
Abstract
Objectives:
Ninety-seven (97) undergraduates with a family history of hypertension participated in a study that evaluated the effects of a brief mindfulness-induction on cardiovascular reactivity and recovery to two stressors.
Materials and methods:
Participants were randomized to either a mindfulness-induction or control condition and were then exposed to the cold pressor task (CPT) followed by the mirror-tracing task (MT). Blood pressure and heart rate were measured at baseline and postinduction, as well as during and immediately following each stressor.
Results:
There were no group differences in reactivity to either stressor. Participants in the mindfulness-analog condition experienced significantly greater latency to systolic blood pressure recovery following the CPT and a tendency toward greater latency to diastolic blood pressure recovery, although these findings were not replicated with the MT task.
Conclusions:
These results are contrary to what was hypothesized and to the anecdotal evidence available regarding effects of comprehensive mindfulness interventions on reactivity. The findings are discussed with respect to purported mechanisms of mindfulness and learning theory.
Introduction
Predictors of the Development of Hypertension
It is well established that hypertension is heritable. 4 Furthermore, it has been proposed that the progression from CVR to hypertension may, in part, be moderated by a family history of hypertension. 5 Children of hypertensive parents exhibit heightened SBP and DBP in response to stressors when compared to children of normotensive parents, 6,7 and this reactivity may precede development of hypertension. 8 Children of hypertensive parents may also have greater resting levels of SBP and heart-rate (HR). 6
The ability to recover from a stressor also appears to be related to the development of hypertension. 2 Stewart and France 9 demonstrated that ability to recover more quickly from a stressor was subsequently related to lower levels of SBP. Quick recovery may also be associated with better overall cardiovascular health even when autonomic reactivity is high. 10
Mindfulness and CVR
One technique with potential promise to address reactivity to stress is mindfulness. Derived from Buddhist traditions, the underlying philosophy is to overcome human fallibility (e.g., hatred, ignorance) by centering and focusing attention in a particular way on thoughts, emotions, and bodily sensations. 11 The key features of mindfulness appear to be awareness, acceptance, and labeling of present experience in a nonjudgmental, nonreactive manner. 11,12 Mindfulness may work to increase the ability to become aware of and accept internal experiences, thereby reducing reactivity. Mindfulness appears to reduce perceptions of stressors 13 and tends to decrease ambulatory blood pressure (BP) and HR 14 as well as reactivity to acute stressors. 15,16 Similar results have been found with other meditation techniques, including Transcendental Meditation technique. 17 –19 Research on mindfulness and BP suggests that traditional-length interventions 20 may have a greater effect on these markers than brief mindfulness analog (MA) inductions. Research on brief MA inductions has been limited by small sample sizes, 21 –24 as well as potentially inappropriate comparison groups 15 and inductions. 22 The present study proposed that a brief MA induction addressing these limitations would result in decreased CVR and decreased latency to recovery from two stressful tasks—the cold pressor task (CPT) and mirror-tracing (MT) task—compared to a control group.
Arch and Craske 21 used a brief “focused-breathing” induction as an analog of mindfulness to model an introduction to mindfulness for people without meditation experience. Although not comparable to full interventions, this kind of laboratory induction may be particularly good for examining the mechanisms of mindfulness because it allows for more rigorous control of variables, including individual differences in practice.
The Proposed Study
It was proposed that an MA induction would reduce BP and HR reactivity and latency to recovery from stressful tasks in a sample of college students with a family history of hypertension. Individuals with family history of hypertension are at increased risk for developing hypertension and express greater reactivity in response to stressors. 6,7 As reactivity may precede the development of hypertension in those with a family history of hypertension, 9 ameliorating this reactivity may reduce progression toward cardiovascular disease states, including hypertension.
Materials and Methods
Participants
Ninety-seven (97) undergraduates (53.6% female) were recruited from the research participant pool of a large northeastern university (see Table 1 for a breakdown of descriptive variables by condition). Eligible participants were required to: (1) be at least 18 years old, (2) be able to sit quietly for 20 minutes, (3) have minimal experience with meditation, (4) have no history of frostbite or any other skin condition that may interfere with the CPT, and (5) have one or more first-degree relatives with hypertension.
BMI, body-mass index.
Demographic information was collected on participants' gender, race/ethnicity, age, education, religion, marital status, and height and weight via self-report measures. Participants were then randomly assigned to either an experimental MA induction or a control condition. The MA induction was a focused-breathing exercise adapted from the mindfulness-based stress reduction work of Kabat-Zinn 25 and included instructions such as “If you notice your attention getting away from your breath, gently guide it back to your breathing.” In the control condition, participants listened to the beginning portion of an audiobook, Harry Potter and the Sorcerer's Stone, because the narrator of this book has a soothing voice and the content is not overly stimulating. 22 This was to control for the effects of time and minimize any extraneous emotional valences that might cause arousal. A behavioral manipulation check was administered and assessed by the experimenter during the induction, whereby participants were instructed to raise their hand to the tone of a bell at regularly scheduled intervals to indicate whether or not they were adhering to the manipulation or paying attention to the audiobook (instructions modeled from Frewen et al. 26 ).
Following the induction, participants underwent two consecutive stressful tasks. The CPT (modeled from Baeyer et al. 27 ) was administered first, followed by the MT task (modeled from Frazer et al. 6 ). Participants in the MA condition were instructed to employ the strategy they were taught during the induction throughout the course of both the CPT and MT tasks. Participants in the control condition received no such instructions.
Measuring reactivity
HR and BP were measured during six distinct time periods: initial resting period (baseline), immediately following the induction, during the CPT (reactivity), recovery from the CPT, during the MT task (reactivity), and during recovery from the MT task. Each period consisted of three readings of HR and BP. For baseline, postinduction, and reactivity, the three readings taken during each period were averaged for SBP, DBP, and HR, respectively. 28 A change score was calculated by subtracting the average reactivity reading from the average baseline reading.
Results
Descriptive statistics and preliminary analyses
Preliminary analyses were conducted to evaluate whether the MA and control groups varied on demographic variables of gender, ethnicity, body–mass index, and age. Groups were also compared with respect to their baseline SBP, DBP, and HR, as well as adherence to their induction. Conditions differed on degree of adherence to the induction and minority status. These differences were controlled in subsequent analyses where appropriate. See Table 2 for correlation coefficients between baseline and subsequent physiologic readings and Table 3 for readings of SBP, DBP, and HR at each time-point by condition.
CPT, cold pressor task; MT, mirror-tracing task; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate.
Postinduction period.
CPT reactivity period.
CPT recovery period.
MT reactivity period.
MT recovery period.
SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; CPT, cold pressor task; MT, mirror-tracing task.
Physiologic reactivity to CPT and MT
To test the hypothesis that participants in the mindfulness condition would experience reduced reactivity to the CPT and MT compared to those in the control condition, one-way analyses of covariance (ANCOVAs) examining induction (mindfulness versus control) were performed with the reactivity change score as the dependent variable.
Examination of assumptions of normality of sampling distributions, linearity, homogeneity of variance, homogeneity of regression, and reliability of covariates suggested these were all adequate. There was no significant difference between the two conditions on reactivity to the CPT on measures of SBP, F(1,92)=0.57, p=0.45, ηp 2=0.01; DBP, F(1,92)=0.05, p=0.83, ηp 2<0.01; or HR, F(1,92)=0.05, p=0.82, ηp 2<0.01. Moreover, there was no significant difference between the two conditions on reactivity to the MT on measures of SBP, F(1,93)=0.11, p=0.74, ηp 2<0.01; DBP, F(1,93)=0.02, p=0.89, ηp 2<0.01; or HR, F(1,93)=0.41, p=0.53, ηp 2<0.01.
Recovery from the CPT
To test the hypothesis that participants in the mindfulness condition would have reduced latency to recovery after the CPT compared to participants in the control condition, a 2×3 repeated-measures ANCOVA was performed on cardiovascular recovery to the CPT with group status and 1-minute intervals of time up to 3 minutes as the independent variables. CPT immersion time was added as a covariate because immersion time varied widely and can determine degree of reactivity. Respective baseline physiologic indices (SBP, DBP, or HR) were also added as covariates to maximize power.
There was a significant main effect of condition on SBP, F(1,91)=4.13, p=0.043, ηp 2=0.04, indicating that condition had an impact on SBP recovery from CPT (Fig. 1) with the MA condition experiencing increased latency to recovery compared to the control condition. There was no significant main effect of condition on DBP, F(1,91)=2.00, p=0.16, ηp 2=0.02, indicating that condition had no impact on DBP recovery from the CPT. There was no significant main effect of condition on HR, F(1,91)=0.47, p=0.49, ηp 2=0.005, indicating that condition had no impact on HR recovery from CPT.
