
Abstract
Objectives:
The objective of this study was to elucidate the safety and effectiveness of acemannan, a polysaccharide extracted from Aloe vera, in the treatment of oral aphthous ulceration.
Design:
A skin patch test was performed on 100 healthy subjects, and 0.5% acemannan in Carbopol® 934P NF (Lubrizol Corporation, USA) was applied to the oral mucosa of the lower lip of 50 healthy participants 3 times/day for 7 days. Oral examinations and blood tests measuring liver and kidney function were performed prior to, and following, 7 days of application to assess the side-effects of acemannan when used on oral mucosa. Another 180 subjects with recurrent aphthous ulceration randomly received one of three treatments: 0.1% triamcinolone acetonide (HOE Pharmaceuticals, Malaysia), 0.5% acemannan in Carbopol® 934P NF, or pure Carbopol® 934P NF. Medications were applied to the ulcers 3 times/day for 7 days. Measurements of ulcer size and patient satisfaction ratings were performed on days 2, 5, and 7. Pain ratings were recorded daily.
Results:
No subjects exhibited allergic reactions or side-effects to acemannan. There were no significant differences between the blood test values before and after 7 days of acemannan application. The effectiveness of acemannan in reducing ulcer size and pain was superior to that of control, but inferior to that of 0.1% triamcinolone acetonide. Patients were mostly satisfied with 0.1% triamcinolone acetonide and acemannan treatment.
Conclusions:
Acemannan can be used for the treatment of oral aphthous ulceration in patients who wish to avoid the use of steroid medication, although the effectiveness was not comparable to that of 0.1% triamcinolone acetonide.
Introduction
Currently, there is no curative management of RAU available. The aims of treatment are the reduction of pain and inflammation, as well as promoting healing, but do not include preventing the recurrence of the ulcers. Thus, the treatment of choice for these lesions is topical steroid application. 9 Antimicrobial agents, topical analgesics, immunosuppressive agents, anti-inflammatory agents, and laser therapy have all been used to treat RAU. 4 Because of the possible adverse effects from steroid treatment and the potential for the development of secondary oral candidiasis from long-term steroid use, herbal medicines have been advocated as an alternate form of treatment.
Several natural products have been investigated for the promotion of wound healing. Aloe vera (Aloe barbadensis Miller) has long been used to treat various skin conditions such as cuts, burns, and eczema. 10 –13 Aloe vera has been proven to stimulate dermal wound healing in rats by increasing collagen and glycosaminoglycan synthesis. 14 Aloe vera's beneficial properties may be attributed to mucopolysaccharides present in the inner gel of the leaf, especially acemannan (β-(1,4)-acetylated polymannose). 15 Acemannan has been reported to increase epithelial and fibroblast proliferation through the activation of growth factors. 14 Animal experiments also confirmed the effect of acemannan in accelerating oral wound healing and the immunomodulatory activity of Aloe vera gel. 16,17
The safety of acemannan has been shown in an animal study of rats fed with acemannan for 14 days. 18 Increasing levels of proliferating cell nuclear antigen, keratinocyte growth factor-1, vascular endothelial growth factor, and type I collagen have been reported when acemannan was used on rat oral wounds. 16,19
The aims of the present study were to investigate the potential for allergic reaction to acemannan when used on human skin, to assess local and systemic side-effects of acemannan when used on normal oral mucosa, and to measure the effectiveness of acemannan in the treatment of oral aphthous ulceration.
Materials and Methods
Aloe vera (Aloe barbadensis Miller) was obtained from a local herbal supplier in Bangkok, Thailand, and the specimen (No. 051101) was deposited in the Museum of Natural Medicines, Faculty of Pharmaceutical Sciences, Chulalongkorn University (Bangkok, Thailand).
Acemannan was extracted from fresh Aloe vera pulp gel by homogenization, centrifugation, and alcohol precipitation as previously described. 20 To remove small proteins and monosaccharides, acemannan was placed into a 10,000 molecular weight cut off semipermeable dialysis bag for 24 hours and then lyophilized. The molecular weight of acemannan was analyzed by high-performance liquid chromatography (Shimadzu, Kyoto, Japan). The isolation was performed by using a column (Shodex Sugar KS-804; Showa Denko K.K., Yokohama, Japan) and compared with a P-82 standard (Showa Denko K.K., Yokohama, Japan). The monosaccharide composition and structure of the polysaccharide was determined by gas chromatography-mass spectroscopy, and 13 C nuclear magnetic resonance spectroscopy as previously described. 21,22 These analyses were consistent with prior results, confirming the polysaccharide extracted from fresh Aloe vera gel was acemannan. 21,22 The yield of the acemannan extraction was about 0.2%.
Acemannan in Carbopol® 934P NF was prepared by diluting acemannan in distilled water and then it was autoclaved and mixed with Carbopol® 934P NF. The pH was adjusted to be in the range of 6.5–7.
The present study was conducted with informed consent following protocols approved by the Chulalongkorn University Faculty of Dentistry's Committee on Investigations Involving Human Subjects. The study population comprised 150 healthy volunteers and 180 subjects with recurrent aphthous ulceration. Acemannan used in the study was extracted from Aloe vera and passed cellular and animal safety screening.
To investigate whether acemannan caused an allergic reaction when used on human skin, 100 healthy volunteers (50 females and 50 males) were recruited to participate in the study. One-half percent acemannan in Carbopol® 934P NF (Lubrizol Corporation, Cleveland, OH, USA) was loaded in two Finn chambers (Epitest, Tuusula, Finland) and pure Carbopol® 934P NF was loaded in two other chambers. The chambers were then applied to the subjects' upper backs. After 48 hours, the chambers were removed and 15 minutes later, any reaction was scored according to the International Contact Dermatitis Research Group standard. Scoring was conducted again 24 hours later. The subjects and examiner were blinded as to which chambers contained acemannan.
To assess the local and systemic side-effects of acemannan when used on normal oral mucosa, 50 healthy volunteers (25 females and 25 males) were recruited to participate in the study. Subjects were instructed to apply 0.5% acemannan in Carbopol® 934P NF with a diameter of 1 cm 3 times per day for 7 days on their lower labial mucosa. Oral examination and blood tests were performed before and after 7 days of drug administration. The blood parameters assayed were serum glutamic oxaloacetic transaminase, serum glutamic pyruvic transaminase, alkaline phosphatase, T protein, T bilirubin, albumin, blood urea nitrogen, and creatinine.
To measure the effectiveness of acemannan in the treatment of oral aphthous ulceration, 180 subjects with recurrent aphthous ulceration randomly received one of three treatments: 0.1% triamcinolone acetonide (HOE Pharmaceuticals, Malaysia), 0.5% acemannan in Carbopol® 934P NF, or pure Carbopol® 934P NF. The medications were applied to the ulcers 3 times per day for 7 days. Measurement of the ulcer size was performed before treatment and on days 2, 5, and 7. Ulcer diameters were measured using a calibrated dental probe with millimeter markings, and the sizes of the ulcers were calculated using formulas for the surface area of a circle or ellipse. The ulcers were photographed alongside a visual reference of known size, and the images were analyzed using computer software (Image-Pro Plus version 4.5 for Windows, Media Cybernetics, Rockville, MD, USA).
All ulcers were diagnosed by an oral medicine specialist. Traumatic, infectious, and immunologic-related ulcers were excluded (Table 1). If there was more than one ulcer, the ulcer with the easiest access was selected for investigation. Subjects and investigator were both blinded to the treatment type. When a subject developed RAU more than one time (at least 1 month apart), they reentered the study, receiving a different medication.
Pain ratings using a visual analog scale consisting of a 100-mm horizontal line between the endings marked “no pain” and “unbearable pain” were recorded daily. On the last day, subjects were asked to rate their satisfaction with the medication used on a scale of 0 to 10. Each subject was interviewed at each visit by the investigator regarding the emergence of any adverse reactions.
Statistical Methods
Background and demographic data were summarized with descriptive statistics. One-way analysis of variance was performed to compare group differences in the satisfaction rating, ulcer size, and pain level at each monitoring point. All data were analyzed using SPSS software (SPSS 12.0 for Windows; SPSS, Chicago, IL). A p-value of ≤0.05 was considered to be statistically significant. Outliers were excluded from the database.
Results
A representative lesion in this study is seen in Figure 1.

An aphthous ulcer with two size references.
Skin patch test
Assaying the reaction to acemannan when used on human skin revealed that no subjects had any positive allergic reaction. One subject (number 7) had mild irritation (discrete patchy erythema, no infiltration) on all treated areas (Fig. 2) 24 hours after the removal of the Finn chambers. This subject had a history of metal allergy and possibly had an allergic reaction to the aluminum component of the Finn chamber. When 0.5% acemannan in Carbopol was applied directly onto the subject, no reaction was observed.
Skin reaction assay results, Subject 7.
Blood tests
The results of assessing the local and systemic side-effects of acemannan when used on normal oral mucosa revealed that there were no significant differences in any blood parameter examined (p>0.05) when compared between before and after the 7-day application of the medication.
Subject satisfaction with the treatment of oral aphthous ulceration
The three groups of subjects—0.1% triamcinolone acetonide, 0.5% acemannan in Carbopol® 934P NF, and pure Carbopol® 934P NF—were well matched as to age, sex, and size and pain level of ulcerations at the first visit.
Assessment of the effectiveness of acemannan in the treatment of oral aphthous ulceration showed that subjects who received 0.1% triamcinolone acetonide were mostly satisfied with the medication with an average satisfaction score of 8.3, followed by acemannan with an average score of 7.5, and control with an average score of 6.5. Analysis by analysis of variance revealed that the differences were significant (p≤0.05), and the Bonferroni test confirmed that subjects were significantly more satisfied with 0.1% triamcinolone acetonide and acemannan than control. The difference in satisfaction scores between subjects receiving acemannan and 0.1% triamcinolone acetonide did not reach statistical significance.
Seventeen (17) subjects were treated with all three medications. When these subjects were asked to pick which medication they preferred for treatment, 76% of the subjects selected acemannan as their treatment of choice. Eighteen percent (18%) of the subjects who received all three medications chose triamcinolone, while 6% picked the control medication.
Daily pain rating for the treatment of oral aphthous ulceration
When daily pain ratings were compared between the three groups, it was found that 0.1% triamcinolone acetonide markedly reduced the pain level from day 2 onward when compared to acemannan and control (Fig. 3). Acemannan had an immediate effect in relieving pain symptoms, but its long-term effect was not comparable to that of 0.1% triamcinolone acetonide. There was a significant difference in pain reduction by 0.1% triamcinolone acetonide compared to the other groups. Subjects receiving acemannan reported lower levels of pain during the entire 7 days when compared to control, although the difference did not reach statistical significance.
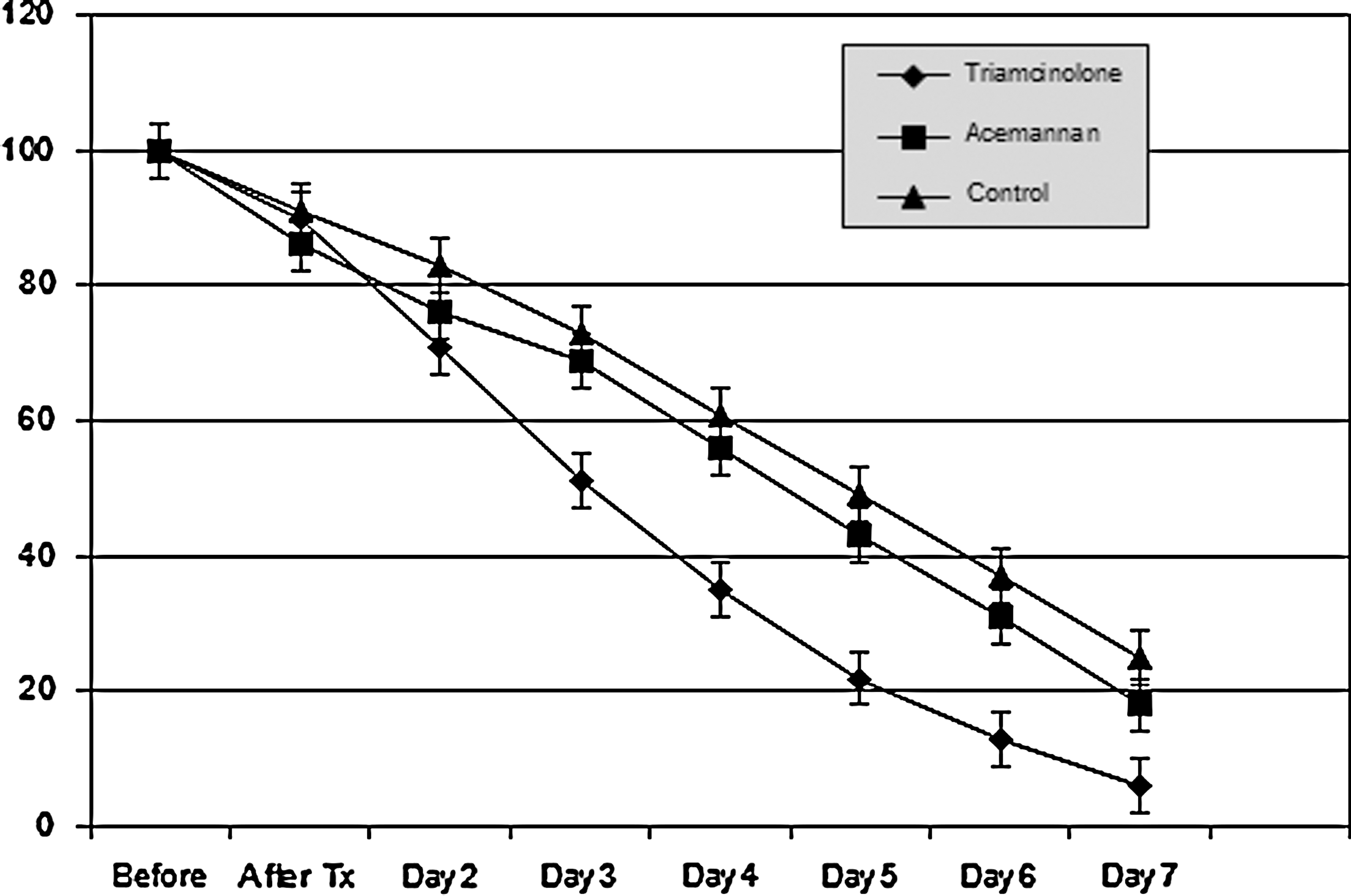
Daily pain ratings (adjusted to percentage).
