
Abstract
Aim:
The aim of the present study was to investigate the usefulness of rose essential oil as a supplementary and adjunctive therapy for the relief of renal colic, specifically because rose essential oil is soothing and can act as a muscle relaxant.
Materials:
Eighty patients who were diagnosed with renal colic in the emergency room were included in the study, with ages ranging from 19 to 64 years. Half of the patients (n=40) were treated with conventional therapy (diclofenac sodium, 75 mg intramuscularly) plus placebo (physiological serum, 0.9% NaCl), while the other half (n=40) were given aromatherapy (rose essential oil) in addition to conventional therapy. In each patient, the severity of pain was evaluated using the Visual Analog Scale (VAS) (0 [no pain] to 10 [very severe pain]).
Findings:
The VAS values prior to the start of therapy, and 10 and 30 minutes after therapy were 8.18±1.36, 5.60±2.02, and 3.75±2.08 for the conventional therapy plus placebo group, while for the conventional therapy plus aromatherapy group, the VAS values were 8.63±1.03, 4.25±1.72, and 1.08±1.07, respectively. There was no statistically significant difference between the starting VAS values of the two groups, but the VAS values 10 or 30 minutes after the initiation of therapy were statistically lower in the group that received conventional therapy plus aromatherapy.
Conclusion:
This study demonstrated that rose essential oil therapy in addition to conventional therapy effectively reduces renal colic pain.
Introduction
Aromatherapy can help improve the physical, mental, and/or general quality of life of a patient. Recently, it has become increasingly popular and is an accepted supplementary and adjunctive therapy in many countries. 7 –9 Aromatherapy has been used for more than six millennia and can be applied in several ways, the most common of which are massage, inhalation, and vapor. 10 In particular, patients may prefer this therapy for the relief of tiredness, anxiety, stress, nausea, and vomiting. 11
It has been reported that pure essential oils may have a variety of positive effects such as regulation of the emotional state, 12 anxiety control, 13 reduction of depression, 14,15 stimulation and strengthening of the memory, 16 and improved cognitive processes in dementia patients. 17 Recently, rose essential oil has been reported to have anxiolytic, anti-inflammatory, analgesic, and antispasmodic effects. 18,19
Professional organizations in developed countries strongly encourage the use of aromatherapy to decrease anxiety. 20 Despite the absence of professional standards for the use of aromatherapy, there are multiple studies published in the United States concerning the use of aromatherapy, and a large portion of part of the society is reported to use these adjunctive therapies. 21
There are studies in the literature that demonstrate the efficacy of alternative therapies such as acupuncture for the treatment of renal colic. However, to date there has been no study concerning the use of aromatherapy for the treatment of renal colic. Since rose essential oil has soothing and antispasmodic effects, the aim of this study was to investigate the possibility of using rose essential oil use as a supplementary and adjunctive therapy to drug therapy for the treatment of renal colic.
Materials and Methods
Subjects
This study was approved by the ethics board of Gaziosmanpasa University (10-BADK-021). Written informed consent was obtained from all participants. Eighty patients with the diagnosis of renal colic whose ages ranged from 19 to 64 years were included in the study.
Inclusion criteria
The patients were evaluated using a detailed history, physical examination, and routine hematological and biochemical tests. Kidney stones were diagnosed using plain abdominal radiography and ultrasonography. Patients who had flank pain and were positive for kidney stones were included in the study.
Exclusion criteria
Patients with allergies, the common cold, a history of asthma, renal dysfunction, peptic ulcer disease, or chronic obstructive pulmonary disease or who were pregnant at the time of the study were excluded. In addition, patients taking anticoagulant treatment or who had an allergy to nonsteroidal anti-inflammatory drugs (NSAIDs) or had taken NSAIDs within 24 hours were excluded.
Study design
The study was designed as a double-blind, randomized, placebo-controlled interventional study. Patients were randomly placed in one of the two study groups and were identified only by patient number. The rooms in which the therapy took place were simply labeled with either a single or a double number. Patients were treated in one of two rooms, which were separated from each other but had the same layout. Patients were forbidden to talk with one another. Health care personnel who were uninformed about the study evaluated the severity of the pain experienced by all participants in the study. Patients in group I (single number, n=40) were treated with conventional therapy (75 mg intramuscular diclofenac) plus placebo (physiological serum, 0.9% NaCl), and those in Group II (double number, n=40) were treated with conventional therapy (75 mg intramuscular diclofenac) plus aromatherapy.
Drug administration and inhalation of essential oil
Rose essential oil was purchased from Gulbirlik (Isparta, Turkey). In addition to the conventional treatment, the double number group received aromatherapy given via an electronic vapourizer (Robert Tisserand Ltd.) and maintained at a 2% concentration as previously described. 22 The single number group received physiological serum via an electronic vapourizer, which was refilled continuously as a placebo treatment in addition to conventional therapy.
Measurement of pain
In all groups, the pain severity of the patients was evaluated using the Visual Analog Scale (VAS) which ranges from 0 (no pain) to 10 (very severe pain). The VAS results were further categorized as 0 (no pain), 1–4 (mild pain), 5–6 (moderate pain), and 7–10 (severe pain). 23 The VAS, mean arterial pressure (MAP), and pulse rate in beats per minute (BPM) were measured in all patients before treatment and 10 and 30 minutes after the treatment. The VAS levels of both groups were compared using statistical analysis.
Statistical analyses
The Kolmogorov-Smirnov test was used to determine whether the data was normally distributed. In order to compare the data from the two groups, an independent sample t-test and Mann-Whitney U test were used, and p-values lower than 0.05 were considered significant.
Results
The demographic characteristics, MAP, and pulse rate of the patients are shown in Table 1 and Table 2. Of the 80 patients in the study, 39 were men and 41 were women. The mean age was 36.20±9.32 years in the conventional therapy plus placebo group and 36.87±8.86 years in the conventional therapy plus aromatherapy group. The mean VAS values of the patients are shown in Table 3. The mean VAS values before and 10 and 30 minutes after treatment were 8.18±1.36, 5.60±2.02, and 3.75±2.08 in the conventional therapy plus placebo group and 8.63±1.03, 4.25±1.72, and 1.08±1.07 in the conventional therapy plus aromatherapy group, respectively. There was no significant difference between the two groups in terms of age and sex. Although there was no difference between the VAS values of the two groups before treatment, in the conventional therapy plus aromatherapy group, the VAS values 10 and 30 minutes after treatment were statistically lower than the corresponding VAS values in the conventional therapy plus placebo group (p=0.002 and 0.000, Mann-Whitney U test, Figure 1).
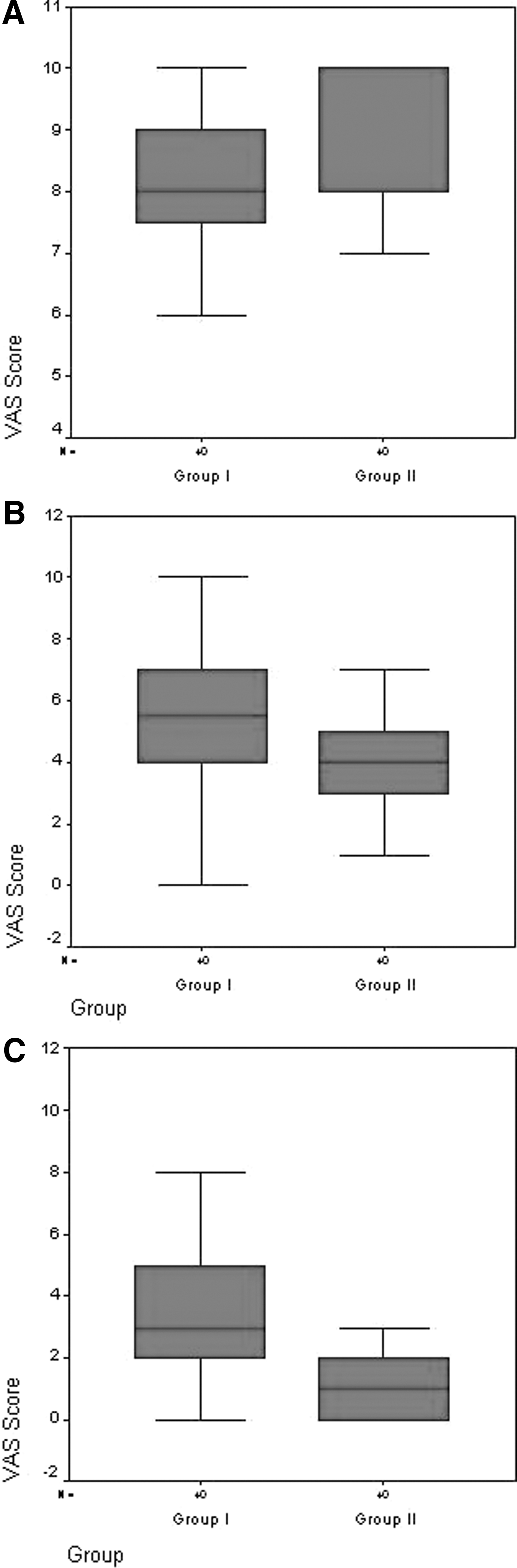
Comparison of visual analog scale (VAS) scores between the patient groups at initial
Data are expressed as mean±SD.