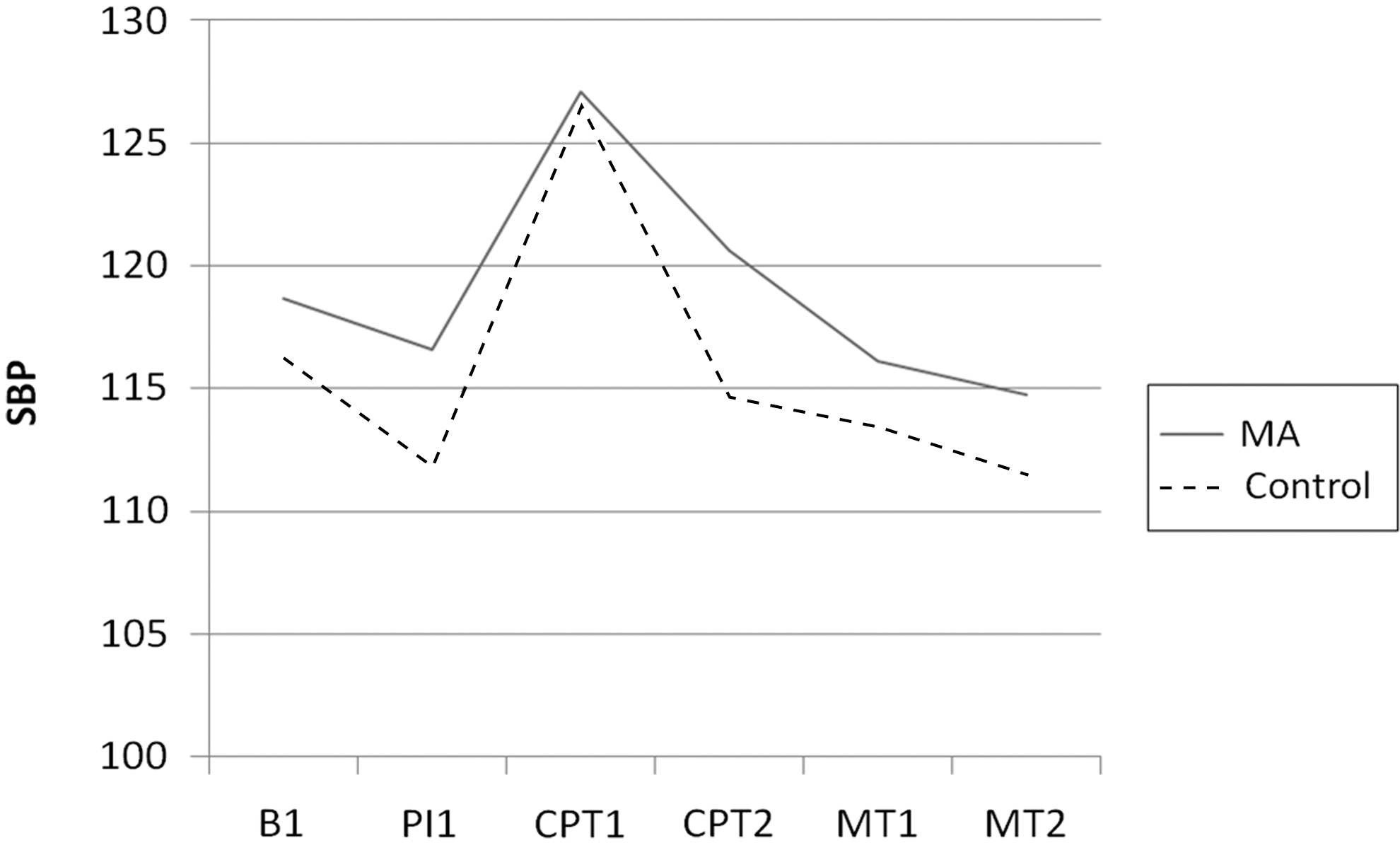
Mean systolic blood pressure (SBP) responding though duration of experiment (B1, baseline; PI1, postinduction; CPT1, cold pressor reactivity; CPT2, cold pressor recovery; MT1, mirror-tracing reactivity; MT2, mirror tracing recovery; MA, mindfulness analog.
