
Abstract
Objectives:
Current treatment strategies for painful diabetic neuropathy (PDN) include oral medications, which are costly and may have adverse effects. Topical therapies have been used for PDN with some benefit. Nutmeg has certain properties that may be effective in ameliorating neuropathic pain. The purpose of this study was to determine whether topical nutmeg extracts can reduce pain or improve the quality of life in PDN sufferers.
Design:
This study was a randomized, double-blind, placebo-controlled trial.
Settings/location:
It was conducted at a primary care center in Trinidad, Caribbean.
Subjects:
Seventy-four (74) diabetic subjects who met criteria for painful neuropathy were recruited.
Interventions:
Participants were randomized to receive either topical nutmeg extracts (NEMM; mace oil [2%], nutmeg oil [14%], methyl salicylate [6%], menthol [6%], and coconut oil) or placebo (MM; methyl salicylate [6%], menthol [6%], coconut oil, and alcohol).
Outcome measures:
Outcome measures of pain and quality of life were assessed using the Brief Pain Inventory for Diabetic Painful Neuropathy and Neuropathic Pain Symptom Inventory.
Results:
An intention-to-treat analysis was done for 24 male and 50 female subjects (30–85 years) with an average duration of diabetes of 11 years. Significant reductions in worst and average pain scores were seen within each group (p≤0.001). Similarly significant reductions were also noted for interference with walking, sleep, and mood scores as well as burning, pins and needles, and tingling scores within each group (p<0.05). There were no statistically significant differences between both groups after 4 weeks for any outcome measure.
Conclusions:
In this trial topical, nutmeg extracts did not add to the improvements observed in PDN symptoms during 4 weeks treatment with preparations containing menthol and methyl salicylate. Further research designed to test the individual components of the topical therapies used in this study may clarify their benefit.
Introduction
Strict glycemic control is perhaps the single greatest preventative measure for neuropathy. However, once pain develops, current treatment options are not specific for the underlying cause of nerve damage and are aimed at symptomatic relief. Tricyclic antidepressants (e.g., amitriptyline), carbamazepine, gabapentin, pregabalin, and duloxetine have undergone clinical trials for use in PDN, but only the latter two are approved by the U.S. Food and Drug Administration for treatment. 6 Although an increasing number of trials have investigated different kinds of drugs to manage neuropathic pain, anticonvulsants and antidepressants are still the options most commonly used for PDN. 7 Long-term studies of the efficacy and adverse effects of these drugs and the need for novel drug and nonpharmacological strategies have been emphasized. 7
In addition to oral therapies, topical treatments have also been used for PDN. Several controlled studies combined in a meta-analysis provide some evidence that the topical application of capsaicin has efficacy in diabetic neuropathic pain. 8 However, of major clinical concern, topical capsaicin application has been shown to produce nearly complete denervation of the epidermis in both control subjects and people with diabetes. 9 Glyceryl trinitrate spray has also demonstrated significant pain reduction compared to placebo with approximately 10% of patients experiencing side-effects of palpitation and headache. 10 Minimal clinical improvements have also been found with 5% lidocaine applied topically. 11
Complementary and alternative modalities are increasingly being used in the treatment of diabetes and its complications, even in the developed world. 12 Trinidad is no exception, with as many as 42% of persons with diabetes using herbal remedies in general and 24% using bush medicines specifically for their diabetes. 13 In Trinidad it has also been shown that diabetes is associated with low income status, worse health status, and more frequent expenditure on medical services. Furthermore, adults with diabetes who delayed or did not get needed conventional medical care because of cost are more likely to report the use of complementary or alternative medicine. Clearly, a less expensive complementary alternative with fewer adverse effects will be more acceptable to PDN sufferers. Nutmeg may offer hope as such an agent.
Nutmeg is the dried kernel of the broadly ovoid seed of Myristica fragrans Houtt. (Myristicaceae), a bushy evergreen tree that is found in most Caribbean islands. Mace is the seed coat of the same species. Historically, nutmeg has been widely used as a spice, and in alternative medicine it has been reported to have various medicinal (narcotic, hypolipidemic, antithrombotic, and anti-inflammatory 14 ) properties.
Phytochemical studies indicate that nutmeg contains a volatile oil, a fixed oil, proteins, fats, starch, and mucilage. The fixed oil contains myristin and myristic acid. Nutmeg yields 5%–15% of volatile oil, which contains pinene, sabinene, camphene, myristicin, elemicin, eugenol, isoeugenol, methoxyeugenol, safrole, dimeric phenylpropanoids, lignans and neolignans. 15,16
Some studies support nutmeg as a potential analgesic for PDN. It has demonstrated analgesic effects in animal models. 17,18 Impaired skin microvascular reactivity has been one recent postulate in the pathogenesis of PDN. 19 Some researchers have investigated the effects of eugenol present in nutmeg oil on nerve and vascular dysfunction in diabetic rats. 20 They found that aspects of both vascular and neural complications were improved by eugenol and concluded this could have potential therapeutic implications for diabetic neuropathy and vasculopathy. 20 Eugenol-containing periodontal dressings have also been used successfully for pain relief following gingivectomy. 21
In the absence of any randomized clinical trial on nutmeg, the main objective of this study was to test topical nutmeg extracts' ability to reduce pain or improve quality of life in patients with PDN.
Research Design and Methods
This was a double-blinded randomized controlled trial carried out at the St. Joseph Enhanced Health Centre, Trinidad between October 2010 and May 2011. Respondents from diabetes outpatient clinics were screened according to entry criteria. Inclusion criteria included age 21–85 years, diabetes or impaired glucose tolerance, symptoms limited to the extremities of limbs, and an average neuropathic pain >4 as determined by the DN4 (Douleur Neuropathique) Questionnaire. 22 The French Neuropathic Pain Group validated the clinician-administered DN4 questionnaire, which was shown to have a sensitivity of 82.9% and specificity 89.9% for the diagnosis of neuropathic pain in patients with a score of 4/10. Exclusion criteria were soft-tissue infections and injuries, radiating cervical or lumbosacral pain, tendinitis, spurs, broken skin or rash at pain sites and salicylate allergy.
Eligible volunteers were provided with an information sheet that thoroughly explained the trial protocol. They were told that a new topical treatment was being tested that might possibly relieve their symptoms, and upon agreement they signed informed consent. No alteration was made by the trial investigators to the treatment of diabetes and its comorbidities as this was continued by the participants' usual caregivers. Any patient on prior antidepressant or anticonvulsant therapy for painful neuropathy was instructed to continue the medication at the prescribed dose. Any topical preparation used in the area of symptoms was discontinued at least 1 week prior to treatment.
A random-number-generating software was be used to generate two equal sets of 40 per arm of random numbers ranging from 1 to 80, and the 40 treatment bottles and 40 placebo bottles were numbered accordingly. The treatment (NEMM) was a commercially available topical preparation containing mace oil (2%), nutmeg oil (14%), methyl salicylate (6%), menthol (6%), coconut oil, and alcohol. The placebo (MM) was a topical preparation containing only methyl salicylate (6%), menthol (6%), coconut oil, and alcohol. All treatments were in similar 125-mL spray bottles, and their contents were colorless and of the same viscosity. The menthol present in all treatments also ensured that their odors were the same.
Consecutive eligible patients picked sealed envelopes, each containing one number ranging from 1 to 80, and each participant was given their own bottle, which had clear instructions on use, but no other information identifying any ingredients. Participants were instructed to apply 4 sprays of the assigned treatment to the affected area 3 times a day followed by gentle massage for 4 weeks. Age, gender, ethnicity, glycosylated hemoglobin, presence of hypertension, smoking, duration of diabetes, antidepressant/anticonvulsant use, neuropathic pain, and daily function scores were all recorded as baseline variables. Participants were asked to return with their treatment bottles at 1, 2, and 4 weeks. A modified version of the Brief Pain Inventory was validated for Diabetic Painful Neuropathy (BPI-DPN). 23 The BPI-DPN was to be used to assess pain severity as well as its impact on daily functioning. The Neuropathic Pain Symptom Inventory (NPSI) 24 was also used to quantify different aspects of neuropathic pains. All scores were measured by a blinded assessor.
Although well-validated scales were used in this study, the investigators wanted to test how the numerical rating scales (NRS) measured up against visual analog scales (VAS), another popular method of pain assessment. VAS equivalents to NRS questions for worst pain, average pain, and interference of sleep and general activity scores (4 BPI-DPN descriptors) were administered to 20 consecutive trial patients who were blinded to their scores. These data were then analyzed for any significant correlations. Compliance was determined by bottle weights as well as patient testimony to use of 4 sprays three times daily over the preceding 24 hours. Adverse events were noted.
A sample size of 32 patients in each group was calculated as 80% power, 5% significance level, standard deviation for worst pain severity score 2.823 to detect a difference of at least 2 points on both pain severity and mean interference scores between groups. A difference of 2 points was validated as being a clinically important change in pain level for both acute 25 and chronic pain. 26
Mann-Whitney U tests were used to compare pain, interference with activity scores, and NPSI scores between groups. Wilcoxon rank-sum tests were used to measure score differences within each group. These nonparametric tests were used because the pain score data collected were ordinal and not normally distributed. Fisher's exact test and χ2 tests with appropriate corrections were used for 2×2 contingency tables. An intention-to-treat (ITT) analysis was performed. All patients in each group were included in the final analysis, with last observations carried forward for imputation of missing data (dropouts). All calculations were two-sided and done with SPSS Software (Version 17) using 5% significance levels.
This study was approved in July 2009 by the Ethics Committee of the Faculty of Medical Sciences, The University of the West Indies, St. Augustine, Trinidad. Permissions to use the necessary assessment inventories were also obtained.
Results
Of 120 respondents, 74 patients met entry criteria and their progress throughout the trial is depicted in Figure 1.
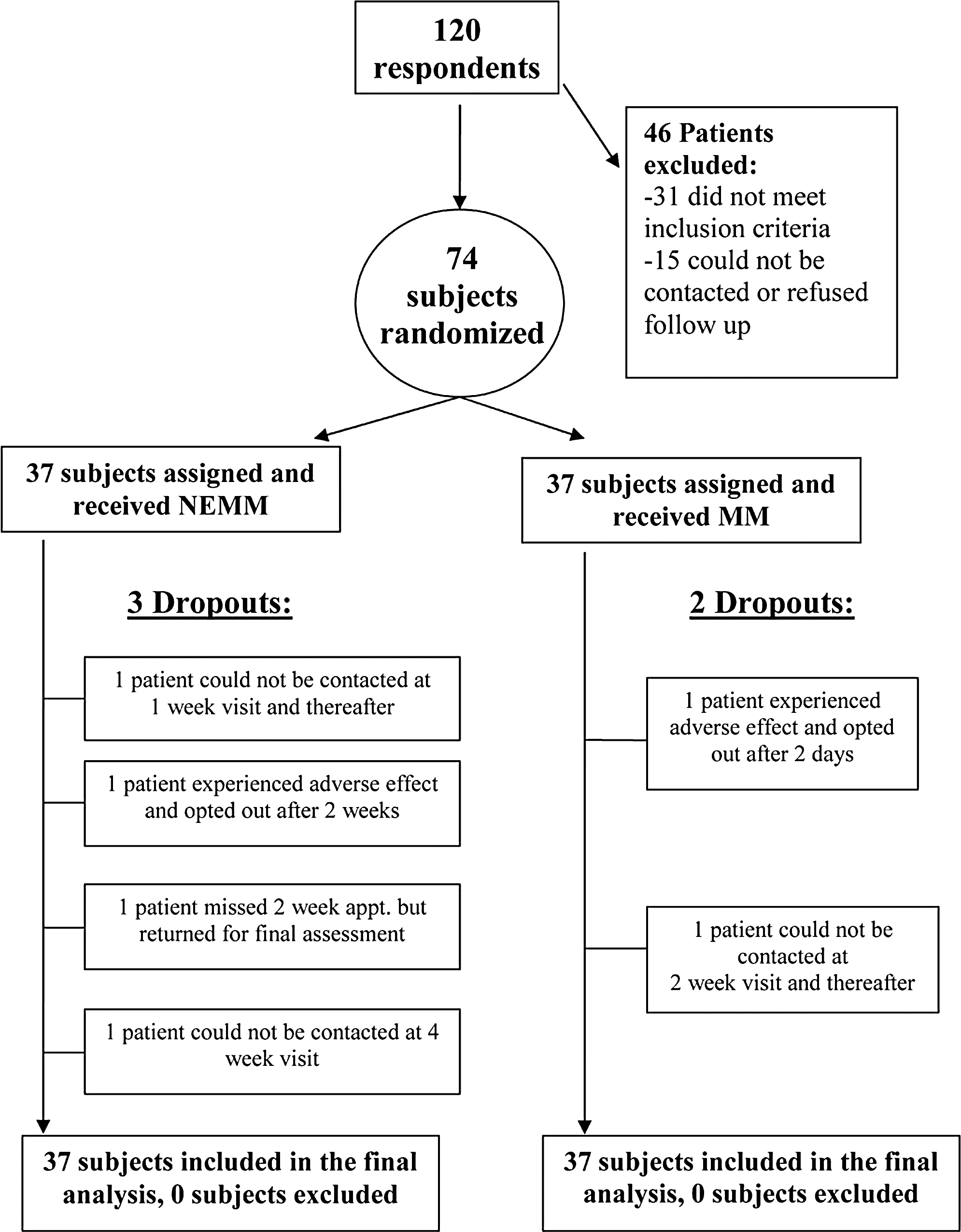
Flow diagram showing the progress of the patients throughout the trial.
