
Abstract
Objective:
The ancient Indian medical system, Ayurveda, is the oldest scientifically based system of medicine in the world. According to Ayurvedic concepts, there are 3 humors or Doshas: Vata, Pitta, and Kapha. The combination of these Doshas in varying degrees leads to one's constitution, referred to as Prakruti. Prakruti determines one's physical, physiologic, and mental character and disease vulnerability. This clinical study was undertaken to determine the constitutional typing of individuals with known idiopathic Parkinson's disease (PD) compared with that of nonparkinsonian controls. This study sought to validate the ancient observation that persons of Vata Prakruti are at risk for nervous system diseases. PD was used as a test case because the exact cause is not known.
Methods:
Patients with established PD (n=75) and closely related controls with no known neurologic disease (n=73) were assessed for their Ayurvedic constitution (Prakruti). An Ayurvedic constitutional assessment form and an independent Ayurvedic clinical assessment were used in the patients and controls.
Results:
The total mean score (±standard deviation) for Vata was 11.0±3.9 in patients with PD and 6.9±3.0 in controls. This finding was significant (p<0.0001), indicating that the incidence of PD is highest in those with Vata Prakruti. The incidence of PD was higher in men than in women.
Conclusions:
Knowledge gained from this study may be helpful in identifying the vulnerable population, delaying the onset of symptoms, or slowing disease progression or development of treatment-related complications by keeping Vata in balance through anti-Vata diet and lifestyle changes as prescribed in Ayurveda.
Introduction
In an individual, starting at fertilization, the tri-Doshas work together and maintain homeostasis throughout lifetime. Distinct properties and functions have been ascribed to each Dosha. For instance, Vata contributes to manifestation of shape, cell division, signaling, movement, excretion of wastes, and cognition and also regulates the activities of Kapha and Pitta. Kapha is responsible for growth and maintenance of structure, storage, and stability. Pitta is primarily responsible for metabolism, thermoregulation, energy homeostasis, pigmentation, vision, and host surveillance. Thus, phenotypic diversity, according to Ayurveda, is a consequence of a continuum of relative proportions of the Doshas. 3 Prakruti does not follow Mendelian traits or change with aging. Genopsychosomatic typing of humans consists of common basic birth constitution, which remains stable during one's lifetime. 4 Ayurveda classifies the human population into several constitutional types (Prakruti). On the basis of a patient's history and physical examination findings, an Ayurvedic physician can identify an individual's major and minor Dosha; determine the type of disease vulnerability; and recommend proper diet, lifestyle changes, and treatment, including disease-preventing or -modifying measures.
Apart from genetic influence, a person's constitution is also affected by environment, improper diet, and inappropriate lifestyle, which can cause imbalance of one's Dosha and increase one's vulnerability to a disease to which the person is already predisposed according to his or her Prakruti. In other words, a healthy person has a balance of the 3 Doshas. Any disturbance or imbalance of the Doshas, in which one or the other goes out of balance with respect to the others, results in disease or disorder. According to this system, an individual's basic constitution determines to a large extent predisposition and prognosis of diseases and type of therapy most suitable for that individual's disease. The type of disease, signs, and symptoms depends on the type of disturbance. For example, nervous and mental disorders are said to originate from a disturbance of Vata humor. Vata imbalance predisposes an individual to diseases of the nervous system, chronic pain, cardiac arrhythmia, rheumatic disorders, anxiety, and insomnia. Individuals with Pitta imbalance are predisposed to peptic ulcers, hypertension, inflammatory bowel disease, skin diseases, and allergic reactions. Kapha imbalance predisposes toward diseases of the upper respiratory system, sinusitis, diabetes mellitus, obesity, and cancer. 5
Although this concept of disease prevalence in a particular constitutional type has been known for centuries, it has not been tested with contemporary clinical trial methods. On the basis of the Ayurvedic concept, it is hypothesized that individuals with predominant Vata constitution are at a risk for developing Parkinson's disease (PD), described in Ayurveda as Kampavata. 6 To test the ancient observation, the present study was undertaken to determine the Prakruti of individuals with known idiopathic PD compared with that of nonparkinsonian controls.
Materials and Methods
Patients with established PD from the Plummer Movement Disorders Center, Department of Neurology, Scott & White Clinic/The Texas A & M University System Health Science Center College of Medicine, were recruited after the institutional review board approved the study. Diagnosis of PD 7 (or absence of it in the control group) was established according to the established criteria 7 by a neurologist specializing in PD and related disorders (B.V.M.). For each patient, a sibling acted as a control. In the absence or unavailability of a sibling, the closest adult blood relative was substituted. When such a person was not available, the patient's spouse or a friend acted as the control. The goal was to maintain genetic and environmental commonality as much as possible. Informed consent was obtained from all participants.
Controls were screened for absence of neurologic disorders, including parkinsonism and use of central nervous system active drugs. Demographic data and presence of any known systemic diseases were collected from controls. Presence of systemic diseases was recorded in both patients and controls. The study sample consisted of 75 patients with PD and 73 controls. The mean age (±standard deviation [SD]) of both male and female patients with PD was 70.9±8.8 years; the mean age of male patients with PD (n=42) was 70.8±8.0 years, and that of female patients with PD (n=33) was 71.1±9.8 years. The mean age of both male and female controls was 64.2±12.9 years; that of male controls (n=23) was 67.4±10.3 years, and that of female controls (n=50) was 62.8±13.8 years.
Prakruti of patients and controls were objectively assessed by using an Ayurvedic constitutional assessment form (ACAF; Appendix). This form consisted of 30 questions, including those eliciting the participant's physical features, physiologic features, and mental status. Each of 3 answers would reflect one's Vata, Pitta, or Kapha character. The questions were arranged in a randomized manner to avoid the participant's bias regarding the order of Vata, Pitta, and Kapha segments. The score sheet was coded and calculated independently. From the answers, the number of Vata, Pitta, or Kapha responses was totaled and converted into a percentage to determine various subgroups of Prakruti. Clinical Ayurvedic assessment was performed by a qualified Ayurvedic physician specializing in assessing Prakruti (A.K.). Vata, Pitta, and Kapha scores were rated numerically so that a correlation coefficient could be calculated between ACAF and the Ayurvedic physician's clinical assessment of Prakruti.
From the data generated, a correlation coefficient was calculated to determine validity of the ACAF score compared with assessment by the Ayurvedic physician using GraphPad Prism version 5.04, Graphpad Software, Inc., La Jolla, CA. Means with SDs were calculated. A Student's t test was used to detect statistically significant differences between 2 mean values. P values less than 0.05 were considered to represent statistically significant differences.
Results
The total mean score (±SD) for Vata was significantly higher in patients with PD (at 11.0±3.9) than in controls (6.9±3.0) (p<0.0001). Vata score for male patients with PD was significantly higher, at 10.1±3.7, than for male controls, at 6.1±2.6 (p<0.0001). Vata score was significantly higher for female patients with PD (12.3±3.9) than for female controls (7.3±3.2) (p<0.0001).
In patients with PD, the total mean score (±SD) for Pitta was significantly lower, at 10.9±3.1, than that of controls, 12.8±3.4 (p<0.0005). Pitta score was significantly lower for male patients with PD (11.4±3.1) than for male controls (13.2±3.4) (p<0.05). Pitta score for female patients with PD was significantly lower (10.2±3.0) than that for female controls (12.6±3.4) (p<0.0001).
In patients with PD, the total mean score (±SD) score for Kapha was significantly lower, at 8.1±3.0, compared with the controls' score, at 10.2±2.9 (p<0.0005). Kapha score was significantly lower for male patients with PD (8.5±3.1) than for male controls (10.7±3.1) (p<0.001). Kapha score for female patients with PD was significantly lower (7.5±2.7) than that for female controls (10.0±2.7) (p<0.0001).
Combined (male and female) total scores for Vata, Pitta, and Kapha of controls and patients with PD are shown in Figure 1.
