
Abstract
This is the first report of the successful treatment of advanced biliary tract cancer with gemcitabine single-agent chemotherapy in combination with Juzen-taiho-to (JTT), a Japanese traditional herbal medicine. An 84-year-old woman was referred to our hospital with general fatigue and appetite loss; she was diagnosed with advanced biliary tract cancer and accompanying colonic invasion and hepatic metastasis. The patient's response to combination chemotherapy was extremely good, and her tumors disappeared. Recent studies have confirmed the occurrence of spontaneous and induced antitumor immune responses, carried out by tumor-infiltrating lymphocytes in the tumor microenvironment. The availability, antigen presentation, and proliferation of these immune cells are increased by cytokines such as granulocyte macrophage colony-stimulating factor (GM-CSF) and interleukin (IL)-2. Recently, JTT has gained recognition as a biological response modifier that has stimulatory effects on systemic immune responses such as enhancement of cytokine expression (GM-CSF, IL-2, etc.). In addition, some chemotherapy agents, such as anthracyclines and gemcitabine, are effective boosters of the immune response through tumor-specific antigen overexpression after apoptotic tumor cell destruction. These findings suggest that JTT enhances the antitumor effects of gemcitabine, in particular its tumor-specific effects on immune response, and these drugs are a good combination for advanced biliary tract cancer therapy.
Introduction
According to the recommendations of the National Comprehensive Cancer Network (NCCN), 3 palliative care, entry into a clinical trial, or systemic chemotherapy with 5-fluorouracil (5-FU) or gemcitabine (GEM) should be prescribed for this patient group. To date, many phase II studies have reported some benefit of chemotherapy, but no single regimen had been adopted as a standard of care because of the small size and low power of the studies. Generally, when used as a single agent, the objective response rate (ORR) to chemotherapy is 10%–30%. 4 In single-agent therapy, GEM demonstrated moderate efficacy (17.5% partial response rate) with manageable toxicity in patients with BTC. 5 Recently, results from randomized phase III studies (ABC-02, BT-22) have demonstrated that patients receiving a GEM-cisplatin combination had a significantly longer progression-free survival and overall survival (11.7 compared with 8.1 months; HR 0.64 [95% CI 0.52 to 0.80]; log rank p<0.001) 6 than GEM single agent with an acceptable toxicity. 6,7 Despite these findings, the effect of chemotherapy on survival or ORR is still not sufficient, and the development of additional regimens is required.
Advanced BTC patients commonly have significant comorbidity, advanced age, intercurrent sepsis, and poor performance status. In addition, supportive care and therapy are important therapeutic options to reduce the toxicity and increase the efficacy and feasibility of chemotherapy. Recently, the use of complementary and alternative medicines has become more popular in many countries. Japanese traditional herbal medicine (Kampo medicine) can be used easily because it mainly comprises granular essence style drugs. In Japan, generally, 86.3% of practicing physicians have used Kampo medicines at one time or another as a treatment for various patients' symptoms. 8 Co-administration of Kampo medicine with chemotherapy can reduce side effects and improve the general condition of patients. Juzen-taiho-to (JTT) is a formula of Kampo medicine. Traditionally, JTT has been administered to patients with anemia, anorexia, or general fatigue. Recently, it has been reported that JTT plays a role as a biological response modifier (BRM) and has a stimulatory effect on hematopoiesis and anticancer immune responses, mainly via the enhancement of cytokine expression. 9 –11
Therefore, the induction of a synergistic effect between classical chemotherapy and JTT on the antitumor immune system is a potentially useful and safe therapeutic strategy for BTC. In our hospital, if patients request it or therapeutic indication is shown, we perform Kampo therapy in combination with or without conventional modern medicine in cooperation with Kampo medicine specialists from another hospital that specializes in Kampo therapy, with the consent of IRB committee or approval of the national health insurance. Herein, we report a case of advanced BTC successfully treated by GEM single-agent chemotherapy in combination with JTT.
Case Report
An 84-year-old woman was admitted to our hospital because of general fatigue, high fever, and appetite loss. Seven years previously, she had been diagnosed with cerebral infarction and type 2 diabetes. Physical examination revealed a body temperature of 39.0°C, a blood pressure of 83/44 mm Hg, a heart rate of 76 beats/min, and a body weight of 49 kg. She was conscious and alert, and mild pale conjunctiva was found. Auscultation revealed moist rales in the left-inferior lung field and a cardiac murmur. