
Abstract
Objectives:
The study objective was to evaluate the effectiveness of homeopathic medicines for the prevention and treatment of migraine in children.
Design:
This was an observational, prospective, open, nonrandomized, noncomparative, multicenter study.
Setting/location:
The study was conducted in 12 countries worldwide.
Subjects:
Fifty-nine (59) physicians trained in the prescription of homeopathic medicines and 168 children, aged 5–15 years, with definite or probable migraine diagnosed using International Headache Society 2004 criteria were the subjects in this study.
Interventions:
Physicians were given complete freedom in terms of treatment prescription; thus, prescriptions were individualized for each patient.
Outcome measures:
The frequency, intensity, and duration of migraine attacks in the 3 months prior to inclusion were compared with those during the 3-month follow-up period. Pertinent data were collected using questionnaires completed by the doctor and the patient or his/her parent/guardian. The secondary outcome measure was the impact of homeopathic medicines on education, measured as absence from school.
Results:
The frequency, severity, and duration of migraine attacks decreased significantly during the 3-month follow-up period (all p<0.001). Preventive treatment during this time consisted of homeopathic medicines in 98% of cases (mean=2.6 medicines/patient). Children spent significantly less time off school during follow-up than before inclusion (2.0 versus 5.5 days, respectively; p<0.001). The most common preventive medicines used were Ignatia amara (25%; mainly 9C), Lycopodium clavatum (22%), Natrum muriaticum (21%), Gelsemium (20%), and Pulsatilla (12%; mainly 15C). Homeopathy alone was used for the treatment of migraine attacks in 38% of cases. The most commonly used medicines were Belladonna (32%; mainly 9C), Ignatia amara (11%; mainly 15C), Iris versicolor (10%; mainly 9C), Kalium phosphoricum (10%; mainly 9C), and Gelsemium (9%; mainly 15C and 30C).
Conclusions:
The results of this study demonstrate the interest of homeopathic medicines for the prevention and treatment of migraine attacks in children. A significant decrease in the frequency, severity, and duration of migraine attacks was observed and, consequently, reduced absenteeism from school.
Introduction
Because long-term treatment with allopathic drugs is not indicated for the prevention of migraine, and because recurrent migraine attacks have a significant impact on the personal life, family life, and education of children, the ANAES (now the Haute Autorité de Santé [HAS]) has recommended non-drug-based therapies such as relaxation, cognitive therapy, and behavioral therapy for children and adolescents. 6
The practice of homeopathy has been rooted in medicine for over 200 years. Homeopathic medicines are prepared from minerals, chemicals, plants, or animal matter at infinitesimal dilution. Even if the exact mode of action of homeopathic medicines is not completely explicated, physicochemical study using thermoluminescence showed that the structural state of a solution can be modified by shaking solutes in water and that this modification remains even when the initial molecules have disappeared. 7
Many medical homeopathy monographs advise acute treatment or long-term treatment for migraine attacks. These monographs describe the triggering factors and accompanying signs that are essential factors for individualization of homeopathic treatment.
Recent reviews show a clear increase in the number of individuals accessing complementary and alternative medicine services, including patients with migraine, 8 adolescents, and children. 9
An observational study published in 2001 showed an improvement in migraine or tension-headache symptoms in adult patients (>16 years) treated with homeopathic medicines. 10 Another study on the use of homeopathic medicines for the treatment of chronic diseases reported greater improvements in children, 11 although it was not clear from this report how many children suffered from migraine.
In view of the lack of data on the use of homeopathic medicines for the prevention and treatment of migraine in pediatric patients, we carried out a 6-month observational study on the use of homeopathic medicines for the treatment and prevention of migraine in 168 children, aged 5–15 years.