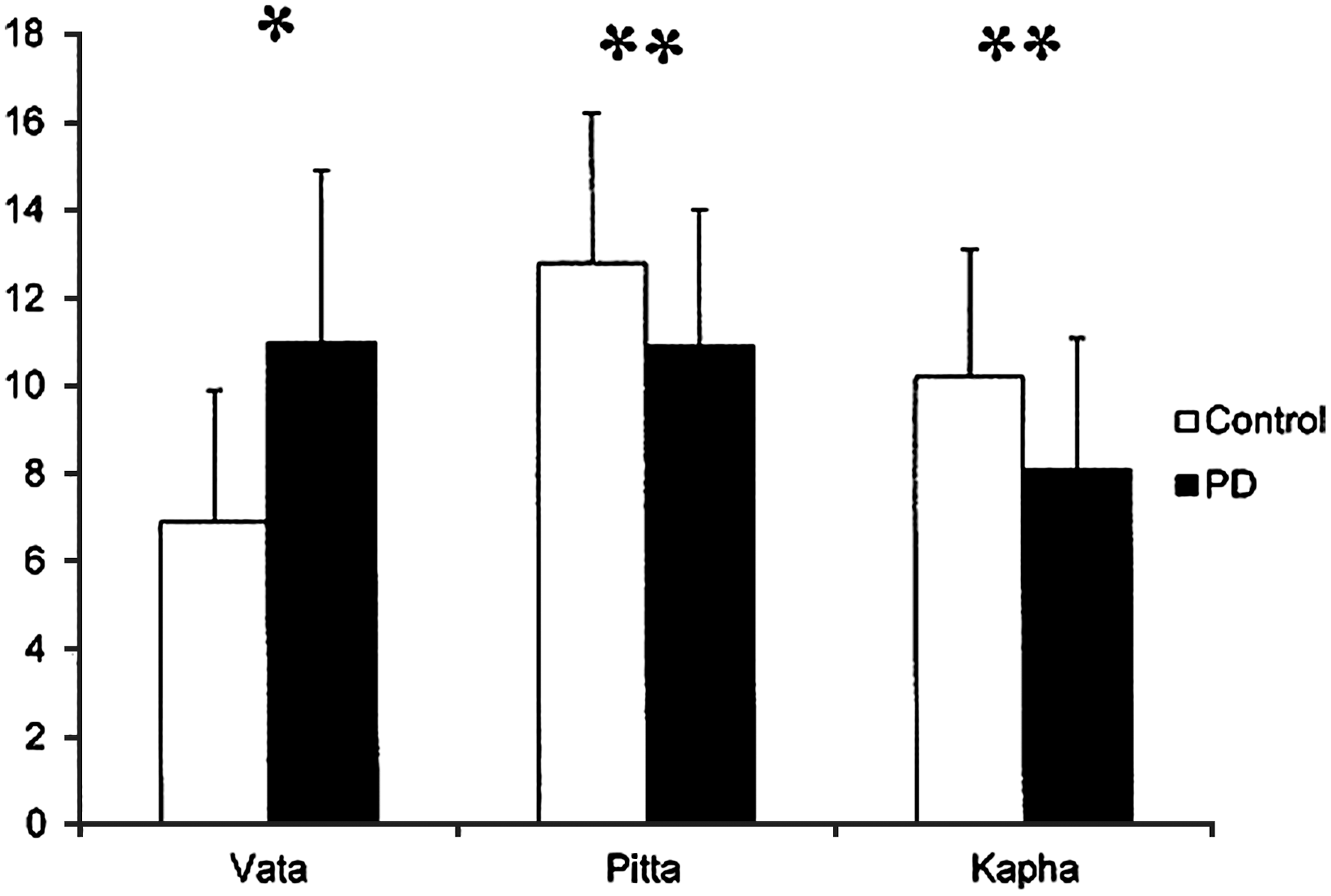
Combined (male and female) total scores for controls and patients with Parkinson's disease (PD) for Vata (p<0.0001)*, Pitta (p<0.0005),** and Kapha (p<0.0005).**
Correlation coefficients were determined between the Ayurvedic physician's clinical diagnoses of the participants' constitution (Prakruti) and the ACAF score. The correlation coefficient was 0.993 (n=148), establishing the validity of the ACAF compared with the independent Ayurvedic physician's clinical assessment.
