
Abstract
Objectives:
This study investigated the effect of acupuncture needles developed for double-blind (practitioner–patient blinding) trials employing a tapping-in method that is commonly used to penetrate the skin in Japanese-style acupuncture.
Design, subjects, and interventions:
An acupuncturist applied a penetrating, a skin-touch placebo, and a no-touch control needle designed to blind both practitioners and patients in the forearm in 80 healthy subjects (patients) by tapping-in method.
Setting:
The setting was a practice room of the Japan School of Acupuncture, Moxibustion and Physiotherapy, Tokyo, Japan.
Outcome measures:
The outcome measures were the acupuncturist's and subjects' guesses at the type of needles and confidence of their guesses on a 100-mm visual analogue scale (VAS). The subjects were asked about pain with needle application.
Results:
The number of correct/incorrect guesses (the latter including unidentified) of the acupuncturist were 73/167 with a confidence of 55.2±16.9 (mean±standard deviation) on the VAS. The subjects identified 148 needles correctly and 92 needles incorrectly, the mean confidence being 71.0±28.4. There were a few penetrating and skin-touch placebo needles that the subjects guessed as “no-touch.” Whereas few of the 80 no-touch control needles were guessed as “penetrating,” 16% of them were guessed as “skin-touch” and 11% were reported as “unidentifiable” by the subjects. Forty percent (40%) of the penetrating needles and 50% of the skin-touch placebo needles did not elicit skin penetration pain.
Conclusions:
The effect of practitioner blinding employing the needles for double blinding with the tapping-in method was satisfactory. It was difficult to blind the subjects when no-touch control needles together with penetrating and skin-touch placebo needles were used.
Introduction
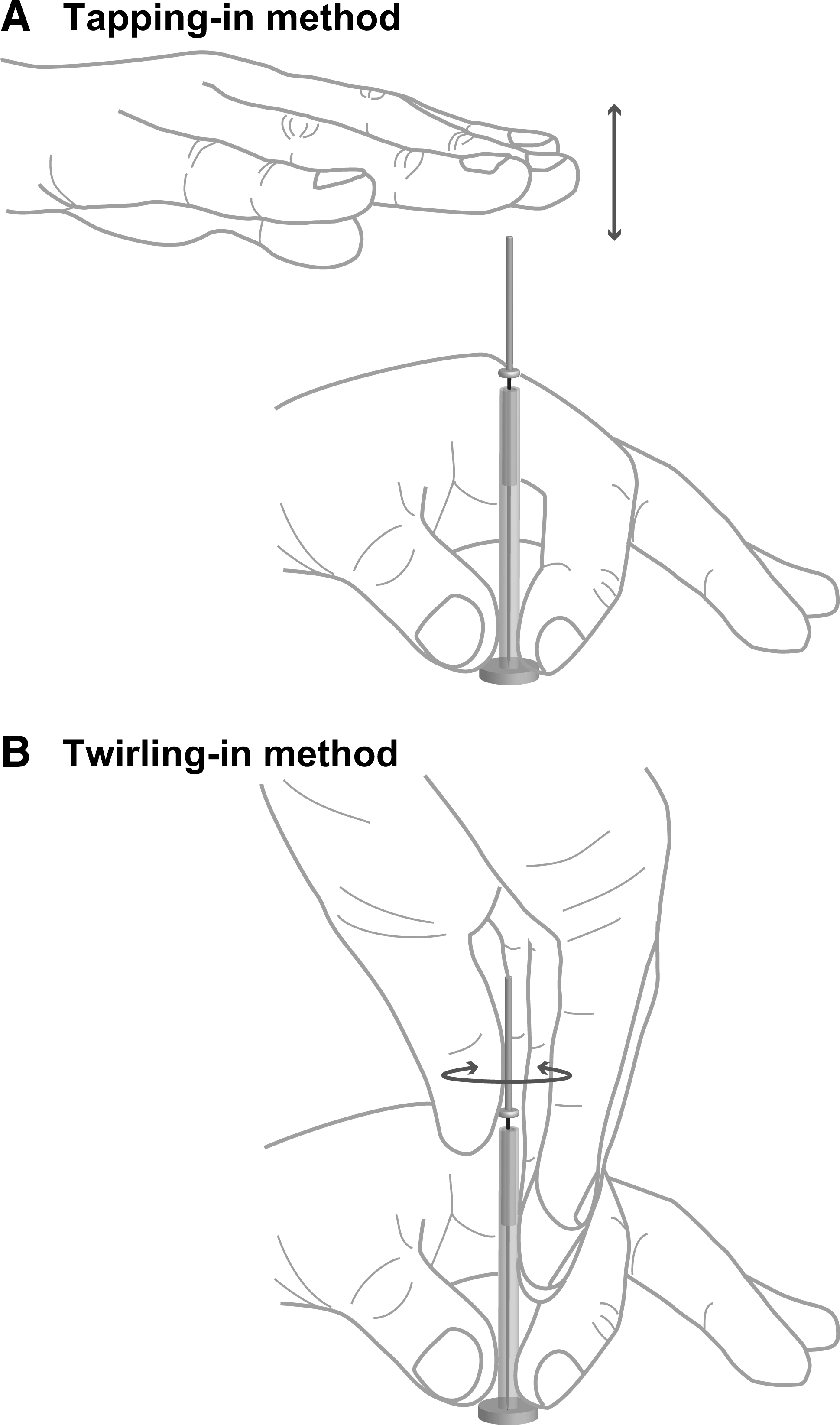
Methods of skin penetration with an acupuncture needle.
The aim of this study was to test whether the needles for double blinding could be effective for practitioner and subject blinding when the tapping-in method was employed. For comparisons between the effect of blinding and pain associated with needle application by the tapping-in method in this article and those by twirling-in method, the data were used when the double-blind needles were applied by twirling-in method in the same subjects, which has been already presented in a separate article. 11
Methods
Participants
Eighty (80) healthy volunteers who were familiar with acupuncture treatment and the concept of de qi (mean±standard deviation [SD] age: 27.1±6.9 years, 48 males, 32 females) from the Japan School of Acupuncture, Moxibustion and Physiotherapy, Tokyo, Japan participated in this study as experimental subjects. 11 The authors recruited the acupuncturist (acupuncture experience: 3 years) on the teaching staff. 11 She had been well trained in how to perform the tapping-in method with the needles for double blinding. 3 –11 Prior to the study, the purpose and format were explained to the subjects and the acupuncturist, and they provided written consent. The study was approved by the Ethics Committee of the Showa University School of Medicine.
The needles for double blinding
The skin-touch placebo needle whose tip presses against the skin but cannot penetrate it and matching the penetrating needle with 5 mm insertion depth, and the no-touch control needle whose tip cannot reach the skin were used; the appearances of these three needles are indistinguishable (Fig. 2). 3 –11 The needle tips of the skin-touch/no-touch and penetrating needle were set just above the lower stuffing and the skin, respectively. The diameter of the needles was 0.16 mm. 3 –11
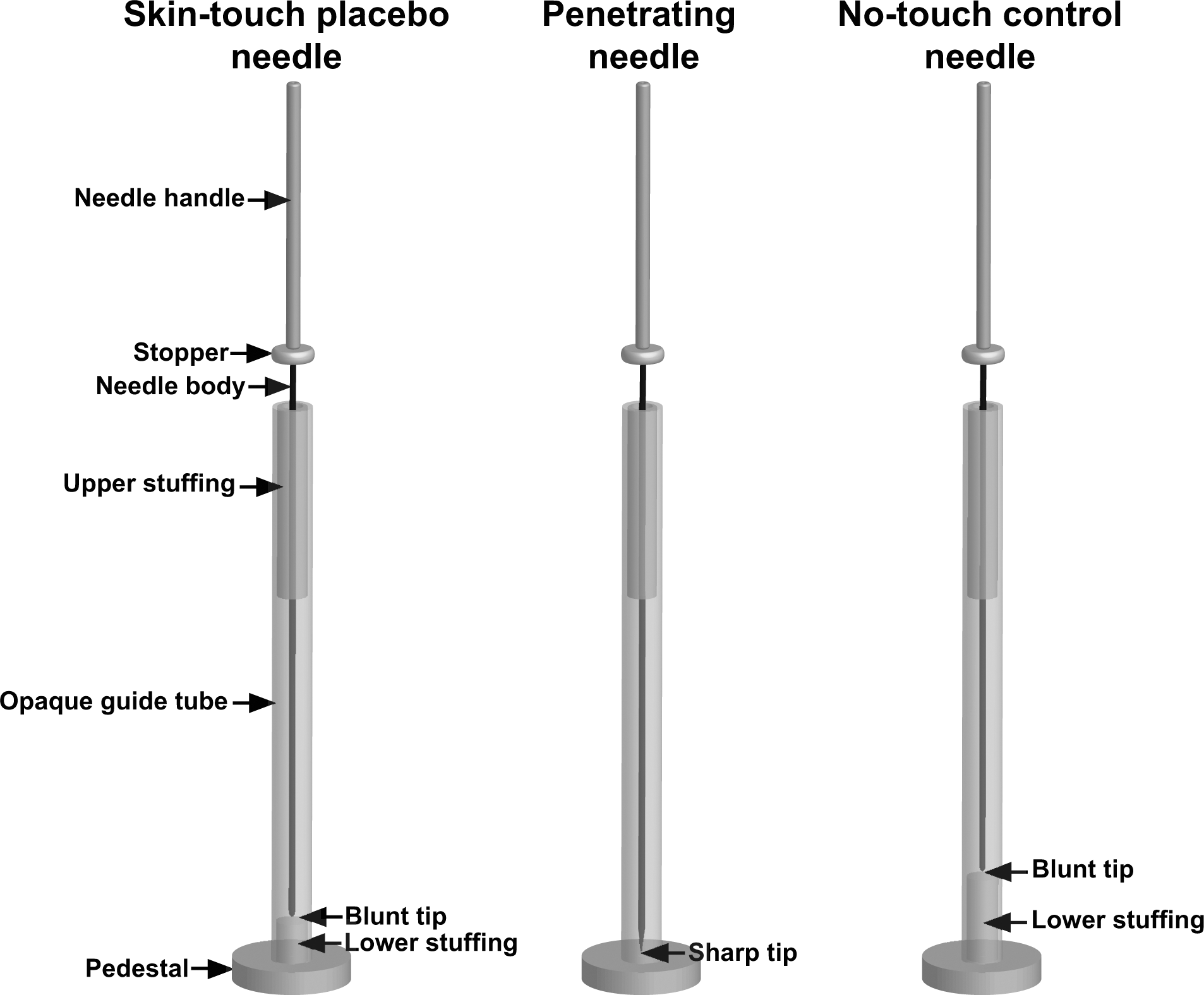
The needles for double-blinding. 10,11 The skin-touch placebo (left), penetrating (middle) and no-touch control needles (right) comprise an opaque guide tube and upper stuffing to give resistance to the needle body during its passage through the guide tube. Each needle has a stopper, which prevents the needle handle from advancing further when the tip of the needle reaches the specified position. The needle body of the skin-touch placebo needle is just long enough to allow its blunt tip to press against the skin, and the needle body of the no-touch control needle is shorter than the guide tube, but the needle body of the penetrating needle is longer than the guide tube by an amount equal to the insertion depth when the needle body is advanced as far as possible. The skin-touch placebo and no-touch control needles contain lower stuffing to give a similar sensation to that of skin puncture and tissue penetration.
Protocol
Before the trial, the 80 subjects and the acupuncturist were informed that penetrating, skin-touch, and no-touch needles would be used. For each subject, one set of three needles was prepared consisting of a penetrating, a skin-touch placebo, and a no-touch control needle sealed in a small opaque container, and then the needles were sterilized.
Three (3) points on the Triple Energizer Meridian on the posterior part of the forearm were used to apply the needles at one fourth (distal point), two fourths (middle point), and three fourths (proximal point) of the length from the skin crease in the posterior surface of the hand joint to the elbow (the olecranon). 11,14
The acupuncturist took a needle randomly from the set of three types of needles in the container and applied the first needle at the distal point. Then, one of the remaining needles was applied at the middle point, and the last one was applied at the proximal point. 11 The acupuncturist applied each needle by tapping the head of the needle handle (tapping-in method) until the stopper made contact with the top of the opaque guide tube (Fig. 1A). Then the acupuncturist pulled the needle out to the initial position by an alternating twirling technique. 11
The acupuncturist applied the three needles in the left forearm of the first and fourth subject and in the right forearm of the second and third subject by the tapping-in method. This pattern was repeated for the remaining subjects. As was reported in the authors' previous article, another set of three needles was applied on the other side of the forearm in the same subject by the twirling-in method. 11
After removal of each needle, the subjects were asked to rate the intensity of pain with needle application on a 100-mm visual analogue scale (VAS), ranging from 0 (no pain) to 100 (the most intense pain imaginable). 5,6,9,11 They also reported whether they felt de qi, which was defined as deep dull pain and/or sensation. 5,6,9,11
To evaluate degrees of practitioner and subject blinding, the acupuncturist and subjects were asked to record whether they thought the needle was “penetrating,” “skin-touch,” “no-touch,” or “unidentifiable.” 3 –11 They then rated their confidence in the guess of the needle authenticity (i.e., the degree of certainty about the guess being correct) on a 100-mm VAS, the endpoints of which were 0 for no confidence and 100 for complete confidence. 5,10,11
Statistical analysis
The χ2 test was used to determine whether the numbers of correctly and incorrectly guessed needles fitted an expected probability. A ratio of correct and incorrect guesses with the tapping-in method was compared with that with the twirling-in method using the χ2 test. The Mann-Whitney U test was used to identify pairwise group differences in the confidence of identifications and the intensity of pain. To compare the tapping-in and twirling-in method in terms of the effect of blinding and pain with needle application, the authors used the data obtained when the twirling-in method was used in the same subjects; these results have already been presented in another article. 11 All statistical analyses were performed using IBM SPSS Statistics 18 (SPSS Japan Inc., an IBM company).
Results
Efficacy of practitioner blinding
For practitioner blinding with the tapping-in method, the respective numbers of correct and incorrect (including unidentified) answers of the acupuncturist were 73 (30.4%) and 167 (69.6%) (Table 1), which fit an expected 1:2 ratio (χ2=0.92, p=0.34). The blind effect was significantly improved compared with the 120 correct and 120 incorrect guesses with the twirling-in method 11 (χ2=19.1, p<0.01).
Bold number indicates correct identification.
VAS, visual analogue scale; SD, standard deviation.
There was no significant difference between the tapping-in (Table 1) and twirling-in method 11 in the acupuncturist's confidence score in making her guesses at the penetrating (p=0.14), skin-touch placebo (p=0.64), no-touch control needles (p=0.33), and the 240 needles overall (p=0.09).
Efficacy of subject (patient) blinding
Of the 240 total needles, the subjects guessed 148 (61.7%) needles correctly when the needles were applied by the tapping-in method (Table 2), which was not significantly different from 160 (66.7%) correctly guessed needles with the twirling-in method 11 (χ2=1.3, p=0.25). However, the overall confidence of the subjects in the tapping-in method (Table 2) was significantly less than that in the twirling-in method (mean±SD: 75.8±26.7) 11 (p=0.03). Of the 80 subjects' guesses at the penetrating needles when the tapping-in method was used, 48 (60.0%) were correctly guessed (Table 2), which was significantly different from 65 (81.3%) correctly guessed needles with the twirling-in method 11 (χ2=8.71, p<0.01). There was no significant difference in the proportions of correct and incorrect guesses between the tapping-in (Table 2) and twirling-in methods 11 for the skin-touch placebo needles (χ2=0.63, p=0.43) and no-touch control needles (χ2=0.0, p=1.0), respectively.
Bold number indicates correct identification.
VAS, visual analogue scale; SD, standard deviation.
Pain on needle application
Using the tapping-in method, 32 (40.0%) of penetrating needles did not elicit pain, which was significantly different from 15 (18.8%) of painless skin penetration with the twirling-in method 11 (χ2=8.71, p=0.01).
For the penetrating-needles-elicited pain, the intensity of pain for 48 (60.0%) needles with the tapping-in method (mean±SD: 15.5±13.9) was not significantly different from that for 65 (81.3%) with the twirling-in method (17.5±19.7) 11 (p=0.57).
With the tapping-in method, 40 (50.0%) skin-touch placebo needles elicited pain as with the twirling-in method; 11 there was no significant difference in the intensities of pain between both skin penetration methods (tapping-in: 10.2±11.3; twirling-in: 11.5±12.0) (p=0.73).