Materials and Methods
Study design
This observational, prospective, open, nonrandomized, noncomparative, multicenter study was carried out during the first 6 months of 2005. The doctors (general practitioners or pediatricians) who took part in the study were recruited in 12 countries on a voluntary basis. A total of 162 doctors trained in the prescription of homeopathic medicines were contacted. As this observational study was set up to investigate the daily practices of independent homeopathic physicians with regard to the treatment of migraine in children, each doctor was given complete freedom in terms of treatment prescription, and treatment was not dictated by Boiron Laboratories. When IHS 2004 criteria for migraine 5 were present, the prescription of homeopathic medicines was based on the usual criteria used for homeopathic medicines such as triggering factors, concomitant signs, comorbidities, and previous history. As these criteria varied from one patient to another, this resulted in individualized prescriptions for each patient. All homeopathic medicines were fabricated using standard methods of preparation according to current legislation.
Patients
Each doctor was asked to include the first 5 patients for whom homeopathic treatment was prescribed, when they fulfilled the following inclusion criteria: age 5–15 years, diagnosis of definite or probable migraine according to IHS criteria, not receiving any long-term drug treatment, and consent given by a parent/guardian for the child to participate in the study. Patients with epilepsy and patients who interrupted their daily or weekly treatment for at least 10 consecutive days during the course of the study were excluded from the investigation.
The following 2004 IHS criteria were used to diagnose migraine in the children: (1) at least five attacks fulfilling criteria 2 and 4; (2) attack lasting between 1 and 72 hours, with the headache presenting at least two of the following characteristics: unilateral localization; throbbing pain; intensity moderate or severe; aggravated by physical activity; (3) during the headache, at least one of the following characteristics: nausea and/or vomiting; photophobia and/or phonophobia; (4) exclusion by medical history, clinical and neurological examination, and eventually by complementary examinations, of an organic disease that may have caused the headaches. When one of the criteria 1, 2, 3, or 4 was missing, the case was interpreted as probable migraine.
Treatment schedules
The treatments were prescribed during a classic homeopathic consultation through an individualized and holistic approach. There were no predefined treatment or prophylaxis schedules. Data collected by the doctors such as triggering factors, concomitant signs, comorbidities and previous history defined the profile of each patient and enabled the doctor to prescribe specific individualized treatment or prophylaxis in order to decrease the number, severity, and intensity of the attacks.
Data collection
At the beginning of the study, the following data were collected for each patient: the number of migraine attacks in the 3 months prior to inclusion, the duration, intensity, triggering factors, presence of an aura, symptoms associated with each attack, absence from school, and the treatments prescribed.
Intensity was recorded as mild, moderate, severe, or unbearable. Each of these intensity levels was described with the symptoms associated with the attack so that a correlation (and a score) could be established between each level of intensity.
During the 6-month follow-up period, each patient or one of his/her parents completed a logbook recording the duration and intensity of each migraine attack. At the follow-up consultation, the doctors completed a record file for each patient using the information provided in the patient's logbook. Compliance with treatment was also noted at the follow-up visit.
Outcome measures
The primary outcome measure was the frequency, intensity, and duration of attacks. The secondary outcome measure was the impact of migraine on the child's education, measured as absence from school. These criteria were measured at inclusion (for the 3-month period prior to inclusion) and at the 3-month follow-up. All medications prescribed for long-term prevention and/or the acute treatment of attacks were recorded at the inclusion visit. Tolerance to treatment was measured at the follow-up visit.
Statistical analysis
The statistical analysis was carried out on the per-protocol population. Qualitative variables were analyzed using the χ2 test, and quantitative variables were analyzed using the Student's t-test. Alpha risk was fixed at 5%.
Results
Study participants
Fifty-nine (59) of the 162 doctors contacted (36%) took part in the study. The geographic distribution of the doctors was as follows: France (n=27), Poland (n=8), Brazil (n=7), Bulgaria (n=3), Italy (n=3), Tunisia (n=3), Morocco (n=2), Spain (n=2), Hungary (n=1), Mexico (n=1), Romania (n=1), and Switzerland (n=1).
Two hundred and nine (209) patients were included and 168 patient files were analyzed (80%) (41 files were excluded, as the patients were either lost to follow-up or did not fulfill the inclusion criteria). The geographic distribution of the patients was as follows: France (n=53, 32%), Poland (n=47, 28%), Brazil (n=12, 7%), Bulgaria (n=10, 6%), Italy (n=7, 4%), Tunisia (n=12, 7%), Morocco (n=4, 2%), Spain (n=8, 5%), Hungary (n=4, 2%), Mexico (n=2, 1%), Romania (n=5, 3%), and Switzerland (n=4, 2%). The mean age of the children was 11 years, and 60% were female. The mean duration of follow-up was 104 days.
The first migraine attack occurred at 8 years of age on average, and 80% of subjects had already suffered at least five migraine attacks before inclusion. Using the IHS criteria, 77% of subjects were diagnosed with definite migraine and 23% with probable migraine.
Primary outcome measures
Number of migraine attacks
A decrease in the number of migraine attacks was observed between the inclusion and follow-up visits (Table 1). In the first questionnaire, patients reported an average of 10.0 attacks. After 3 months of treatment, the number of attacks decreased from 10.0 to 3.2 (p<0.001) (Table 1). Thus, the number of migraine attacks during follow-up was reduced by two thirds compared to the number before inclusion (Student's t-test, p<0.001).
SD, standard deviation.
Intensity of migraine attacks
The intensity of migraine attacks also decreased significantly during the 3-month follow-up period (p<0.001, χ2 test; Table 1). Over two thirds of patients (66.6%) complained of severe/intolerable headaches at inclusion versus 19.1% at the 3-month follow-up. In parallel, the number of patients with “mild/moderate” headaches increased at follow-up (80.9% versus 33.5% at inclusion) (Table 1).
Duration of migraine attacks
The duration of migraine attacks also reduced significantly during follow-up (p<0.001, χ2 test; Table 1). The percentage of subjects having an attack that lasted >6 hours decreased from 36.5% at inclusion to 13.5% during follow-up, whereas the percentage having an attack that lasted <2 hours increased from 27% to 59.5% (Table 1).
Secondary effectiveness criteria
The percentage of children who took time off from school because of their migraine attacks decreased significantly over the study period from 48.8% of subjects at inclusion to 19.6% during follow-up (p<0.001, χ2 test) (Fig. 1). The mean duration of absence decreased from 5.5 days during the 3 months prior to inclusion to 2.0 days during follow-up (p<0.001, Student's t-test) (Table 2).
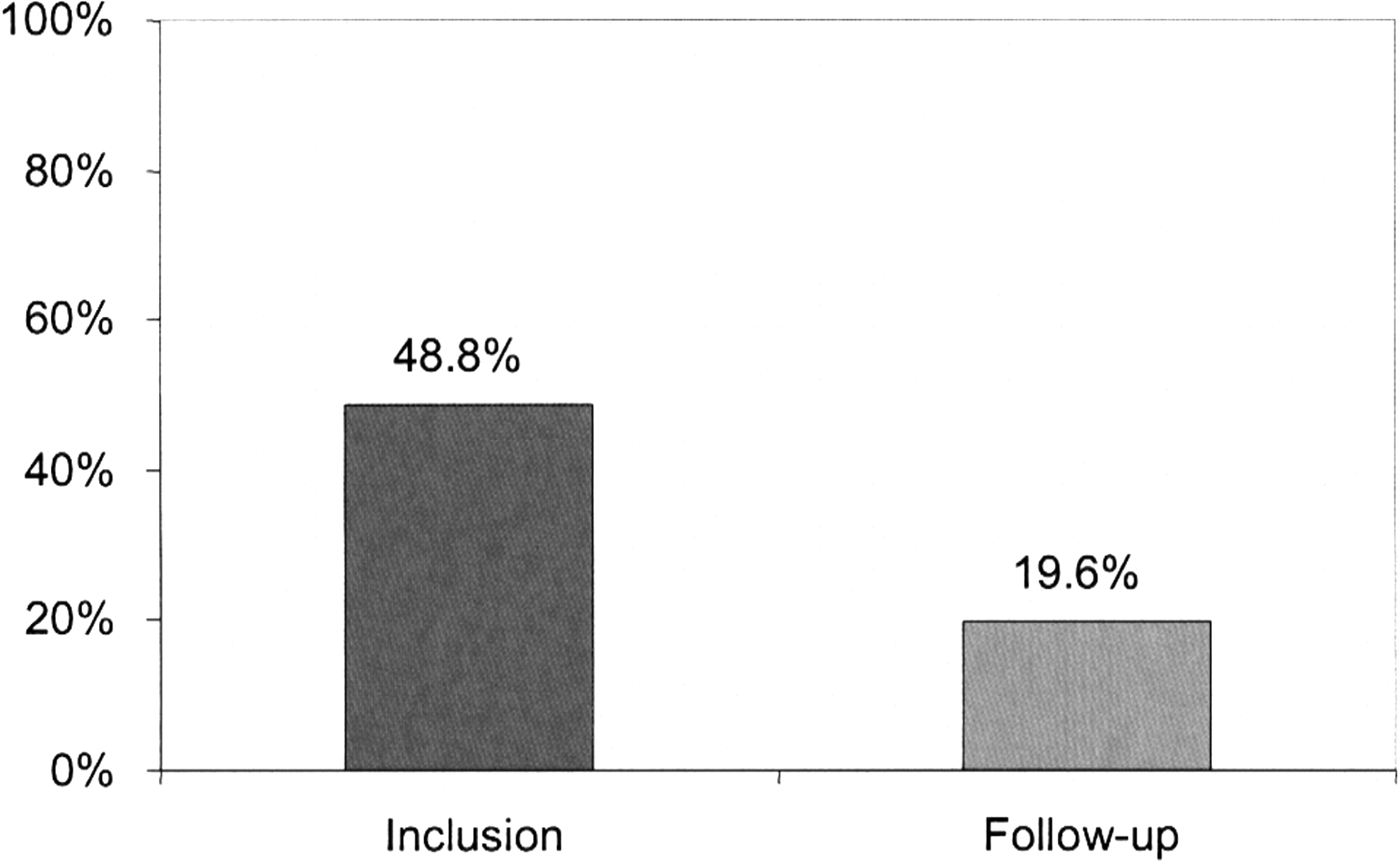
Percentage of subjects who were absent from school during the 3 months prior to inclusion and during the 3-month follow-up period.
SD, standard deviation.
Treatments prescribed
Preventive treatments
Homeopathic medicines were prescribed as preventive treatment in 98% of cases, with a mean of 2.6 medications per patient. In 2% of patients, nonhomeopathic medicines (oligo-elements [trace elements]) were used in association with homeopathy.
The most commonly prescribed homeopathic medicines were Ignatia amara (25%), Lycopodium clavatum (22%), Natrum muriaticum (21%), Gelsemium (20%), and Pulsatilla (12%) (Table 3). Ignatia amara was usually prescribed at a potency of 9C and Lycopodium clavatum, Natrum muriaticum, Gelsemium, and Pulsatilla were prescribed at a potency of 15C. The doses prescribed were usually similar between doctors: Ignatia amara, Gelsemium, and Pulsatilla were most frequently prescribed at a dose of 5 small pills/day, whereas Lycopodium clavatum and Natrum muriaticum were prescribed as 1 dose/week, since the galenic form, dose-globules, was not available in all of the countries involved in the study.
