
Abstract
Objective:
A randomized, single-center, double-blind, crossover clinical trial investigated the effects of an herbal preparation containing Vernonia cinerea in patients with type 2 diabetes mellitus.
Methods:
48 patients with type 2 diabetes mellitus for longer than 6 months were divided into two groups matched for demographic and paraclinical variables. One group received a standard preparation of V. cinerea for 3 months, followed by placebo for another 3 months, and the other group received treatment in the reverse order. All patients received detailed advice on diet, exercise, and lifestyle modification. Glucose level was documented every 2 weeks, and hemoglobin A1c, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein cholesterol, triglycerides, aspartate aminotransferase, alanine aminotransferase, and creatinine levels were determined at recruitment, 3 months, and study completion at 6 months.
Results:
Glucose, hemoglobin A1c, cholesterol, LDL cholesterol, and triglyceride levels decreased significantly in both groups. No significant differences were seen in aspartate aminotransferase, alanine aminotransferase, or creatinine levels, indicating that use of the herbal preparation had no adverse effect on liver or renal function.
Conclusion:
Herbal treatment with V. cinerea has a beneficial effect on reducing the glycemic state in patients with type 2 diabetes.
Introduction
Traditionally used herbal medicines could be effective alternatives for the treatment of diabetes. Several studies have shown the medicinal and clinical significance of traditional medicinal plants in reducing blood glucose and concomitant complications, which are mainly due to increased oxidative stress and reduced free-radical scavenging ability. 8,9
A large number of people in Bangladesh usually consult with a rural traditional healer about their illness and receive herbal preparations. These preparations consist of various plant parts prepared according to the formula given by the traditional physician. An unani consultant informed us of the antihyperglycemic use of Vernonia cinerea root. He has been in practice for many years and has been prescribing the herbal preparation of this plant for the treatment of type 2 diabetes. V. cinerea (L.) (Asteraceae) is an herbaceous plant commonly called purple fleabane (kuksim in Bengali). The whole plant has several pharmacologic properties; it is used for malarial fever, worms, pain, infections, diuresis, cancer, abortion, and various gastrointestinal disorders. 10 Phytochemical analysis of V. cinerea showed the presence of steroids, triterpenoids, sesquiterpenes, flavonoids, and tannins. 11 The practitioner used the root of this plant to treat diabetes. The root is fat and fleshy, with whitish skin. Interviews with several patients suggest it is apparently effective. Therefore, a clinical study of V. cinerea was undertaken to investigate the antidiabetic efficacy and toxicity of V. cinerea root at traditionally prescribed doses in patients with type 2 diabetes.
Methods
Plant material
Several herbal dosage forms of V. cinerea were available for the treatment of diabetes. The traditional unani practitioner, who was involved in the clinical trial, has been practicing as a traditional healer for more than 10 years. According to his suggestions, V. cinerea root paste at 6 g/d (one 2-g pill three times daily) was chosen as the active medication. The placebo test products were formulated so that they matched the active product except that they contained cellulose fiber as an inert ingredient. The test products (active or placebo) were supplied to patients in identically labeled foil packets containing a 2-g dose of the product.
Study design
This single-center, randomized, placebo-controlled, crossover clinical trial was conducted over a 6-month period (Fig. 1). Patients were randomly assigned to one of two groups by using a computer-generated table of random numbers. Group A (n=24; 11 men and 13 women) received a standard preparation of 6 g/d (one 2-g pill three times daily) V. cinerea root paste (active treatment) for 3 months, followed by placebo in similar form and size for another 3 months. Group B (n=24; 11 men and 13 women) received placebo for the first 3 months and the active treatment for the second 3 months. Both the active treatment and the placebo were to be taken three times a day before a meal. During the study period, the patients were not taking any other medications for diabetes. Adherence to the dosing regimen was monitored by interviewing the patients at each visit and by counting the number of returned unopened packages and number of pills in the container (active or placebo) every 2 weeks. Adverse events were recorded on a standardized recording form. All patients received detailed advice on diet, exercise, and lifestyle modification, as indicated in the guidelines for the management of type 2 diabetes. Patients were advised to report to the traditional healer as soon as possible if they experienced extreme weakness; fatigue; tingling or numbness in their hands, legs, or feet; blurred vision; dry or itchy skin; or frequent infections. Per protocol, patients would be withdrawn from the study if such incidents occurred.
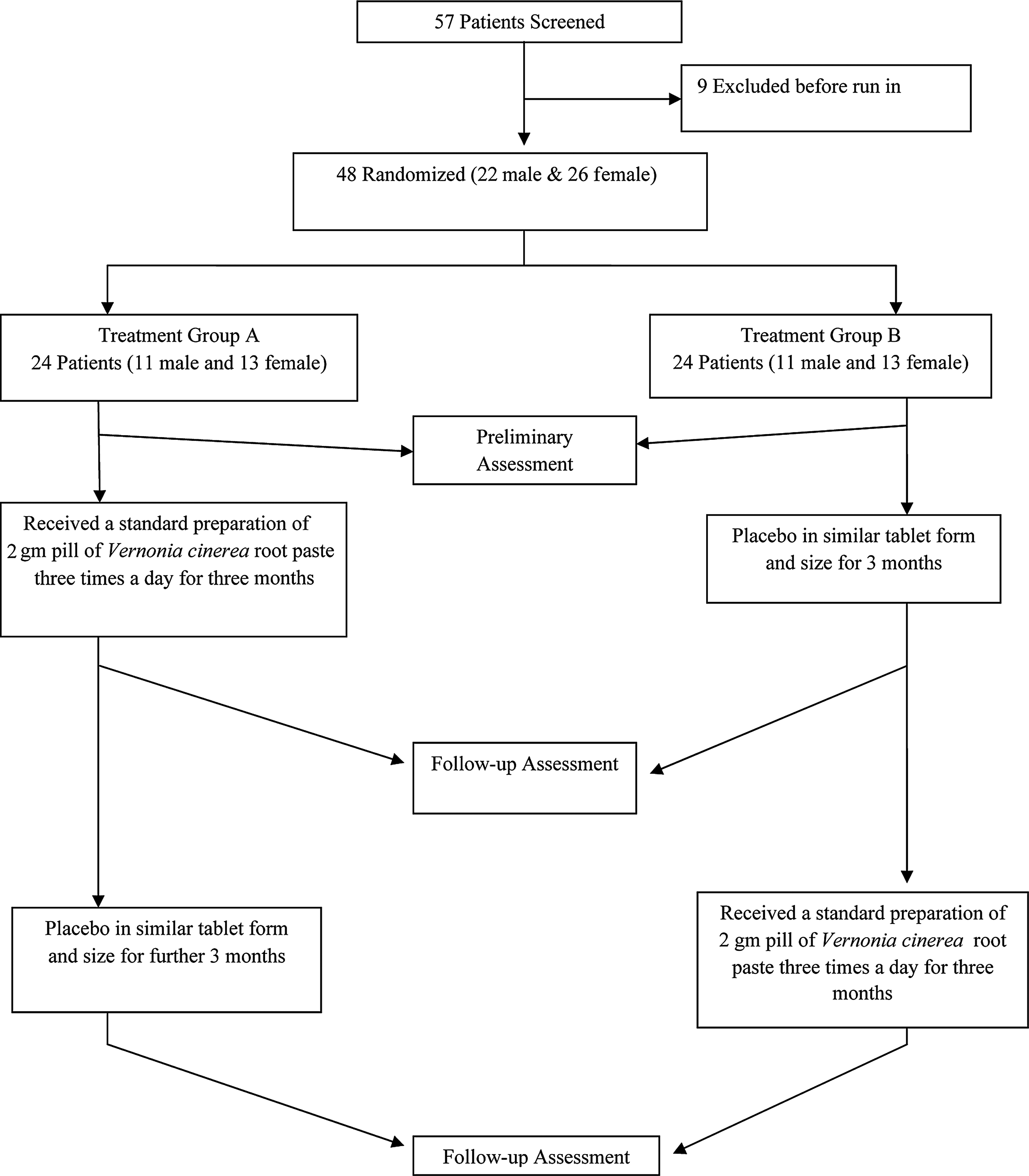
Study flowchart.