Data are expressed as mean±SD.
MAP, mean arterial pressure; BPM, beats per minute.
Data are expressed as mean±SD.
VAS, visual analogue scale.
p<0.05.
Discussion
Pain is defined as an unpleasant, affective, and emotional experience that can originate from any part of the body and can be related to past experiences and associated with actual or possible tissue damage. 24,25 In addition to severe pain, psychomotor agitation and costovertebral angle tenderness may accompany renal colic. Intraluminal pressure, which increases with obstruction, strains and stimulates nerve endings located in the urinary tract mucosa, resulting in a colic type of pain. 3,4 An exact measurement of pain severity is one of the major challenges for physicians. Different visual and numerical scales have been used to show the severity of the pain. One such scale is the VAS, which has been used in different studies to determine pain severity in a variety of conditions and types of pain. 26
In the present study, the average initial (before treatment) VAS value of the patients admitted to emergency room with renal colic was 8.18±1.36 in the conventional therapy plus placebo group and 8.63±1.03 in the conventional therapy plus aromatherapy group. In a recent study, the VAS values of patients with renal colic were found to be 8.95±0.11 prior to treatment. 27 In addition, high initial VAS values were reported in some studies that investigated the efficacy of analgesics for renal colic. 28,29 Therefore, the initial VAS values of the patients with renal colic in the present study are consistent with the past literature.
Aromatherapy is one of the most popular adjunctive therapies in recent years, and the mechanism of its effect is related to smelling essential oils from aromatic plants. 8,30 Aromatherapy is believed to have a therapeutic effect in conditions such as anxiety, depression, and chronic pain induced by stress by affecting the hippocampal formation and regions of the limbic system such as the hypothalamus and piriform cortex. 31 It has been shown that bergamot, which was administered by a microdialysis method, affected a calcium-dependent pathway and increased aspartate, glycine, and taurine levels in the extracellular space in hippocampal tissue. 32 Ceccarelli et al. 33 found that lemon essential oil affected the olfactory-hippocampal pathway in rats and regulated acetylcholine release, thereby having an effect on pain sensation. Aromatherapy was reported to affect GABAergic and putative glutamatergic neurons in addition to cholinergic neurons. 33 Systemic or locally applied aromatherapy (bergamot essential oil) is thought to exert its effect by acting on a portion of the excitatory and inhibitory neurons in the dorsal hippocampus. 34
In the present study, which evaluated the potentially soothing effect of rose essential oil in patients with renal colic, it was found that the VAS pain values were statistically lower after 10 and 30 minutes of treatment with aromatherapy in addition to conventional therapy compared to patients who received conventional therapy and a placebo (p=0.002 and 0.000). Initial MAP and BPM values of placebo were higher than the aromatherapy group. These values may have been affected because of the stress during the first entrance to the emergency department. Reduction of stress with treatment may have been decreased these values in both groups. This decline is greater in the placebo group than the aromatherapy group because of higher initial VAS values of the placebo group.
In animal studies, aromatherapy has been found to sedate hyperactive rats who had received agents such as caffeine. 35 Ileum spasm induced by electrical shock in experimental animals was relieved through the topical application of lavender aromatherapy. 30 It was found that in patients undergoing a breast biopsy, lavender aromatherapy did not result in a significant decrease in pain (as measured by VAS) but increased the level of pleasure in the patients. 36 In a study that investigated the effect of odor on mood and automatic and immune functions, a lemon odor was found to result in a better mood and to increase norepinephrine release. 37 Braden et al. 38 reported that preoperative patients who received lavender aromatherapy had higher satisfaction and lower anxiety, and it has also been found that aromatherapy consisting of lavender, sage, and rose decreased pain in patients with dysmenorrhea. 39
Professional organizations strongly support the use of aromatherapy for the reduction of anxiety. 20 Aromatherapy has recently become a legal part of holistic nursing. 22
This study demonstrated that rose essential oil therapy effectively reduced renal colic pain when combined with conventional therapy. In this context, the use of aromatherapy—a nonpharmacological modality increasingly used as an adjunctive therapy to conventional therapies—and rose essential oil in particular may be considered as a supporting agent for painful conditions like renal colic. Further studies are warranted.
Footnotes
Author Disclosure Statement
No competing financial interests exist.