Ulcer size reduction in the treatment of aphthous ulceration
Analysis of wound reduction among the three medications applied revealed that ulcer size was more than 30% smaller in the 0.1% triamcinolone acetonide group on day 5 compared to the control group (Fig. 4). This reduction in size was greater in the 0.1% triamcinolone acetonide group on day 7. At day 2, acemannan treatment reduced ulcer size to the same degree as 0.1% triamcinolone acetonide. At days 5 and 7, acemannan reduced the ulcer size less than 0.1% triamcinolone acetonide, but the difference was not significant. However, the reduction of ulcer size by acemannan was significantly different from that of control (p≤0.05). Statistical analysis of ulcer size reduction in each group of subjects revealed that 0.1% triamcinolone acetonide and acemannan significantly reduced the ulcer size when compared to baseline while no significant reduction of ulcer size was found in the control group.
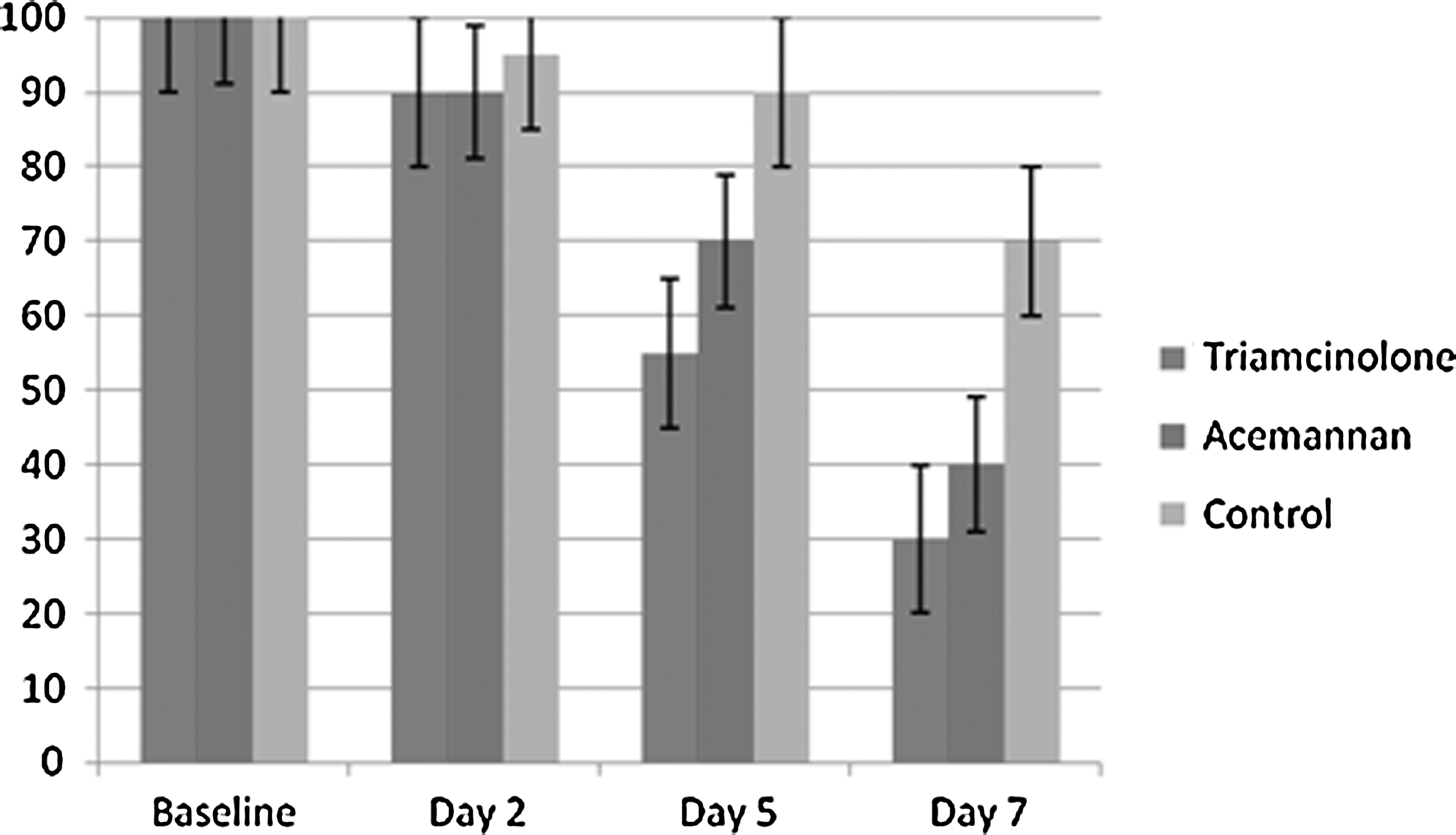
Ulcer size reduction. Numbers represent percentages.
Discussion
In the present study, we evaluated the use of acemannan, extracted from the gel of Aloe vera, as a topical treatment of aphthous ulceration. As no subjects experienced any adverse reactions to the use of acemannan either extraorally or intraorally, we concluded that acemannan is safe to be used on human skin and oral mucosa. Acemannan was found to be effective in reducing the size of, and pain associated with, aphthous ulceration.
Ulcer size, pain level, and patient satisfaction of the medications applied in the treatment of oral aphthous ulceration were evaluated in this study. These are the main issues in the selection of medication for the treatment of RAU. The findings from the present controlled, randomized, double-blind study indicate that acemannan treatment reduced ulcer size and alleviated pain during the 7-day treatment regimen for MiRAU, although pain was not significantly reduced when compared to control. Interestingly, although subjects who used triamcinolone rated their satisfaction toward the medication higher than the ratings by the subjects who used acemannan, subjects who used all three medications preferred acemannan to triamcinolone. This could stem from a soothing feeling from the Aloe vera gel. The results of this study were not as dramatic as those reported by Sasithanasate et al. in 2008 19 and Jettanacheawchankit et al. in 2009 16 on the treatment of rat palatal wounds. The wounds made in those studies were larger (4 mm) and improvements that were more obvious were found with acemannan treatment. Naturally occurring ulcers like RAUs tend to much smaller in size early in the lesion's time course than those created in these studies. Moreover, those studies were performed on rats' palates, which is not a characteristic site for RAUs. Since palatal mucosa is not movable, disturbances to the ulcers were much lower and this may have contributed to the more definitive outcomes they observed.
One limitation of the present study was the measurement of the ulcers. Since ulcer size reduction and pain relief are not the only signs of improvement of healing wounds, depth reduction and reduced levels of inflammation should also be measured. Thus, future study should create criteria for evaluation of these aspects as well.
The present study, to the authors' knowledge, is the first clinical trial using acemannan on recurrent aphthous ulcers. Although acemannan significantly reduced ulcer size, the precise mechanism whereby acemannan induces wound healing is still unknown. The effectiveness of acemannan in the treatment of RAU that was observed in this study could be mediated through anti-inflammatory effects, wound healing promotion, and immunomodulation as shown in Figure 5. 23

Potential modes of action of acemannan. CT, connective tissue; PMN, polymorphonuclear.
Based on the molecular weight and sugar structure of acemannan, acemannan could bind to a receptor on the cell surface and induce an intracellular signaling pathway. 14
Conclusions
The present study indicates that acemannan can reduce recurrent aphthous ulcer size significantly more than control. While its effectiveness is not comparable to that of 0.1% triamcinolone acetonide, acemannan might be suitable for patients who wish to avoid the use of steroid medication.
Footnotes
Acknowledgment
This work (AS549A) was supported by the Higher Education Research Promotion and National Research University Project of Thailand, Office of the Higher Education Commission, and Government Research Fund. We would also like to extend our heartfelt gratitude to Dr. Kevin Tompkins for his assistance in reviewing this article.
Disclosure Statement
No competing financial interests exist.