Recovery from the MT
To test the hypothesis that participants in the mindfulness condition would have reduced latency to recovery to the MT compared to participants in the control condition, a 2×3 repeated-measures ANCOVA was performed on cardiovascular recovery to the MT task, with group status and 1-minute intervals of time up to 3 minutes as the independent variables. Once again, SBP, DBP, and HR were respectively added as covariates.
There was no significant main effect of condition on: SBP F(1,92)=0.671, p=0.415, ηp 2=0.007; DBP, F(1,92)=0.006, p=0.937, ηp 2=0.000; or HR, F(1,92)=0.006, p=0.937, with a ηp 2=0.000, indicating that condition had no impact on physiologic indices with regard to recovery from the MT.
Discussion
This study evaluated the effect of a brief mindfulness induction compared to a control condition on short-term physiologic outcomes when participants were exposed to a physical and a cognitive stressor. A couple of studies have looked at the effects of mindfulness inductions on physiologic outcomes, 15,22 but none examined the effects on cardiovascular reactivity and recovery to a stressor after a single-session mindfulness induction. A single-session analog may help us understand how traditional-length interventions work and may also confer some benefit in a brief period of time. Furthermore, previous studies have not examined these effects in individuals with a family history of hypertension, a population predisposed to experiencing increased CVR and at greater risk of developing hypertension.
Reactivity and recovery to stressors
This study proposed that exposure to a MA induction would result in reduced reactivity and quicker recovery to stressful tasks. These hypotheses were not supported, and particular recovery findings were in the opposite direction of what was expected. When exposed to the CPT, the mindfulness group had slower and reduced rates of SBP recovery than the control group. DBP recovery trended in this same direction. Since the effect size was small and there is no theoretical reason to think that there would be a differential impact on diastolic versus systolic responding, it is reasonable to conclude that DBP recovery was affected similarly to SBP recovery.
Taken together, these findings are in contrast to the study by Kingston and colleagues, 15 which suggested that mindfulness interventions that are longer in duration and practiced more frequently may reduce physiologic response to stress. These seemingly inconsistent findings may be due to differences in the length and content of the interventions being tested. It is important to note that this study did not evaluate a true mindfulness intervention, which typically involves multiple sessions spread over the course of many weeks. Instead, this study evaluated a brief MA that gave participants only a limited dose of the mindfulness experience. Furthermore, participants in the present study were meditation-naïve. These points are salient because increased focused awareness toward aversive discriminative stimuli should theoretically result in an initially large physiologic response, which should then decrease with repetition. Over time, enhanced attention and awareness to discriminative stimuli should lead to habituation of physiologic responding to these stimuli. Mindful breathing may initially draw attention to the internal sympathic response to imposed external stressors, thus increasing physiologic arousal. 30 With repeated practice, the sympathetic arousal associated with novel or uncomfortable internal stimuli (e.g., nociceptive pain) would be expected to habituate and generalize. Studies incorporating meditation going back more than 30 years suggest that repeated or prolonged meditation may reduce reactivity, 29 –31 and recent research suggests that mindfulness may increase the rate of extinction for learned behaviors. 33
Given that limited exposure to mindfulness may increase physiologic arousal, it is unclear why recovery, but not reactivity, scores differed between the MA and control conditions. It is possible that participants found it difficult to practice mindful breathing during the reactivity period. While undergoing stressful tasks, there may have been a considerable amount of competition for participants' cognitive resources. As a result, perhaps effects of the induction were only revealed during the recovery period. This is consistent with the cognitive load literature, which suggests that physical and cognitive tasks share competition for bodily resources. Therefore, increased physical stress would make it more difficult for MA participants to engage in practicing the mindful-breathing induction. 34
It is unclear why the CPT but not the MT task revealed an effect on physiologic recovery. During recovery from a stressor, the vagus nerve is activated in an attempt to reduce sympathetic responding and maintain homeostasis. As the MT task occurred immediately following the CPT, there may have been a carryover effect whereby vagal activity was still suppressing SBP and HR responding, an effect that has previously been demonstrated by Mezzacappa and colleagues. 35
Clinical implications
This study evaluated a sample of participants with a family history of hypertension, a group that is predisposed toward development of hypertension. It has been proposed that this development may, in part, be mediated by greater CVR and latency to recovery from stress. Therefore, interventions that reduce this reactivity and latency to recovery may ameliorate the progression toward hypertension. There is a literature demonstrating the effect of mindfulness-type meditations on reducing BP in normotensive samples. 14,15,22 There is also anecdotal evidence of the effectiveness of mindfulness meditation for hypertension, but efficacy has yet to be examined and the mechanism is unclear. For example, it is uncertain whether practicing mindfulness may lead to a cognitive reframing of stress, habituate physiologic responding to stressors, or some combination of both. 36
The present study suggests that brief mindfulness analogs asking listeners to maintain awareness of bodily sensations (i.e., breath) may reduce BP recovery from a stressor. More specifically, this latency to recovery occurred after a physical stressor, but not a cognitive stressor. This has potential implications for clinicians interested in decreasing cardiovascular risks for patients who may regularly endure painful stimuli or other physical stressors. It is not entirely surprising that focused internal attention during painful stimuli inhibited autonomic recovery. Decades of previous research have supported the use of distraction, not focused attention, for improving the experience of pain. 37 However, in experimental research, mindfulness training has been shown to be as beneficial as distraction in reducing subjective pain experience during laboratory stressors and better than distraction at reducing pain sensitivity over time. 38 Therefore, it remains unclear what aspects of the current study's intervention resulted in this unexpected and undesired cardiovascular outcome. Until the mechanisms of mindfulness meditation interventions can be evaluated further and clarified, clinicians should be cautioned against the use of brief MAs such as this one to improve cardiovascular recovery after physical stressors.
It is important to keep in mind that these results can only generalize to young populations with a family history of hypertension and single-session, breathing-focused mindfulness analogs. Longitudinal studies such as the HARMONY * may produce tangible evidence for the effectiveness of full-length interventions on hypertension that can guide clinical practice beyond the constraints of the current study.
Limitations
The hand CPT was used as a physiologic stressor because it has demonstrated a large and reliable effect on sympathetic nervous system indices. This effect, and the associated nociceptive pain, requires instructing participants that they can halt the task at any time. This complicates data analysis because it results in a varying number of physiologic readings, depending upon participants' immersion times. Choosing a physiologic stressor that allows for an equal number of reactivity readings for each participant would have allowed for measurement in slope as well as changes in directionality over the course of the stressor as opposed to a single averaged reactivity reading.
Measuring adherence is a thorny issue in meditation interventions, and there are no generally agreed-upon guidelines. In the present study, the adherence probes may have been disruptive to the participants' ability to engage in the MA induction. These probes may also have served to encourage concentration as opposed to mindfulness, potentially reducing the effectiveness of the induction. 39
Future directions
The early work on distraction and attention in coping with distress may inform future studies (for an early meta-analysis see Suls and Fletcher 40 ). For example, McCaul and Haugtvedt 37 conducted an experiment in which participants used distraction or attentiveness to cope with CPT distress. They found that distraction was the superior coping method initially, but attentiveness was superior in managing distress in the latter stages. Accordingly, future studies may employ a CPT paradigm that is more tolerable (i.e., lower temperature) in order to discern effects that unfold over longer periods of time. This may reveal whether a mindful-awareness strategy begins to exert superiority with longer duration of immersion.
Conclusions
This present MA induction was designed to evaluate only one component of mindfulness—awareness—but mindfulness is thought to be a multifaceted construct. 41 Other facets, such as describing inner experience or cultivating a nonjudgmental attitude, may be necessary in reducing reactivity. Future studies could examine possible benefits of adding such components.
The question of minimum or adequate amount of dosage (i.e., length and number of sessions) to reveal treatment effects is one with great potential clinical utility. What is the minimum amount of intervention necessary to acquire benefits, and is there a point of diminishing returns? Future studies might contrast various frequencies and durations of doses to further answer these questions.
Footnotes
Disclosure Statement
No competing financial interests exist.
*
Sunnybrook Health Sciences Centre & University Health Network, Toronto. HARMONY Study (Hypertension Analysis of Stress Reduction Using Mindfulness Meditation and Yoga). In: ClinicalTrials.gov [online]. Bethesda, MD: National Library of Medicine (US). 2000 [cited May 15, 2011]. Online document at: