
Abstract
Objectives:
To investigate the effect of sedative music on the different stages of the sleep cycle in young adults with various sleep latencies by using polysomnography (PSG).
Design:
Prospective, randomized, controlled, crossover study.
Setting:
Sleep center of a teaching hospital.
Participants:
Young adults with different sleep latencies. Poor sleepers (Pittsburgh Sleep Quality Index score ≥5) were excluded.
Interventions:
Each participant stayed one night in the sleep center for adaptation and on each of the following two nights was assigned to (1) music and (2) control (without music) conditions in random order. In the music condition, sedative music composed by certified music therapists was played on a compact disc player for the first hour the participant was in bed.
Outcome measures:
Sleep measures recorded with PSG, including sleep latency and durations of sleep stages.
Results:
Twenty-four young adults (mean±standard deviation, 24.5±2.6 years) participated. They were classified into the short sleep latency (SL) group if the baseline SL of the adaptation night was shorter than 10 minutes or into the long SL group if the baseline SL was 10 minutes or longer. Sedative music did not alter the SL in either group. Sedative music reduced stage II sleep in both SL groups (main effect of music, p=0.03; interaction effect, p=0.87) but increased the duration of deep sleep (stages III and IV) only in the long SL group (main effect of music, p=0.15; interaction effect, p=0.02).
Conclusions:
In participants with long SL, sedative music improved the quality of sleep by prolonging the duration of deep sleep. This effect provides an alternative and noninvasive way to improve sleep in selected persons experiencing sleep problems.
Introduction
S
Many studies report that sleep deprivation causes poor memorizing ability, impaired schematic thinking, poor decision-making, decreased motivation, and deteriorated interpersonal responses. 5 Even for elite athletes, jet lag results in profound decreases in fitness and sports underperformance. 6,7 Medications, such as hypnotics and melatonin, are commonly used to manage these sleep problems; however, alternative treatments, such as cognitive–behavioral therapy, are proven to be as effective as medication. 4
Listening to sedative music at bedtime is frequently used to help induce sleep. However, the effect of sedative music on sleep remains unclear. Music is defined as a complex of expressively organized sounds composed of key elements, including rhythm, pitch, harmony, and melody. 8,9 Music applied for sleep promotion is usually described as sedative music, characterized by a slow tempo and smooth melody. 10
Some studies reported that music improved sleep quality, decreased sleep latency, and increased sleep efficiency in elderly persons who experienced insomnia. 11,12 Similarly, Tan noted a sleep promotion effect for music in primary school children. 13 Loewy et al. reported that the effects of live music therapy on achieving sleep or sedation in infants and toddlers undergoing electroencephalography are similar to those induced by pharmacologic sedation. 14 Many of these studies used subjective measurements, such as the Pittsburgh Sleep Quality Index (PSQI), sleep logs, and the Stanford Sleepiness Scale. Only limited studies have evaluated the effect of music on young people; in particular, few have used objective assessment tools, such as polysomnography (PSG). Gitanjali reported that traditional Indian music had no effect on sleep, 15 whereas Alvin et al. found positive effects for music in more than 80% of patients with insomnia according to subjective and objective assessments. 9 Lazic and Ogilvie examined the effect of music on sleep quality using standard PSG measured in 10 young female students and found that music was not significantly better than tones or controlled conditions in improving sleep-onset latency, sleep efficiency, or percentage of slow-wave sleep (also called deep sleep). 16
The purpose of this study was to evaluate the effect of music intervention on the sleep quality of young adults by using PSG. Specifically, the study attempted to characterize the specific sleep stages that are affected by music in order to establish the clinical utility of sedative music for sleep.
Materials and Methods
Participants
Twenty-four young adult students at Chang Gung University were invited to participate in the study. Participant ages ranged between 18 and 30 years (Table 1). The participants were not musicians, and none was in the habit of listening to music at bedtime. They reported no history of obvious sleep problems. Participants were instructed not to consume more than 1.4 mg of caffeine per kg body weight 10 hours before PSG. 17 Female students were instructed to avoid participating in this study during menstruation. 18 The exclusion criteria were the following: (1) major depressive disorders; (2) auditory dysfunction; (3) sleep disorders, such as insomnia, narcolepsy, snoring, sleep apnea, or periodic limb movement syndrome; (4) use of medications that influences sleep, such as hypnotics, sedatives, antidepressants, anticholinergics, antihistamines, tranquilizers, or melatonin; (5) a habit of meditation or relaxation in the evening within 30 minutes of bedtime; (6) a habit of not going to bed until midnight; and (7) difficulty falling asleep in an unaccustomed environment.
Values expressed with a plus/minus sign are the mean±standard deviation.
p<0.05.
PSQI, Pittsburgh Sleep Quality Index; SL, sleep latency.
After participants gave informed consent, they were evaluated with the PSQI. 19 Participants with poor sleep quality, as reflected by a PSQI score of 5 or more, were excluded from the study. This protocol was approved by Chang Gung University Research Ethics Board.
Sedative music
Two certified music therapists composed and played the sedative music. The tempo of the music was 60 beats per minute. The music was played on the piano using a pentatonic scale in a soft Asian style. The total duration of the sedative music played was 1 hour.
Overnight PSG
PSG was performed by using the Compumedics P-series PS2 (Compumedics, Victoria, Australia) system to assess sleep measures. Three consecutive full overnight PSG assessments were done according to the standard procedure recommended by the American Academy of Sleep Medicine. Data for 12 measures were obtained: electroencephalography, electrooculography, electromyography, electrocardiography, air flow, thoracic and abdominal respiratory effort, body position, limb movement, snoring, O2 saturation, light, and pulse rate. All recordings were scored according to the international criteria developed by Rechtschaffen and Kales for sleep–wake determinations. 20
Procedures
The participants were asked to complete the screening questionnaire and informed consent forms 2 weeks before the experiment. During the first night of adaptation, the participant was hooked up to the recording sensors and asked to sleep according to the usual sleep schedule, without any intervention in the sleep center. The goal of this adaption night was to allow participants to get accustomed to the laboratory environment. During the following two nights, each participant spent one night in the music condition and another night in the control (without music) condition. The sequence of these two conditions was determined by using a random-sequence generator in accordance with a randomized, controlled, crossover design. The participant slept in the same room for these consecutive three nights. The room temperature was set at 25°C.
Once the participant was in bed, the biocalibration procedure was conducted. When the lights were out, the background sedative music was played for 1 hour on a compact disc player in the music condition, whereas no music was played for the control condition. The participant was then allowed to sleep uninterrupted for the remainder of the night. Participants were not given any specific instructions to attend to or ignore the music.
Data Analysis
To characterize the differences in music effect on participants with different sleep latencies, participants were divided into two groups according to an arbitrary criterion of sleep latency. Participants with sleep latencies shorter than 10 minutes were assigned to the short sleep latency group, and those with sleep latencies longer than 10 minutes were assigned to the long sleep latency group. Ten minutes was chosen as the cutoff value because this is the mean sleep latency observed in the adult population. 21
SPSS software, version 12 (SPSS, Inc., Chicago, Illinois), was used for statistical analysis. Differences in age, body height, body weight, body–mass index, and sleep latency between the two groups were compared by using the Student t test, and differences in gender distribution were determined by using the chi-square test. For sleep variables, two-way analyses of variance (ANOVA) for repeated measures (two conditions×two groups) were used to examine the main effects of music and sleep latency group as well as the interaction effects. Statistical significance was set at p<0.05.
Results
Twenty-four young adults were enrolled in this study: 11 men and 13 women. Their mean age (±standard deviation) was 24.5±2.6 years, and their mean sleep latency was 15.5±13.7 minutes (Table 1). The comparison of demographic data shown in Table 1 indicates that gender, age, body weight, body–mass index, and PSQI score did not differ between the short and long sleep latency groups, except that the short sleep latency group tended to be taller (p=0.05).
Figure 1 shows that the sedative music did not alter sleep latency in the short or the long sleep latency group (repeated-measures ANOVA main effect of music, p=0.31; interaction effect, p=0.12), indicating the ineffectiveness of music on induction of sleep.
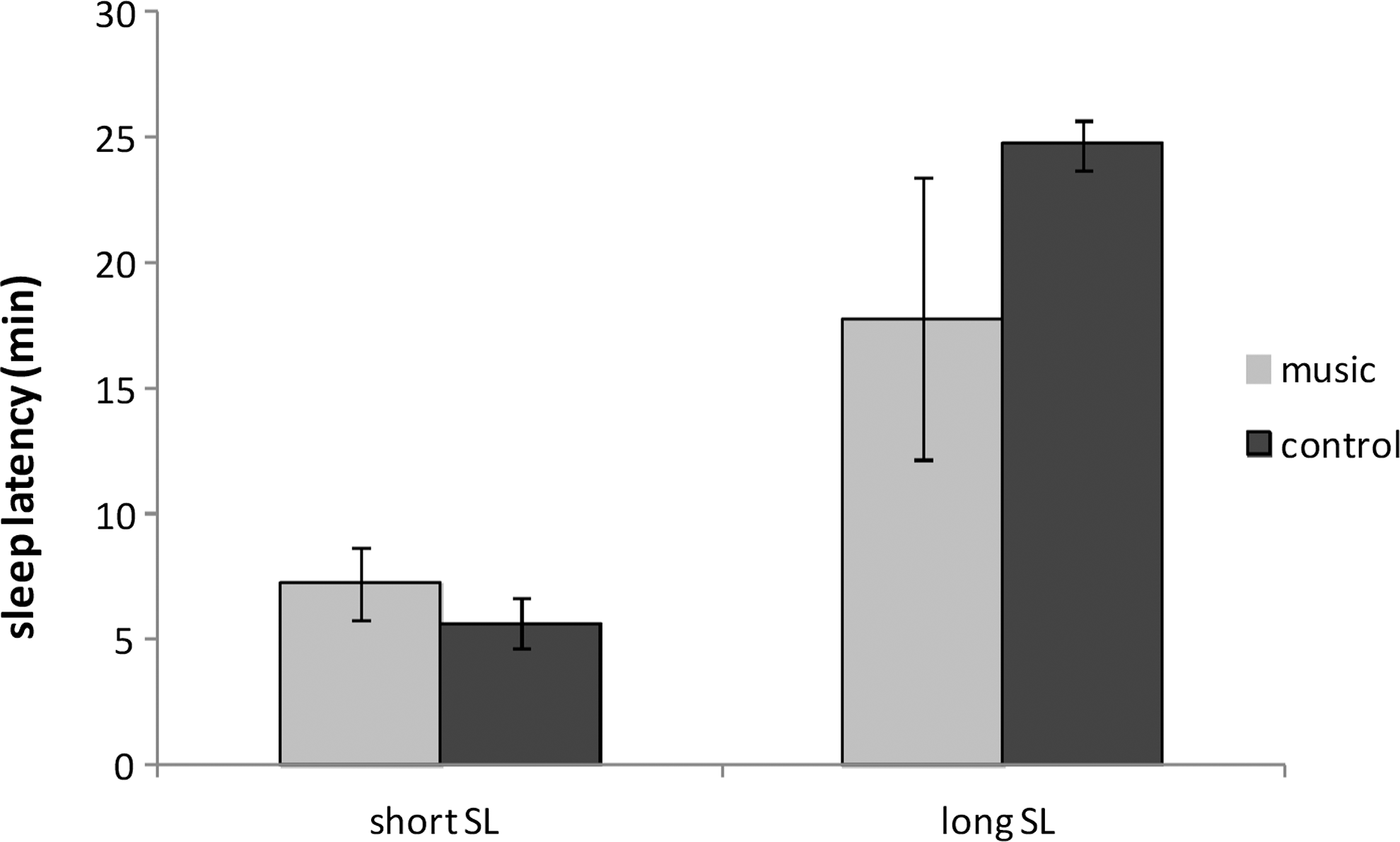
Comparison of the sleep latency between music and control conditions in short and long sleep latency (SL) groups. Music did not alter sleep latency in either the short or the long SL groups (main effect of music, p=0.31; interaction effect, p=0.12). The error bar denotes standard error of mean.
Figure 2 and Table 2 illustrate the changes in duration of each sleep stage, from stage I to IV sleep, and rapid eye movement (REM) sleep. Of note, stage III and IV were combined as deep sleep (stage III+IV, also denoted as slow-wave sleep according to electroencephalographic characteristics) in Figure 2E. The statistical results of repeated-measures ANOVA indicate that compared with the control group, music reduced stage II sleep in both the short and long sleep latency groups (main effect of music, p=0.03; interaction effect, p=0.87). Most interestingly, music increased stage III+IV sleep only in the long sleep latency group (main effect of music, p=0.15; interaction effect, p=0.02). Although not a statistically significant finding, stage IV sleep also increased in the long sleep latency group (main effect of music, p=0.5; interaction effect, p=0.07). As shown in Table 2, music had no effect on the duration of stage I, stage III, or REM sleep.
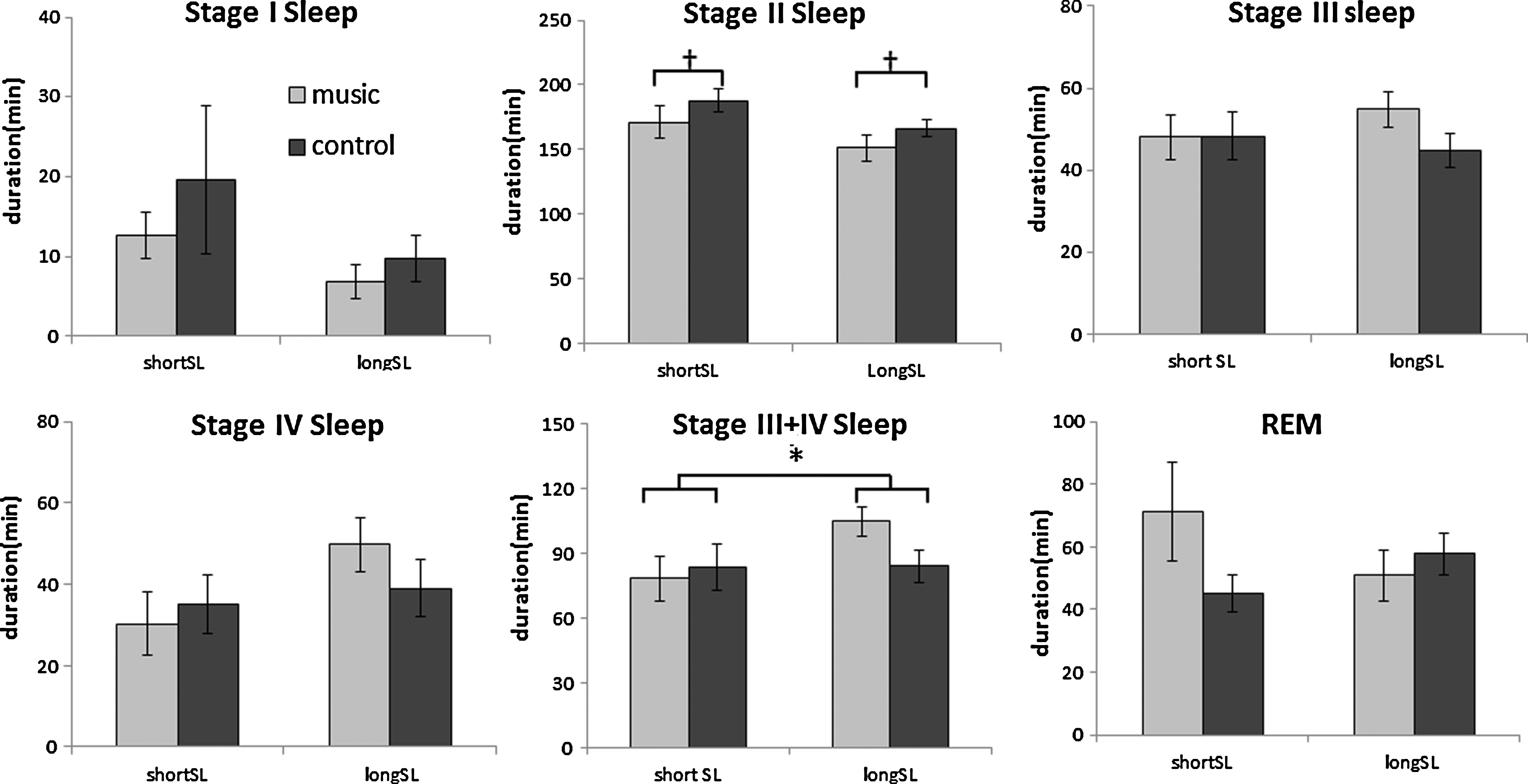
Comparison of duration of each sleep stage between music and control conditions. Music reduced stage II sleep in both the short and the long sleep latency (SL) groups († p=0.03 for main effect of music) and increased stage III+IV sleep only in the long SL group (*p=0.02 for significant condition×group interaction effect). The error bar denotes standard error of mean. REM, rapid eye movement.
Values are expressed as mean±standard deviation.
p<0.05.
Pc, Pg, and Pi, p-value corresponding to condition and group main effects and interaction effect, respectively; REM, rapid eye movement; SL, sleep latency.
Discussion
Normal human sleep is entered through non-REM sleep, which is composed of four stages (I, II, III, and IV) ranging from the lightest to the deepest sleep. REM sleep follows. Typically, non-REM and REM sleep alternate in cycles across sleep. Stage I sleep is the transition from wakefulness to deeper sleep and is the lightest stage of sleep. Stage II sleep constitutes up to 50% of total sleep time and is a true physiologic stage of sleep. Stages III and IV sleep are the deepest sleep and most restorative for body function. 19 The present study found that sedative music was associated with an increase in stage III+IV and reciprocal decrease in stage II sleep in the long sleep latency group. Although not a statistically significant finding, stage IV sleep also increased in long sleep latency group. These findings imply that music benefits the sleep quality of persons with longer sleep latency benefits. To the best of our knowledge, besides the findings reported in the present study, only high-intensity exercise had an analogous effect and increased deep sleep. 22 As a matter of fact, music intervention might be another option for people with long sleep latency to improve their sleep quality, especially for those who are unable to tolerate vigorous exercise.
Several published studies have examined the effect of music on sleep. However, the music selections varied widely, including folk music, soothing classical music, sacred music, or even new age music. 11 –13 To avoid differences in the familiarity of music among individual participants, this study used sedative music that was newly composed by certified music therapists granted by the Certification Board for Music Therapists. The sedative music was composed on the basis of suggestions from behavioral studies comparing responses to stimulating and sedative music. 23 Sedative music is defined in this study as music having a relatively slow tempo, sustained melody passages, nonpercussive timber, legato articulation, and minimal rhythmic activity with an underlying regular beat. 8,24 The pentatonic mode adds a cultural consideration.
Both live music and recorded music have been studied for its effects on sleep. 14,25 A meta-analysis review by de Niet et al. suggests that recorded music played on a compact disc or DVD player, MP3 player, tape recorder, or video recorder can improve sleep quality in patients with sleep issues. 25 The present study used recorded music played on a CD player to standardize the music conditions in the sleep center. The findings showed that recorded sedative music improved sleep quality by prolonging the duration of deep sleep for participants with long sleep latencies. Comparison between live music and recorded music, however, warrants further investigation.
Longer sleep latency is a common problem in patients with insomnia. The current study found that sedative music had no statistically significant effect on sleep latency in either the short or the long sleep latency group. However, sedative music tended to increase sleep latency in the short sleep latency group but decreased latency in the long sleep latency group. Stress leads to sleep disturbance and vice versa, which may become a vicious cycle. de Niet et al. reported that music assists in relaxation and therefore has a beneficial effect on the sleep quality of patients with sleep problems. 25 Thaut and Davis also reported that music relaxes and reduces anxiety in people with longer sleep latencies. 26 However, for people with short sleep latencies who fall asleep easily, listening to music may interfere with falling asleep. 27 According to the theory of the ironic process of mental control, 28 listening to music consumes cognitive capacity, thereby increasing wakefulness and delaying sleep. Therefore, it is possible that the complex effect of music might not elicit a homogeneous effect on sleep latency across individuals.
Chronobiologically, human sleep is a periodic phenomenon manifesting both circadian rhythm (regular sleep–wake cycles that occur on a 24-hour basis) and ultradian rhythm (alternation between REM and non-REM sleep every 90–120 minutes within sleep). Rider et al. reported that music affects the circadian rhythms of various physiologic functions, such as corticosteroid levels. 29 To date no evidence suggests that music changes the circadian rhythm of human sleep. The present study demonstrates the effects of music on sleep structure within the ultradian cycle. The mechanism for regulation of sleep rhythm remains controversial. The underlying mechanism that accounts for the increase in deep sleep by music observed in the present study needs to be further characterized.
A limitation in this study is the fact that it recruited college students with low scores on the PSQI who did not have sleep problems, anxiety, or depression. Therefore, future study in patients with insomnia may be necessary to identify the therapeutic effect of music on sleep.
Conclusions
Sedative music improved the quality of sleep by prolonging the duration of deep sleep, specifically for participants with long sleep latencies. The deep-sleep facilitation effect offers an alternative and noninvasive opportunity to improve sleep in people with short-term sleep problems caused by specific events (e.g., jet lag). The potential application of sedative music among patients with insomnia who have long sleep latencies should be studied further.
Footnotes
Acknowledgments
The authors thank the music therapists Yen-Hsuan Yang, MT-BC, MME, MM, and Yu-Ling Chen, MT-BC, MME, MM, for their contributions of musical improvisation. The authors also thank Yu-Yi Chen for help with conducting the experiment.
Author Disclosure statement
No competing financial interests exist.