Acute treatment of migraine attacks
For migraine attacks, doctors prescribed either homeopathic medicines alone (38% of prescriptions), allopathic drugs alone (15% of prescriptions), or a combination of both (44% of prescriptions). Thus, homeopathic medicines (alone or in combination) were prescribed for the acute treatment of migraine attacks in 82% of cases. The most common homeopathic medicines prescribed were: Belladonna (32%; mainly 9C), Ignatia amara (11%; mainly 15C), Iris versicolor (10%; mainly 9C), Kalium phosphoricum (10%; mainly 9C), and Gelsemium (9%; mainly 15C and 30C) (Table 4). The allopathic drugs used for the treatment of migraine attacks were paracetamol, ibuprofen, and aspirin.
Tolerance
All medications were well tolerated and there were no side-effects reported at the follow-up visit. All patients complied with treatment.
Discussion
Migraine is the primary headache in children and adolescents, resulting in absence from school due to the severe pain, including abdominal pain, nausea, and vomiting associated with migraine attacks. 12,13 Several drugs have been reported to be effective for the acute treatment of migraine in children and adolescents, including acetaminophen, ibuprofen, intranasal sumatriptan, and intranasal zolmitriptan, 14 but data comparing these different drug classes are scarce. 14 A variety of approaches have also been described for the prevention of migraine headaches in children, including β-blockers, dietary manipulation, pizotifen, progressive muscle relaxation training, stress management, thermal biofeedback, self-hypnosis, and topiramate. 12,15
A benefit of homeopathy was observed for the prevention of migraine. In this study's cohort of 168 children, the frequency of attacks decreased in the 3 months after initiation of homeopathic treatment, and this decrease was statistically significant (p<0.001). Furthermore, the intensity and duration of attacks were also significantly lower than before homeopathic treatment was started, and the children spent significantly fewer days off school (2 versus 5.5 days before treatment, p<0.001). The majority of children (98%) were prescribed homeopathic medicines as preventive therapy, mostly frequently Ignatia amara (25%), Lycopodium clavatum (22%), Natrum muriaticum (21%), Gelsemium (20%), and Pulsatilla (12%) at potencies ranging from 9–15C. Homeopathic medicines including Belladonna (32%), Ignatia amara (11%), Iris versicolor (10%), Kalium phosphoricum (10%) and Gelsemium (9%) were prescribed as acute treatment for migraine attacks. It is interesting to note that 38% of patients were able to manage their symptoms with homeopathic medicines only.
This study has a number of limitations. First, the methodology adopted did not allow individualization of the effects of preventive and curative treatments. Second, these results are based on declarative data reported by the parents during the inclusion visit, and a possible bias of memory should therefore be taken into consideration. On the other hand, in order to reduce selection bias, it was decided to include the first 5 patients who had a consultation and responded to the inclusion criteria. Third, no data were collected for patients who refused to participate in the study. Finally, as the study was noncomparative and did not include a placebo arm, the involvement of the placebo effect is not investigated. A review of previous studies on the homeopathic prophylaxis of headaches and migraine suggests that there is a strong placebo effect in this condition, although the author of this review stated that it was premature to make such a judgment due to the paucity of randomized, controlled trials. 16,17
Unlike randomized, controlled trials, which have a standardized protocol, observational studies allow the effects of individualized treatment to be established and have an important place in establishing a body of proof of the effects of homeopathic medicines in patients with headaches or migraine. 10,11,18,19 However, randomized, controlled trials are important to demonstrate superior efficacy of homeopathic medicines over placebo.
Conclusions
The results of this observational study suggest that homeopathic medicines may decrease the frequency, intensity, and duration of migraine attacks, and may significantly reduce absenteeism from school. Further pharmaco-epidemiological studies and randomized, placebo-controlled trials are required to confirm the clinical benefits of homeopathic medicines in the prevention and treatment of migraine in children.
Footnotes
Acknowledgments
The authors would like to thank Laurence Terzan, Medical Director of Boiron Laboratories, for reviewing the manuscript. This study was funded by Boiron Laboratories.
Disclosure Statement
All authors are employees of Boiron Laboratories.