Thirty-six (36; 45.0%) penetrating, 14 (17.5%) skin-touch placebo, and three (3.8%) no-touch control needles elicited de qi, which were very similar to those obtained from the twirling-in method. 11
Discussion
Employing the tapping-in method, practitioner blinding with the needles for double blinding was distinctly improved comparing with the twirling-in method. 11 For the penetrating needles, subject (patient) blinding with the tapping-in method was improved comparing with the twirling-in method. 11 Although subject blinding was improved by using the tapping-in method comparing with the twirling-in method 11 in terms of the confidence in their guesses, it was difficult to blind the subjects when no-touch control needles together with penetrating and skin-touch placebo needles were used.
Practitioner blinding was almost perfect in terms of the number of correct and incorrect guesses, with uncertainty in most correct guesses. This is because the skin penetration with the needle tip could barely be felt by the index finger when using the tapping-in method. Thus, the tapping-in method should be recommended to be used when the needles for double blinding are employed, which makes acupuncture treatment using the needles for double blinding become similar to ordinary acupuncture treatment. However, the tapping-in method with the needles for double blinding called for considerable skill as the acupuncturist acquired in this study because it prevented the needle body from smoothly advancing through the resistance with the upper stuffing in the opaque guide tube to the needle body. Thus, intertester reliability should be tested employing other acupuncturists. Furthermore, it is desirable to ease the handling of these needles by using the tapping-in method for general acupuncturists.
The most important factor of the skin-touch placebo needle to trick the subjects is skin penetration-like pain induced by the skin pressure with the blunt-tip needle. 5,6 By the tapping-in method, it seemed difficult to make subjects believe that they received a penetrating needle because the skin pressure eliciting penetration-like pain with the skin-touch placebo needle was not strong enough compared with that by the twirling-in method. However, the effect of subject blinding with the tapping-in method was not inferior to that with the twirling-in method. 11
For the penetrating needles, the tapping-in method had an advantage for subject blinding comparing with the twirling-in method. The increase in frequency of painless skin penetration with the penetrating needles by using the tapping-in method could make it difficult for the subjects to correctly identify them. This increase also provided evidence of the well-known belief that the tapping-in method is the best way to reduce skin penetration pain with needle insertion. 15 Moreover, it provided a good reason to use the tapping-in method when the needles for double blinding are employed in the clinical study because pain associated with acupuncture treatment is sometimes called an adverse event 16 –18 even if pain with needle insertion seems inherently unavoidable because of its invasive nature.
As with the twirling-in method, 11 the subjects scarcely misidentified no-touch control needles as penetrating, or penetrating needles and skin-touch placebo needles as no-touch with the tapping-in method. It was difficult to blind the subjects when no-touch control needles together with penetrating and skin-touch placebo needles were used because of no skin-touch with the needle tip of the no-touch control needle. Although the no-touch control needles seemed to be unsuitable for double blinding, they may be used as a suitable control for the ritual aspects of acupuncture treatment in future clinical trials. Moreover, approximately 20% of the no-touch control needles were misidentified as skin-touch; this suggests that the no-touch control needle could be a potential tool to estimate whether skin-touch with a blunt tip needle to an acupoint is a “clinically” inert placebo. 11
For the basic limitation of our needle, it should be remembered that any needle for double blinding can neither achieve perfect blinding nor fully reproduce all the conditions of real-life acupuncture; changes in practitioner and/or subject might give rise to different results of “practitioner and patient” blinding. 3,5,6,10,11 In future studies, the blinding effect of the needles with variable insertion depth and using the needle manipulation after the tapping-in method should be tested employing patients in clinical settings.
Conclusions
The effect of practitioner blinding employing the needles for double blinding with the tapping-in method was satisfactory. It was difficult to blind the subjects when no-touch control needles together with penetrating and skin-touch placebo needles were used.
Footnotes
Acknowledgments
The authors thank Ikuo Homma (Second Department of Physiology, Showa University School of Medicine, Tokyo) for his support. The authors also express their appreciation to all the participants of this study. The source of funding was the Educational Foundation of Hanada Gakuen.
Disclosure Statement
NT and the Educational Foundation of Hanada Gakuen possess a U.S. patent 6575992B1, a Canadian patent CA 2339223, a Korean patent 0478177, a Taiwanese patent 150135, a Chinese patent ZL00800894.9 (title: Safe needle, placebo needle, and needle set for double blind), and two Japanese patents: 4061397 (title: Placebo needle, and needle set for double-blinding) and 4315353 (title: Safe needle) on the needles described in this article. NT is a salaried employee of the Educational Foundation of Hanada Gakuen.