Table 1 shows the baseline characteristics of study participants, which were very similar. There were also no significant differences between groups with respect to baseline outcome measures of pain and interference with function (p>0.05).
Data are shown as percentages or mean±SD (standard deviation).
NEMM, treatment; MM, placebo; HBA1c, glycosylated hemoglobin.
There were statistically significant reductions in both pain (average, worst, total NPSI, burning, pins and needles, tingling) scores and interference with function (sleep, mood, and walking) scores within each group after 4 weeks compared to baseline (p<0.05).
Within each group, the worst pain scores fell by at least 2 points or were reduced by at least 30% over the 4-week period. The mean of other pain and interference with function scores (except mood) also fell by at least 2 points. Of importance, statistically significant reductions were apparent from as early as 1 week for worst, burning, pins and needles, total NPSI and interference with general activity scores in each group (p<0.05).
Table 2 displays comparisons for pain and quality of life scores between the treatment and placebo groups at the end of the study. There were no statistically significant differences between the groups at the end of the follow-up period for any outcome measure. In the NEMM group, 48.6% versus 43.2% in the MM group achieved at least a 33% reduction in worst pain from baseline to 4 weeks. The difference between groups was not statistically significant (p=0.64, relative risk=1.12; 95% confidence interval 0.69 – 1.85).
Data are shown as mean±standard deviation, median.
BPI-DPN, Brief Pain Inventory for Diabetic Painful Neuropathy; NPSI, Neuropathic Pain Symptom Inventory.
A consecutive series of 20 randomized patients had their worst pain, average pain, interference scores with general activity and sleep assessed by a self-administered 10-cm visual analogue scale. There were significantly positive correlations for worst pain (r=0.78, p<0.001), average pain (r=0.66, p=0.002), and interference with sleep scores (r=0.70, p=0.001).
Table 3 shows compliance rates and bottle weights over time. Compliance remained uniformly above 75% between groups throughout the follow-up period, falling to less than 75% in both groups at 4 weeks. Bottle weights revealed similar medication consumption in both groups throughout the trial period. At the end of the trial, worst pain scores were compared between compliers and noncompliers within each group, which revealed no differences.
Compliance shown as %.
Bottle weights shown as mean±standard deviation.
NEMM, treatment; MM, placebo.
The incidence of side-effects during this trial was similar in both groups (10.8% in NEMM versus 5.4% in MM group, p=0.67). One (1) patient (2.7%) in the MM group discontinued treatment after 2 days due to blisters on the heels. Another MM recipient complained of heaviness, but it was transient, and chose to continue therapy. One (1) patient (2.7%) in the NEMM group opted to stop therapy after 2 weeks due to eye pain and headache, although the treatment was not applied close to these areas. Two (2) NEMM recipients complained of burning and another complained of stiffness. The 3 latter participants continued treatment until trial completion as their symptoms were transient and tolerable.
Discussion
Treatment effects
This was the first clinical trial to assess the efficacy of nutmeg extracts in relieving pain in patients with PDN. Patients in this trial had painful neuropathy of moderate severity with baseline pain scores in excess of 6 for both average and worst pain (BPI-DPN). There were, however, no differences between both groups at the end of 4 weeks, despite significant improvements in pain and daily functions within each group.
