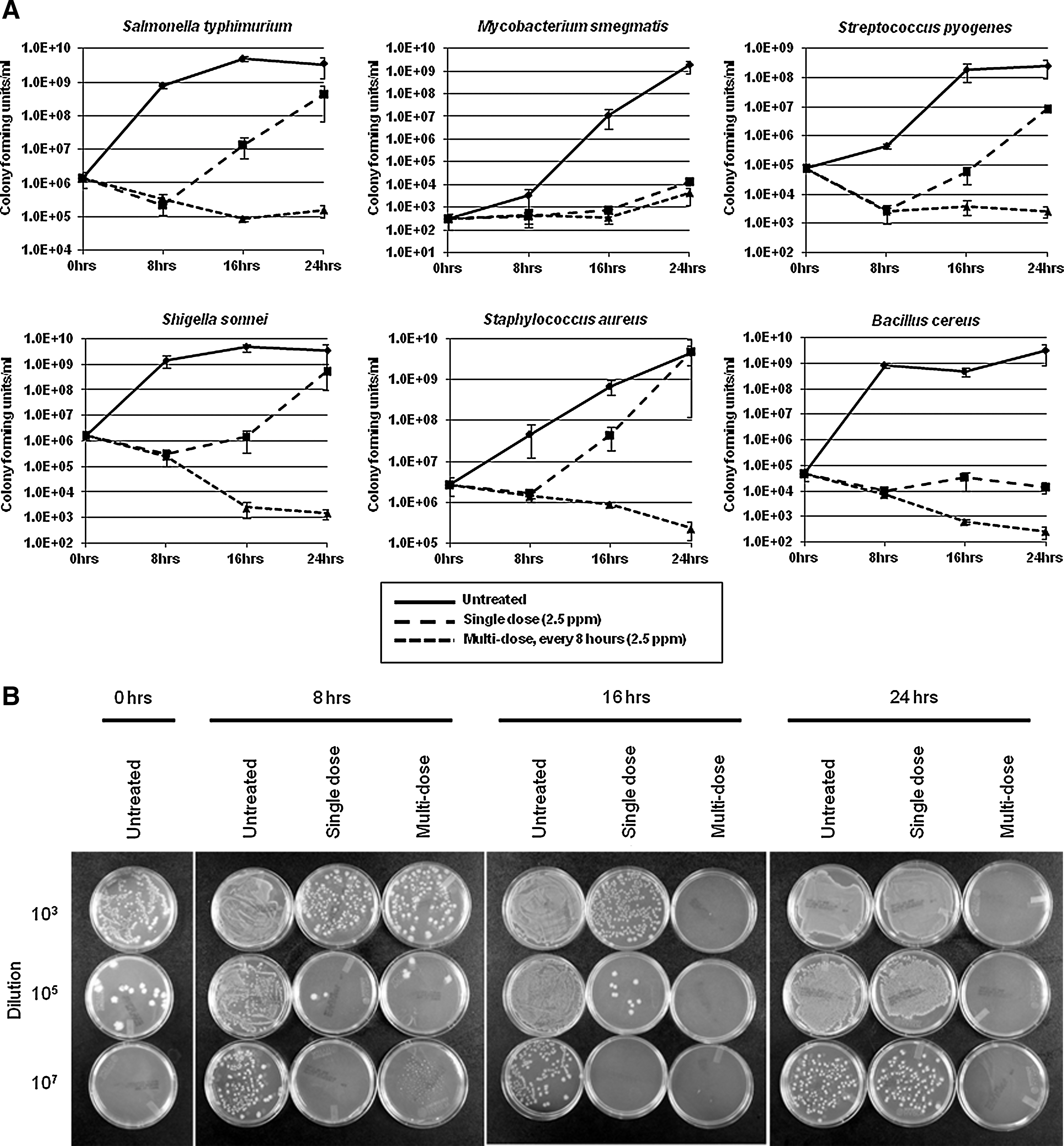
Ionic colloidal silver (ICS) inhibition of bacterial replication under aerobic conditions.
In this study, ICS successfully inhibited the growth of all bacteria tested from 10,000 to 1,000,000-fold with the multi-dose treatment (Fig. 2A). Differences in sensitivity do not seem to correlate with structural differences between the bacteria (i.e., Gram reaction), although the acid-fast nature of M. smegmatis may make it somewhat more resistant to the effects of ICS. These data suggest that ICS is an effective, broad-spectrum antimicrobial agent against bacteria grown under these conditions.
Overall, these results are in sharp contrast to previous studies indicating the lack of efficacy with regard to colloidal silver as an antibiotic. 6,9 In the present study, several bacterial species demonstrated an ability to recover following a single-dose treatment with ICS (Fig. 2A). In these cases, the multi-dose treatment was effective in further inhibiting bacterial growth. In a previous study using a disk diffusion assay with colloidal silver, no inhibitory effect was observed. 6 The lack of effectiveness with this previous study may be due to a multi-dose requirement. Indeed, a previous study using liquid broth bacterial cultures treated with a single dose of colloidal silver suggested that the treatment was relatively ineffective. 9 The mechanism by which colloidal silver may act to inhibit bacterial replication is currently unclear. 8,10 –13 Based on this study's data, it is possible that over time the interaction of the ICS with the bacterium leads to a loss of activity, possibly through oxidation and/or binding up the silver ions/particles.
In order to further assess the antibacterial activity associated with ICS, bacterial cultures were grown under anaerobic conditions in the presence or absence of ICS. Lactobacillus acidophilus is a facultative anaerobic bacterium. L. acidophilus grown under anaerobic conditions exhibited marked inhibition of growth in the presence of ICS similar to that observed with other bacteria in Figure 2A (Fig. 3). This same strain grown under aerobic conditions showed similar growth inhibition following ICS addition (data not shown). To further demonstrate this anaerobic ICS activity, the strict anaerobic bacterium, B. vulgatus and C. difficile, were used. As expected based on the results with L. acidophilus, the growth of B. vulgatus and C. difficile was substantially inhibited with ICS treatment (Fig. 3). Inhibitory effects ranged from 1000 to 1,000,000-fold. For C. difficile, multiple treatments with ICS were necessary to inhibit bacterial growth. For L. acidophilus and B. vulgates, the requirement for multiple ICS treatments to maintain growth inhibition was not as dramatic (Fig. 3). Overall, the data with these bacteria suggest no dependence on oxygen for ICS activity. This supports previous data, which found that the antibacterial activity of silver may be associated with a significant drop in intracellular ATP levels, which is unaffected by the presence or absence of oxygen. 14 In addition, it has previously been shown that silver ions are readily pumped out of healthy bacterial cells with great efficiency. 15 This observation could help explain the requirement for ICS to be administered in multiple treatments to effectively lead to growth inhibition.
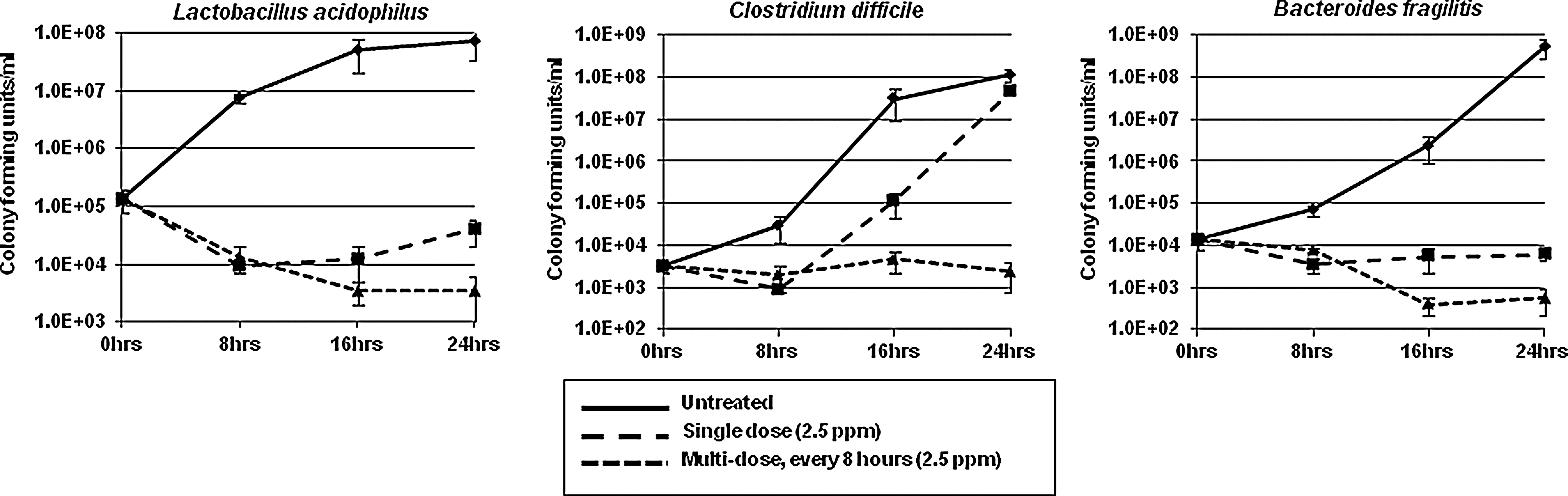
Ionic colloidal silver (ICS) inhibition of bacterial replication under anaerobic conditions. Diluted (1000-fold) bacterial cultures were left untreated (solid line), treated with 2.5 ppm ICS at 0 hours only (long dashed line), or treated with 2.5 ppm ICS every 8 hours (small dashed line). The cultures were maintained and incubated under anaerobic conditions at 37°C with continuous mixing (by rotation) and cfu/mL were determined every 8 hours. Assays were repeated in duplicate.
Historically, ICS has been proposed to have a broad spectrum of antimicrobial activity, not only against bacteria, but viruses and fungi as well. 10 To assess any antiviral activity associated with ICS, distinctly different viruses were grown in the presence of ICS. These viruses varied with regard to genome structure, capsid/envelope structure, and replication mechanisms. Each of these viruses was used to infect mammalian cell monolayers at a low multiplicity of infection (MOI), thereby allowing the virus to spread between cells and complete multiple rounds of replication. As with the bacterial assays, the cell medium was treated with either single or multiple doses of ICS.
As shown in Figure 4, only a minor decrease (2- to 5-fold reduction) in viral titers (plaque forming units/mL) was observed with any of the viruses tested following treatment with ICS. This suggests that ICS was ineffective at inhibiting the replication or spread of any of these viruses. Since this effect could be alternatively explained by a loss of activity of the ICS in the cell culture media by complexing with compounds present in the media, in a separate experiment, the authors demonstrated that Bacillus vulgatus grown in the cell culture media was still sensitive to the inhibitory effects of ICS (data not shown). Previous studies have used silver compounds to treat free virus samples and suggest that silver can attach to viral surfaces. 10,16 –18 In this study's experimental design where the cells were infected at a low MOI, if the ICS affected intracellular virus replication, virus release from the cell, the free extracellular virus, or viral attachment to the cell, a reduction in viral titers should have been observed. Since no effect was observed, the data suggest that ICS did not affect these viruses.

Ionic colloidal silver (ICS) did not inhibit the replication of viruses. Mammalian HeLa cell monolayers were infected with the indicated viruses at a multiplicity of infection equal to 0.01 (1 virus per 100 cells). The cultures were left untreated (solid line), treated with 2.5 ppm ICS at 0 hours only (long dashed line), or treated with 2.5 ppm ICS every 12 hours (small dashed line). The cultures were incubated at 37°C for 48 hours to allow for multiple rounds of viral replication. Viral titers (plaque-forming units/mL) were measured every 12 hours by standard plaque assay procedures. Assays were repeated in duplicate.
Silver proteins have previously been shown to inhibit the free virus of the LIPV strain of smallpox vaccine. 18 With many poxviruses, including vaccinia virus used in the present study, the majority of viral spread from cell to cell is not through the release of free extracellular virus, but requires direct cell–cell contact. 19 If, for poxviruses, silver is only able to inhibit the free extracellular virus, a reduction in vaccinia virus titers may not have been observed in this study's assays. Alternatively, since the previous studies with LIPV were done with silver protein rather than ICS, it is possible that the form of silver used may be important. 18
Regarding the effect of ICS on viruses, it seems, at best, the range of activity is limited to specific viruses. More studies with more viruses and multiple forms of silver would expand knowledge of such specific interactions and activities.
In order to assess the efficacy of ICS toward fungi, and more specifically yeast, cultures of Candida albicans and Cryptococcus neoformans were treated similarly to the bacterial assays described above. For C. albicans, ICS did not inhibit the replication following either a single-dose or multi-dose treatment (Fig. 5). However, a previous study found that silver demonstrated a strong antifungal activity against C. albicans. 20 These assays were done similarly; however the form of silver used was a nano-silver particle suspension in the form of precipitated silver chloride. Again, these data may suggest that varying sensitivity of different organisms to silver depends on the form of silver used. 20
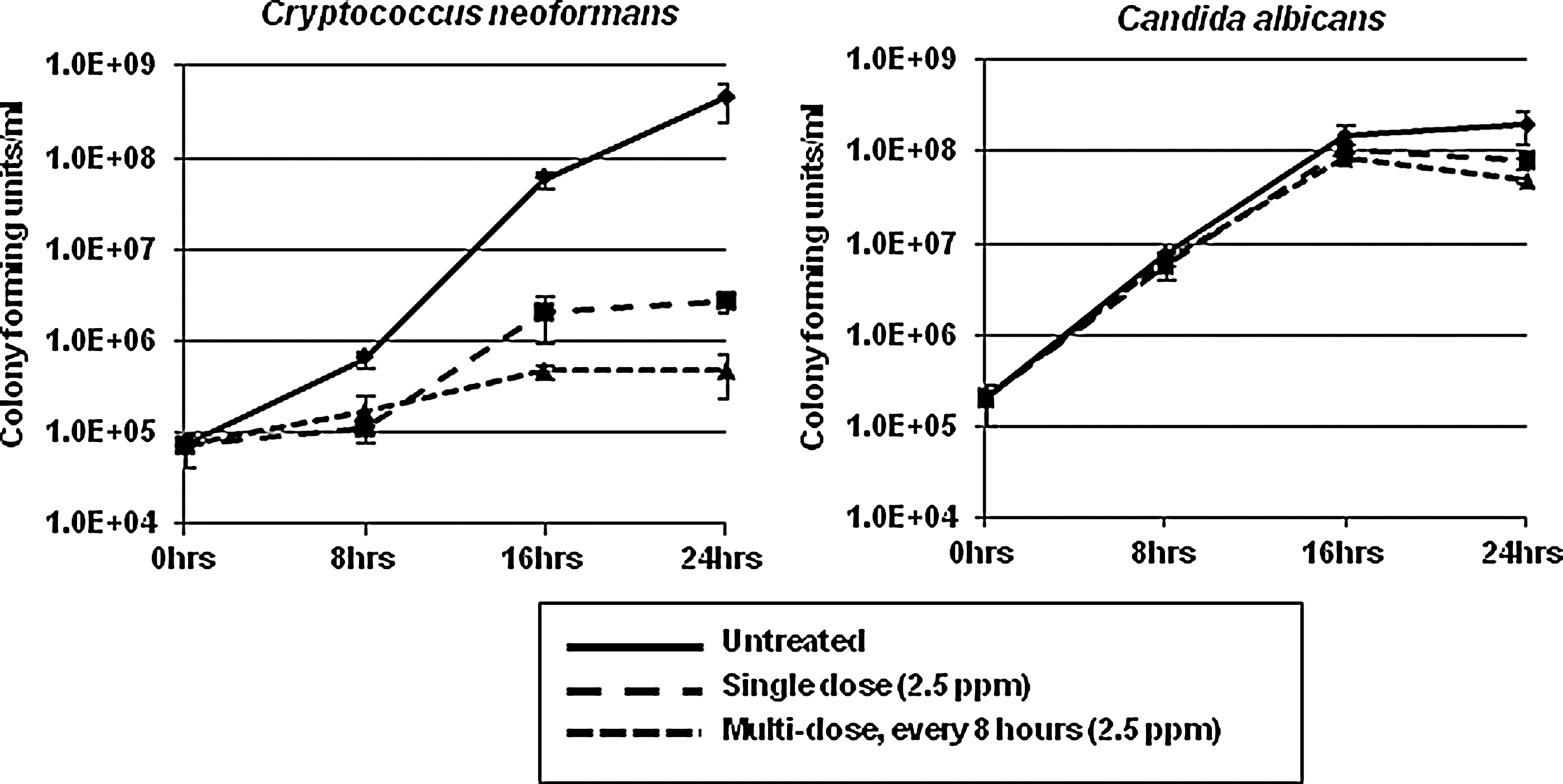
Ionic colloidal silver (ICS) inhibition of yeast replication. Diluted (1000-fold) yeast cultures were left untreated (solid line), treated with 2.5 ppm ICS at 0 hours only (long dashed line), or treated with 2.5 ppm ICS every 8 hours (small dashed line). The cultures were incubated under aerobic conditions at 37°C with continuous aeration (by rotation) and cfu/mL determined every 8 hours. Assays were repeated in duplicate.