Ethical approval
The trial was carried out in accordance with the Declaration of Helsinki and subsequent revisions. It was approved by the institutional review committee. Written informed consent was obtained from each patient before the study.
Participants
A total of 57 patients (25 men and 32 women), aged 40–65 years, who had a confirmed diagnosis of type 2 diabetes according to American Diabetes Association criteria for at least 6 months and were seeking unani treatment were invited to participate in this study. Forty-eight of them (22 men and 26 women) qualified for random assignment to treatment. Patients were excluded from the study if they were receiving lipid-lowering drugs, corticosteroids, lithium, carbamazepine, warfarin, or digoxin; had clinically significant renal, hepatic, gastrointestinal, pulmonary, or thyroid disease; were pregnant or lactating; were women of child-bearing age who were not using contraception; were currently being treated or previously treated for any malignancy; were already receiving treatment with any other preparation containing herbal products; were receiving treatment with other drugs known to affect carbohydrate metabolism (other than standard medications for diabetes mellitus); and were receiving insulin therapy. Also excluded were individuals with a history of myocardial infarction or major surgical procedures within the previous 6 months and those who had a history of allergy to plant materials.
Assessment of efficacy
Fasting blood glucose, glycosylated hemoglobin (HbA1c), total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglyceride, aspartate aminotransferase, alanine aminotransferase, and creatinine levels were determined at recruitment, at 3 months, and at completion of the study at 6 months. Blood glucose levels were determined by an autoanalyzer (Glucometer G-423 S, Bioland Technology, Kowloon, Hong Kong, China) glucose kit immediately after blood sampling. HbA1c levels were determined by a D-10 hemoglobin testing system (Bio-Rad Laboratories, Inc., Hercules, California). All other blood sample variables were measured by a Hitachi 902 autoanalyzer (Hitachi, Tokyo, Japan) using commercial kits. Patients were visited and examined every 2 weeks, and the efficacy of treatment was checked by determination of the fasting blood glucose level.
Assessment of tolerability
All adverse events, reported or observed, were recorded at each visit. Routine physical examination was conducted at each clinical visit.
Statistical analysis
Statistical analysis of the recorded data was performed by independent and paired t-test using SPSS software, version 16.0 (SPSS, Inc., Chicago, Illinois). A p-value<.05 was considered to represent a statistically significant difference.
Results
Demographic and paraclinical characteristics
Table 1 summarizes the demographic and paraclinical characteristics of the two groups at the beginning of the study.
Values are expressed as mean±standard error. Differences with p<.05 were considered statistically significant. No measures in the table had p<.05.
Glucose
The mean (±standard deviation) fasting blood glucose level in group A at the beginning of the study was 189±27 mg/dL. This decreased significantly (p=.04) to 174±44 mg/dL after 3 months of active treatment. After the placebo period, the glucose level was 182±32 mg/dL. In group B, the fasting glucose levels were 182±24 mg/dL initially, 187±35 mg/dL after 3 months of placebo, and 173±31 mg/dL after active treatment (p=.03 for decrease). There was no evidence of a crossover period effect or carryover effect in either group.
HbA1c
The average HbA1c level in group A at the beginning of the study was 10.4%±1.9%. This decreased significantly (p=.02) to 7.8%±2.4% after 3 months of active treatment and was 9.3%±2.0% after the placebo period. The average HbA1c level in group B was 9.1%±1.9% at the beginning of the study, 9.4%±2.4% after placebo administration, and 7.3%±2.0% after active treatment (p=.02 for decrease). There was no evidence of crossover period effect or carryover effect in either group.
Other blood biochemical values
Table 2 summarizes results of the other clinical findings in both groups at the beginning of the study, after 3 months, and at the end of the study.
Values are expressed as mean±standard error. Differences with p<.05 were considered statistically significant. Each group had 24 patients.
p<.05 (statistically significant compared with beginning).
p>.05 (not statistically significant compared with beginning).
HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Safety and tolerability
Weight and systolic and diastolic blood pressure slightly and nonsignificantly decreased in patients receiving active treatment; no significant gastrointestinal adverse effects were reported. Kidney and renal function were also normal, and most patients were satisfied with the therapy.
Discussion
This study investigated the effect of V. cinerea on the glucose profile in patients with type 2 diabetes. V. cinerea treatment significantly decreased fasting blood glucose levels and HbA1c levels in diabetic patients after active treatment in both groups. Administration of placebo did not decrease glucose levels. Although the glycemic improvement was relatively low, this study showed a good trend of hypoglycemic effect, with gradual decrease in blood glucose levels. This finding implies that a longer-term study might show better glycemic improvement.
The study also demonstrated a significant effect of V. cinerea on blood cholesterol profile and triglyceride levels; treatment with placebo in both group showed nonsignificant changes in clinical measures. The absence of any significant changes in aspartate aminotransferase, alanine aminotransferase, and creatinine levels in blood suggest that at the doses given, the extracts did not damage liver or kidney function. Furthermore, the absence of significant gastrointestinal disturbances observed in the present study after V. cinerea administration indicates that the drug was well tolerated and safe at a dose of 6 g/d y (2-g pill taken three times daily) in diabetic patients for 6 months. After 6 months of study, the mean (±standard error) weight was 66.1±1.8 kg in group A and 67.2±1.8 kg in group B, which indicated nonsignificant changes compared with initial weight (Table 1).
The mechanism underlying the glucose-lowering effect of V. cinerea is not clear. Some compounds might have glucose-lowering effects. A recent study showed that methanolic extract of the whole plant of V. cinerea contains n-hexadecanoic acid (42%–88%), 12 and another study confirmed the presence of n-hexadecanoic acid in other medicinal plants with antihyperglycemic properties. 13,14 Palaniab et al. (2010) 14 reported that n-hexadecanoic acid led to restoring of shrinkage of β cells of islets of Langerhans in rats with streptozotocin-induced diabetes. Therefore, we propose that the hypoglycemic effect of V. cinerea could be due to presence of n-hexadecanoic acid, which might restore shrinkage of β cells of islets of Langerhans.
The decreases in HbA1c in this investigation are relatively greater than those in fasting blood glucose level. This finding suggests a primarily postprandial effect and indicates the mode of action via β cells of islets of Langerhans. However, extensive investigation is required. Other secondary effects might have been diminished because of the presence of many active constituents, including flavonoids with antioxidants, that increase cellular glutathione levels and cellular membrane–stabilizing properties. 15 In patients with type 2 diabetes, the elevation of glucose and free fatty acid levels leads to the generation of reactive oxygen species and oxidative stress. 16 These metabolic abnormalities induce not only late diabetic complications but also insulin resistance, β-cell dysfunction, and impaired insulin secretion. 17 V. cinerea, with its powerful antioxidant properties, is active against oxidative stress and may induce a positive effect on diabetic metabolic abnormalities. In support of this hypothesis, several experimental and clinical studies indicate that substances with antioxidant properties have favorable effects on oxidative metabolic derangement of hyperglycemia. 18
In conclusion, the results showed that herbal treatment with V. cinerea helps reduce the glycemic state in patients with type 2 diabetes. The use of this herbal medicine at a dose of 6 g/d (one 2-g pill three times daily) showed no adverse effects during 6 months of therapy. Therefore, V. cinerea could be used as an alternative and complementary treatment of type 2 diabetes, but only after large-scale clinical trials evaluate its long-term efficacy and toxicity in diabetic patients.
Footnotes
Disclosure Statement
No competing financial interests exist.