The decreases in pain scores within each group were also clinically significant, as these differences were at least 2 points. The percentage pain reduction of at least 33% seen for worst pain in each group was also a clinically relevant one. 25,26
It was hypothesized that the similar benefits in the intervention and control groups may have been due to the other ingredients in the preparation used, especially the methyl salicylate (6%) and menthol (6%). A topical methyl salicylate and menthol patch was found to relieve mild to moderate muscle strain in one study of adult patients without serious adverse events. 27 Case reports have also cited benefits of menthol for chemotherapy-induced neuropathic pain 28 and postherpetic neuralgia. 29 Menthol appears to produce its effects through action on the topical transient receptor potential melastatin (TRPM8) receptor. 30,31 Its special properties have led some investigators to believe that this receptor has potential as a drug target, in treating a wide variety of physiological conditions. 32
Placebo effects
Another possible explanation for the apparent benefits seen in both groups is the placebo effect. Placebo (from Latin, meaning “I want to please”) was conceptualized as a commonplace method or medicine prescribed in order to please the patient and not because of its efficacy. 33,34 This has changed over the years, however, as the placebo phenomenon has been well documented for analgesics. 35
Several theories exist that can explain the placebo effect. Psychologic factors, verbal suggestion, expectation and emotional factors, conditioning, and prior experience are some of the possible explanations for the effect. 36 In this trial, all the patients were told that the treatments being tested might possibly relieve their symptoms. This could have contributed to the relief they experienced by increasing their expectations and by verbal suggestion.
Adverse effects and compliance
The adverse event rate resulting in discontinuing therapy for the preparations tested was 2.7% patients in each group. Other side-effects were mild, transient, and tolerable. There were no major systemic side-effects in this trial compared to the adverse effects that have been documented with oral and topical treatments.
Compliance was greatest in the first 2 weeks of this trial. It was measured in part by self-reporting of use of medication because the inventories used to determine the outcomes were mostly specific for symptoms within the past 24 hours. Although compliance dropped at 4 weeks, the reductions in pain seen up to this time in each group may suggest a more long-term effect of the preparations used.
Strengths of this study
This study was a well-designed, double-blinded, randomized controlled trial that adhered to most (24 of 25 item checklist) of the updated CONSORT guidelines. 37
The Special Interest Group on Neuropathic Pain (NeuPSIG) revised guidelines in 2011 for the assessment of patients with neuropathic pain. 38 This study adhered to their updated recommendations as follows: (1) It used suitable screening questionnaires to identify neuropathic pain sufferers (e.g., DN4 Questionnaire); (2) Validated pain inventories were employed; (3) 30% reductions in pain were measured to determine responders with significant pain relief; (4) Both numerical rating scales (NRS) and visual analog scales (VAS) were used.
In the absence of any data to suggest superiority of one scale over the other, there was moderately strong correlation in this study, among a subset of patients, between the NRS used and 10-cm VAS equivalents.
Limitations of this study
This study was conducted over a 4-week period for each patient. Low compliance was the main concern with continuing the trial for a longer period of time. The decrease in compliance in this trial between the 2- and 4-week visits would seem to suggest a downward trend over time if the trial were to be continued beyond 4 weeks. The number of patients used in this trial gave a power of 88%. There remains a possibility that the study could have failed to detect a difference because of the sample size. One of the major limitations in increasing the sample size or testing for a longer duration was the finite number of intervention bottles the researcher had at his disposal.
One main investigator assessed each patient. A second independent assessor, if available, would have allowed for interobserver agreement and reliability, thereby increasing the rigor of the study. Resources at the trial center, however, did not allow for this.
The nutmeg preparation used in this trial was produced by an independent manufacturer. The investigators had no control over the exact constituents of the nutmeg oil used. Given the heterogeneous nature of nutmeg extracts, the percentage of eugenol was unknown. This is one of nutmeg's main constituents for which evidence exists as an analgesic. 24,25 A purified topical eugenol preparation might have proved to be a more ideal intervention.
Lastly, inert placebos were not tested in this trial. This would have meant several additional treatment arms (e.g., massage only, drug vehicle only, menthol only, etc.) Although this may have allowed for more definitive conclusions about the placebo phenomenon and menthol's therapeutic effects, it would not have allowed the study to be of a double-blinded design. The menthol in this trial effectively masked the scent of the nutmeg and mace extracts. Loss of blinding in this regard could have reduced the validity of the study's results. A multiple-arm trial would have also warranted more participants. If this could not be attained, the result would have been smaller group sizes and an underpowered study.
Conclusions
In summary, a topical nutmeg extract preparation reduced PDN scores and improved quality of life after 4 weeks of treatment, but the effects were not superior to the control tested. Further placebo-controlled trials designed to test the individual ingredients of the topical therapies used in this trial (e.g., eugenol, menthol, methyl salicylate) may clarify their usefulness for PDN.
Footnotes
Acknowledgments
The authors are thankful to Mr. Denis Noel of Noelville Ltd., Grenada for agreeing to manufacture and supply both the treatments and placebos used in this trial.
Disclosure Statement
No potential conflicts of interest relevant to this study were reported.