In the studies for C. neoformans, a substantial reduction (100–1000 fold) was observed following either a single-dose or multi-dose treatment with ICS (Fig. 5). As compared to Figure 2A, the effect on the C. neoformans was not as strong as the ICS effect on most bacteria. However, a similar inhibitory curve was observed between the single-dose and multi-dose treatments on C. neoformans (Fig. 5), which may suggest that the cellular target for ICS in C. neoformans can be permanently inhibited with a single dose. Since yeast are eukaryotic cells, the cellular target for ICS activity may be completely unique from that of bacteria. Indeed, for C. albicans using nanoparticle silver, it has been proposed that silver may inhibit the normal budding process of the cell by destruction of membrane integrity. 20 Overall, ICS may only target specific genera of yeast, and the antifungal activity proposed for silver may be primarily dependent on the form of silver used.
Very little conclusive research has been done regarding human cell toxicity that may be associated with ICS. 2,10,21,22 In determining human cell toxicity associated with ICS, HeLa cells were treated with increasing concentrations of ICS. As illustrated in Figure 6, minor cell death was only observed at the concentration of 20 ppm following a single treatment of ICS, while substantial cell death was observed at concentrations above 10 ppm with multiple treatments with ICS. Although toxicity was observed, the results demonstrated that at concentrations that effectively inhibited bacterial cell replication, there was little or no human cell toxicity.
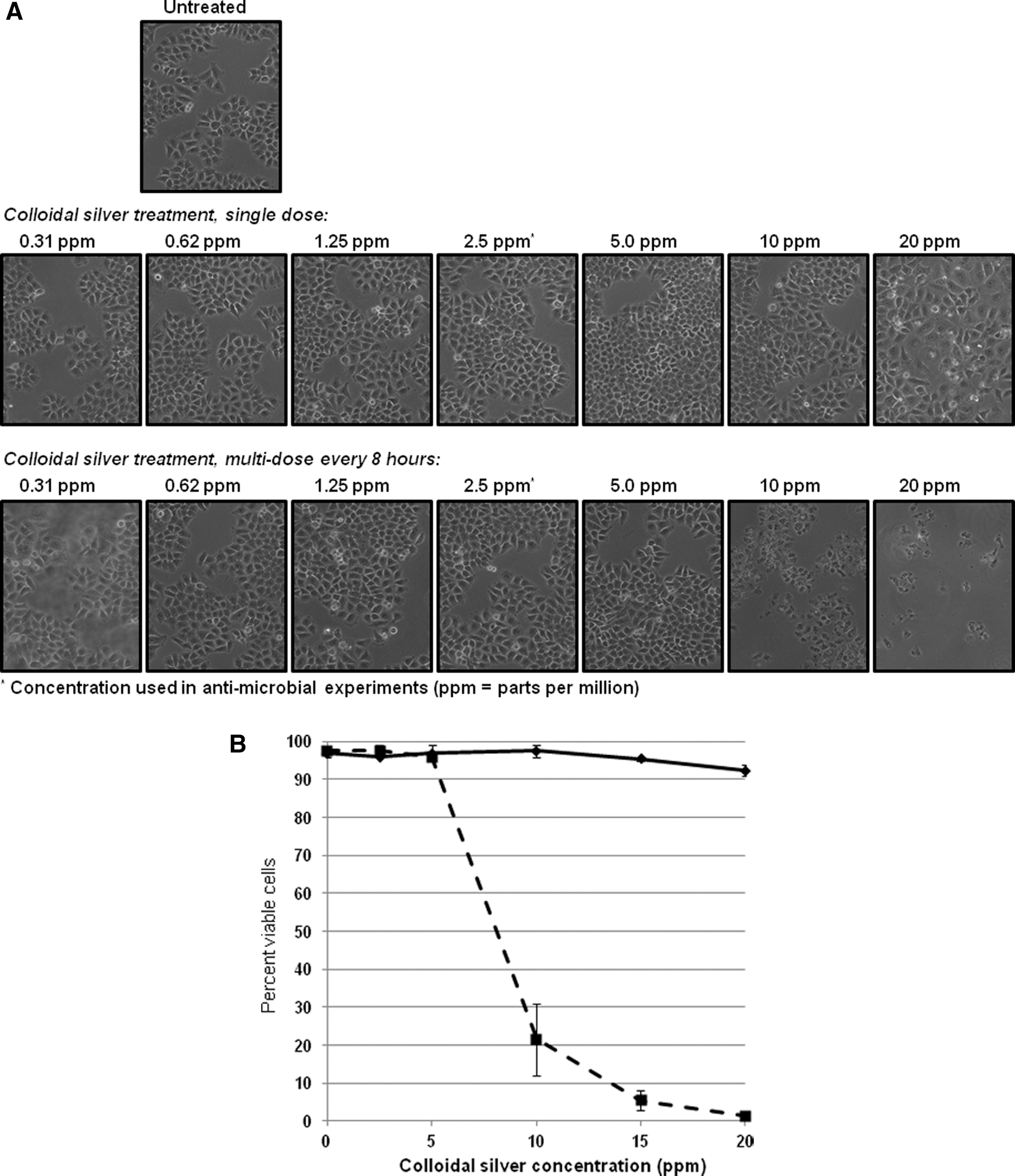
Determination of human cell toxicity associated with ionic colloidal silver (ICS). The mammalian HeLa cell culture line was treated with increasing concentrations of ICS as indicated. Cells were treated with ICS one time only (
Experience has shown that silver compounds are believed safe and effective in controlling pathogenic organisms. 2,10,21,22 Nonetheless, deposition of silver particles in the skin and other organs can result from chronic ingestion or inhalation of colloidal silver, which are non-life-threatening but cosmetically undesirable, leading to argyra. 10 Silver toxicity is rarely reported, and the Environmental Protection Agency's critical dose for an average adult human is equivalent to 21.8 ppm. 10,23,24,25 Based on this, doses that have antimicrobial activity (<2.5 ppm) should be efficacious and have minimal, if any, toxicity in the human host. A typical oral therapeutic dose of ICS is 1 ounce (30 mL) prepared at concentrations of 25–50 ppm (125–250 μg). The quantity of doses generally ranges from 3 to 4 times daily.
Discussion