We used the Vata scores from the ACAF for a substudy based on Ayurvedic risk factors that individuals with Vata component are susceptible to nervous system diseases. 2 If the Vata scores were higher than Pitta or Kapha scores, the participants were subgrouped as Vata major. If their Pitta or Kapha scores were higher than their Vata scores, they were subgrouped as Vata minor. Participants with the lowest Vata scores (i.e., lower than both Pitta and Kapha scores) were not included in this analysis. On the basis of this analysis, the mean age (±SD) of Vata major patients with PD (n=40) was 72.3±1.2 years. The age of the Vata minor PD group (n=18) was 70.0±2.3 years. Table 1 provides the details of all scores. The results show that the Vata scores accounted for 7.3% of Vata major/Pitta minor plus Vata major/Kapha minor (VP+VK) patients in the PD group compared with 28.8% of the nonparkinsonian control group. Further, the VP+VK subgroup of patients with PD made up the highest percentage (53.3%) and the nonparkinsonian controls the lowest (8.2%). When patients with Vata component, major or minor, were compared between controls and PD, the occurrence of PD in the Vata group as major or minor component was significant (p<0.001). When this comparison was separated by sex, the incidence of the disease was much higher in men than in women, in agreement with the higher incidence of PD in men. 8
Unless otherwise noted, values are expressed as the mean±standard deviation. VP, Vata Pitta; VK, Vata Kapha; PV, Pitta Vata; KV, Kapha Vata.
Discussion
The cause of PD is not well understood but probably involves both genetic and environmental factors. 9 Despite a vast literature on lifestyle and possible environmental risk or protection factors, few findings are consistent. There is compelling evidence for protective effects, but the biological mechanisms for these causal relations are poorly understood. 7 Thus, there is a need to explore such biological factors as host vulnerability for developing PD.
Vata Prakruti individuals are known to be lean, with low body weight due to fewer body fat deposits and comparatively lower bone density. 10 Supporting this observation, studies indicate that body–mass index in patients with PD is lower than that of controls, even before the patients developed symptoms. 11 Evidence suggests that a characteristic preexisting personality exists in patients who later develop PD. 12 The personality pattern of individuals with Vata Prakruti seems to fit this observation. The person with Vata constitution has some specific characters, such as disproportionate and underdeveloped general physique; flat and depressed chest; marked prominence of veins; and dry, cracked, and rough skin. Physiologically they have poor appetite, with poor digestion, irregular food intake, less thirst, a tendency toward constipation, disturbed sleep, and low vital capacity. Psychologically they have good short-term memory but poor long-term memory. They have a good mental grasp, a tendency toward mental instability, and a short temper; they are also creative. 13
The knowledge that one's Prakruti predisposes a person to a particular group of diseases is well known in Ayurveda. 5 PD is well described in Ayurveda under the name Kampavata. 2,6 The results of this study, which used PD as a test case, support the ancient Ayurvedic observation that the incidence of PD is higher in individuals with Vata Prakruti than in the other 2 groups. In addition, it showed that the incidence of PD was highest in men, a finding that agrees with current data on the disease. Further studies with more patients are needed to establish this initial observation that individuals with Vata-predominant Prakruti are predisposed to PD.
In conclusion, although the constitutional type (Prakruti) acquired at birth cannot be altered, the Ayurvedic recommendation suggests that vulnerability to diseases based on one's Prakruti can be reduced by following certain dietary and lifestyle changes that are specific for that group of individuals. 10 Further, Ayurveda approaches can balance the imbalanced Doshas by treatment with a specific diet and a procedure called Panchakarma. 14 These approaches can be used before antiparkinson treatment begins, for better results. 15 Knowledge gained from this study may help delay symptom onset, slow disease progression, or reduce development of treatment-related complications by keeping Vata in balance through an anti-Vata diet and lifestyle. 13
Footnotes
Acknowledgments
This work was supported by the Helen Vosburg McCrillus Plummer and Robert Edward Lee Plummer, Jr. Endowed Fund. The authors thank Jacqueline I. Whetteckey, MD, for clinical help and Binu Tharakan, PhD, and Muralikrishnan Dhanasekaran, MPharm, PhD, for statistical support.
Disclosure Statement
No competing financial interests exist.
Appendix: Ayurvedic Constitutional Assessment Form
Medical Records Number: ____________
Code number: ____________
Name: _______________ ____ __________________
(Last) (MI) (First)
Age (in years): □□
Gender: [M] [F]
Code number: ____________
Total each of V(Vata), P(Pitta), and K(Kapha)