
Abstract
Objective:
This report of one case illustrates the potential effect of acupuncture therapy in addition to Western medicine for regaining postoperative consciousness in patients with traumatic brain injury (TBI).
Clinical features:
A 65-year-old man experienced a TBI after being involved in a motor vehicle accident. His initial Glasgow Coma Scale (GCS) score was E1V1M2, and brain computerized tomography showed a right-sided subdural hemorrhage. He received emergency medical treatment and underwent craniotomy to remove the lacerated portions of brain as well as subtemporal decompression, followed by a decompressive craniectomy the following day to remove an intracerebral hematoma due to late-onset temporo-parietal rebleeding. Twelve days after surgery, the patient remained in poor condition due to serious complications and the GCS was E2VeM4. His family then underwent counseling and he subsequently received acupuncture treatment.
Intervention and outcome:
This patient was treated with acupuncture three times each week, consisting of strong stimulation at GV26 (Shuigou) and the 12 Well points using the half-needling technique. After 3 weeks of consecutive treatment, his GCS score improved to E4VtM6. In addition, he regained consciousness and could tolerate rehabilitation programs.
Conclusions:
We believe that an experienced physician may use acupuncture as complementary therapy in patients with TBI who fail to regain consciousness postoperatively.
Introduction
Despite improvements leading to more rapid diagnosis and surgical intervention, outcomes in patients with severe head injury remain poor. Mortality rates among patients admitted to the hospital with TBI range from 20% to 40%. One-fifth of patients who survive the injury will have significant long-term neurologic disability. Less than one-third of patients whose best initial Glasgow Coma Scale (GCS) score is ≤8 will have a favorable outcome. 2 Patients whose GCS score is ≤8 and who have abnormal findings on head computerized tomography (CT) following head injury will usually require intracranial pressure monitoring and surgery to evacuate any hematoma. Decompressive craniectomy can be lifesaving, but the prognosis may remain grave. 2
Some studies conducted and published in China have suggested that acupuncture may be beneficial in the acute treatment and rehabilitation of TBI. 3 This paper presents a case of a patient with TBI who underwent craniectomy and removal of intracerebral hematoma and whose GCS score improved from E2VeM4 to E4VtM6 with a restoration to consciousness after 3 weeks of acupuncture treatment, in addition to Western medicine.
Case Report
History and examination
A 65-year-old man in good health with no past medical or surgical history suffered a TBI after a motor vehicle accident on May 26, 2011. He presented with a severe head contusion and was comatose upon arrival to the emergency room. In the emergency room, his first GCS score was E1VeM2, his pupils were dilated to 5/5 mm without a noticeable light reflex, and muscle strength was 4/2/2/1 (right arm/right leg/left arm/left leg). Head CT showed a right-sided subdural hemorrhage over the cerebellar tentorium and falx cerebri with midline shift (Fig. 1).
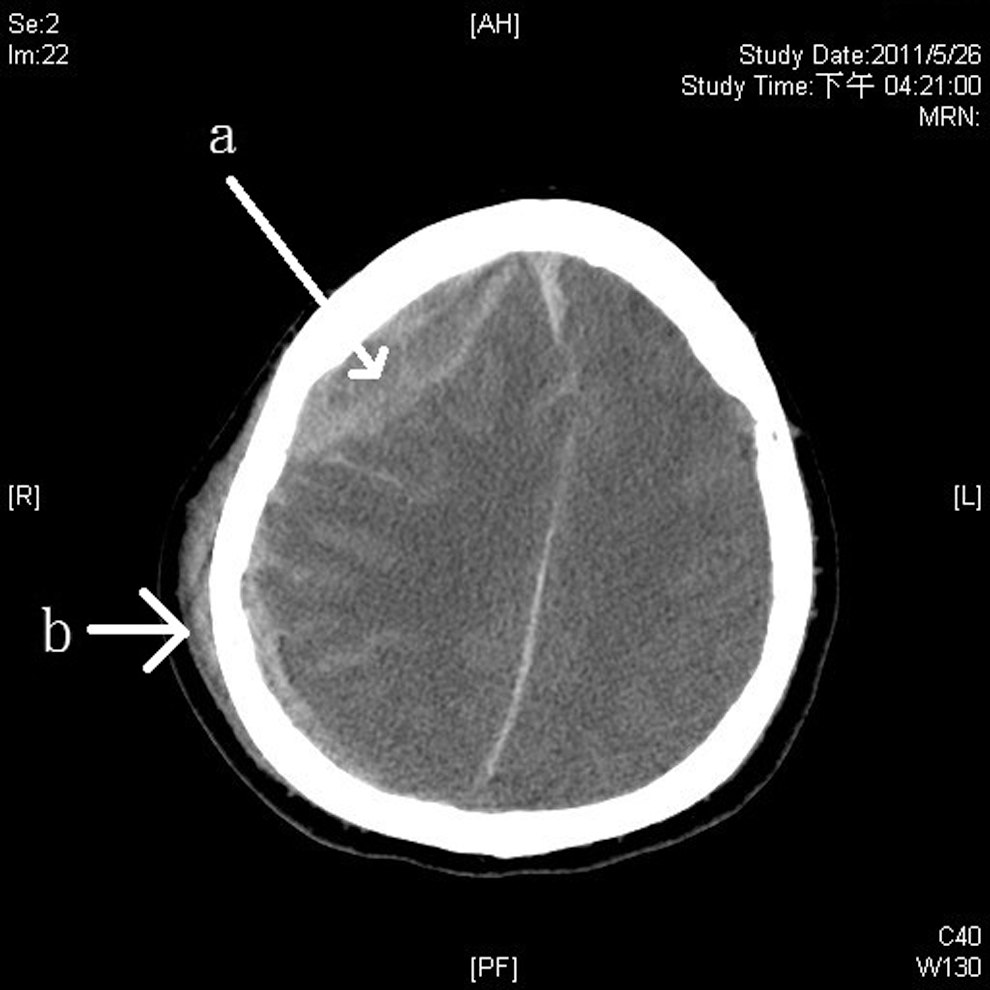
Head computed tomography (CT) reveals right fronto-temporo-parietal subdural hematoma with mass effect
Due to the presence of severe brain edema and the critical condition of the patient, he underwent craniotomy to remove the lacerated portions of the right fronto-temporo-parietal lobes and partial resection of the right temporal tip for decompression. The day following initial operation, tremors were noted, indicating late-onset temporo-parietal rebleeding. Decompressive craniectomy was performed to remove additional intracerebral hematoma and to institute intracranial pressure monitoring in the neurosurgical intensive care unit. The patient did not regain consciousness after the second operation and experienced residual left hemiplegia. The patient remained in poor condition due to development of pneumonia, malnutrition, and electrolyte imbalance due to diarrhea and was dependent on mechanical ventilation due to respiratory failure. Twelve days after the initial operation, the GCS score remained E2VeM4. He was unable to be weaned from the ventilator, and a tracheostomy was performed on June 21, 2011.
Acupuncture therapy and outcome
Acupuncture intervention was suggested as a complementary therapy. The patient's family underwent counseling and the patient subsequently received the first acupuncture treatment on June 8, 2011. He received acupuncture therapy three times per week. Aims of treatment included improvement in consciousness and movement of his left limbs. Each therapeutic session began with strong stimulation at the GV26 (Shuigou) point (at the junction of the upper and middle third of the philtrum). Following the stimulation, a half-needling technique was used that included the 12 Well points of all four limbs. After nine therapeutic acupuncture sessions, the patient's GCS score improved to E4VtM6. Due to the improvements in his condition, he was weaned from mechanical ventilation and transferred to a general medical ward on June 27, 2011. He was subsequently able to begin rehabilitation programs (Fig. 2).
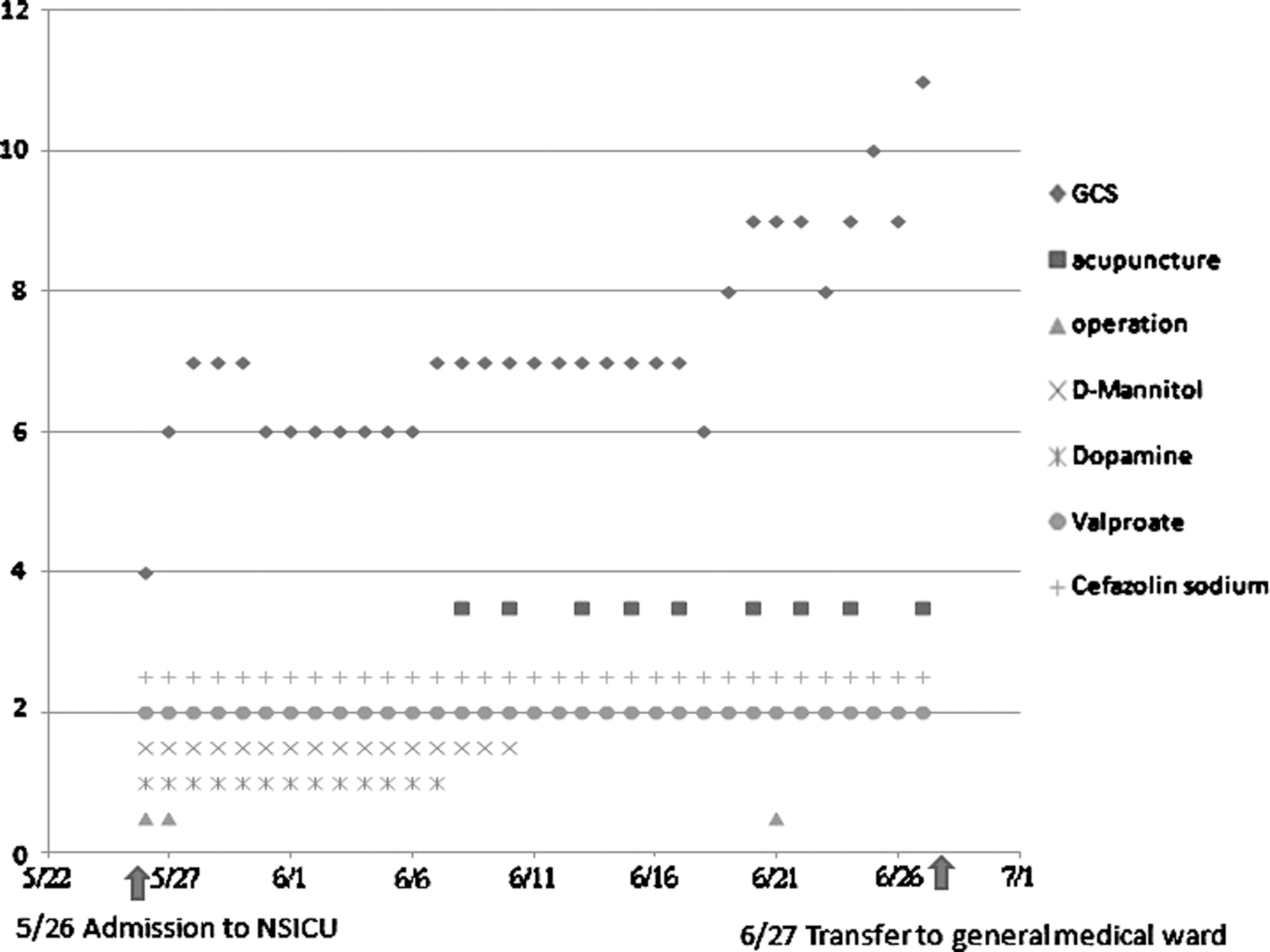
Serial Glasgow Coma Scale (GCS) scores over time and timeline of treatments throughout the patient's course of hospitalization. NSICU, neurosurgical intensive care unit. Graph illustrates timing of surgeries (green triangles), acupuncture treatments (red squares), and medication administration. Time is indicated by month/date and begins at the time of hospitalization. Operations on 5/26 and 5/27 were for head injury and on 6/21 for tracheostomy.
Discussion
Although decompressive craniectomy can be lifesaving for patients with severe TBI, the prognosis may remain grave. Patients who survive the initial injury may experience loss of consciousness and neurologic disability, which may have long-term implications for recovery. We provided pre-acupuncture counseling to the patient's family by explaining that acupuncture is a widely used treatment modality for different neurological disorders, and because TBI has the same pathophysiology as many other neurological disorders, acupuncture may also be beneficial in TBI treatment or rehabilitation. 3 Furthermore, we explained that scalp acupuncture would be avoided to prevent interference with the healing of the operation wound.
Shuigou is the point of intersection for Shouyangming, Zuyangming, and the Governor Vessel; it is an essential point for first aid. Acupuncture on Shuigou can restore consciousness and promote resuscitation. Twelve meridians reach the head, with the exception of the lung and pericardium meridians. Twelve Well points were selected, based on “places where meridian passed, treatments thereby can be reached.” Acupuncture at the 12 Well points can clear the stagnant qi and blood within the meridians, adjust organs, promote harmony within organs, un-impede meridians, balance blood and qi, and promote harmony of yin and yang, thus facilitating the treatment of the disease. 4 For example, a previous study showed that blood-letting punctures at 12 Well points of the hand improved the consciousness of patients with small brain injuries. 5
TBI has various outcomes, which depend on the severity of the insult to the brain. Many patients recover gradually over a prolonged period; however, some studies have reported that patients with severe head injury have a mortality rate of as high as 90%. 2 A study that used electroencephalographic (EEG) reactivity for the prognostic evaluation of consciousness recovery in post-acute brain injury revealed that 92% of the patient group with uncertain progress recovered consciousness within 5 months from EEG recording. 6 Our patient's GCS score improved from E2VeM4 to E4VtM6 with a restoration to consciousness after 3 weeks of acupuncture treatment, in addition to Western medicine. Therefore, acupuncture may have a role in facilitating consciousness recovery.
The patient's muscle strength was 3/1/2/1 (right arm/right leg/left arm/left leg) after craniectomy and 3/2/2/1 when transferred to the general medical ward. A previous study reported on a 10-week acupuncture treatment performed on patients who were stable after neurosurgical operation. The study revealed that early acupuncture can improve the limb motor function of patients with severe head injury. 7 When our patient was finally discharged from the rehabilitation ward on August 20, 2011, his muscle strength was 4/3/4/3. Thus, combining rehabilitation with acupuncture may have helped improve his left limb motor function.
TBI can cause a range of debilitating sequelae that require cognitive, motor, communication, emotional, or behavioral rehabilitation of varying intensities and durations. In a study that used acupuncture in combination with point-injection therapy in posttraumatic coma patients, the GCS value in the treatment group was higher than that of the control group, but with no statistical significance (p>0.05). 8 Electroacupuncture therapy has been shown to promote consciousness in patients with long-term coma due to severe craniocerebral trauma. The average awake time and awake rate were 40.1 days and 73.3%, respectively, in the observation group, which were better than the respective values of 51.8 days and 28.6% in the control group. 9
Acupuncture has been shown to be effective in improving prolonged coma after brain surgery and also improving muscle contractures induced by long periods of bed rest. A slight increase in cerebral blood flow (CBF) along with the recovery of consciousness was induced following acupuncture therapy, suggesting a strong connection between CBF and symptomatic improvement. 10 The addition of acupuncture therapy to conventional treatment for patients who fail to regain consciousness after TBI without serious complication can enhance brain activation and restore consciousness, leading to better therapeutic outcomes and increased recovery and cure rates. 11 –15
The results of the various studies suggest that acupuncture is efficacious for the acute treatment and/or rehabilitation of TBI. However, the low methodological quality of the studies renders the results questionable and does not allow us to definitely conclude the efficacy and safety of acupuncture in the acute treatment and/or the rehabilitation of TBI. The beneficial role of acupuncture for these indications remains uncertain. Further research with high-quality trials is required. 3
Conclusions
Acupuncture at the GV26 and 12 Well points was associated with the recovery of postoperative consciousness and shortening of healing time for this patient with TBI in poor condition due to serious complications. An experienced physician may use acupuncture as a complementary therapy in surgically treated patients with TBI who fail to regain consciousness. Thus, better outcomes can be achieved through the combination of Western and Chinese treatments, expediting and boosting treatment efficacy and ultimately leading to decreased medical costs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.