Currently, with antibiotic-resistant bacteria being a continuing challenge, the interest in understanding the antimicrobial properties associated with silver is increasing. Based on the data in this study, ICS appears to have strong antimicrobial activity against a wide spectrum of aerobic and anaerobic bacteria at low and likely safe concentrations. This has important implications as a therapy, especially for open wounds and possibly oral/gastrointestinal infections. Topically, ICS is commonly applied as a spray or cream on wounds as an antiseptic for control of microbial contamination. ICS has also been widely used for oral/throat infections, including treatment for “Strep throat,” pharyngitis, and gingivitis. Additionally, ICS is commonly used for gastrointestinal infections associated with food poisoning, food-borne illness, and diarrhea. Treatment of these conditions agrees with this study's results regarding the spectrum of bacteria inhibited by ICS. Importantly, these results may suggest ICS as an additional therapy for infections associated with C. difficile.
The use of ICS for deeper-tissue, internal bacterial infections remains more controversial. A major portion of ingested silver is absorbed in the small intestine. Based on animal and human experiments, up to 10% of ingested silver is initially absorbed. 26 Most of the absorbed silver is transported through the blood as a soluble colloid associated with the plasma protein albumin. Following absorption, the highest concentrations of silver are found in the skin, liver, spleen, and adrenal glands, with lesser deposits in the skin and brain. Though representing a single case, ICS treatment was suggested to inhibit the growth of Burkholderia multivorans and clear the infection in a patient with cystic fibrosis. 27 Based on these observations, ICS may demonstrate efficacy in the treatment of internal bacterial infections, although additional clinical studies are needed to verify this concept.
As for additional antimicrobial activity associated with ICS, the picture is more complex and likely limited to specific species of fungi and viruses. Although ICS is commonly used for Candida infections and viral-associated respiratory and nasopharyngeal diseases, clinical studies have yet to be done to support the efficacy in the treatment of these infections. Many physicians prescribe the use of silver for fungal and viral infections; however, the data presented suggest that ICS efficacy is most significantly supported as an antibacterial therapeutic. Arguably, the form of silver used may greatly influence the spectrum of antimicrobial activity. 8,18,22 It is possible that fungal and viral infections may be more sensitive to alternative forms of silver such as silver salts or silver proteins. Further studies need to be done to compare and contrast the efficacy and activity associated with these multiple forms of silver.
Conclusions
Silver was one of the first “antibiotics” in medicine and remains in use in the treatment of various microbial infections, including burns and wound care. It is commonly a constituent in heart valve, orthopedic, and dental prostheses. Historically, colloidal silver use declined markedly following the discovery of penicillin and sulphonamides. With the resurgence of antibiotic resistant pathogenic bacteria, alternative therapies need to be considered. ICS may represent an important asset to the limited repertoire of therapeutics available for these emerging pathogens.
Footnotes
Disclosure Statement
No competing financial interests exist for any of the authors.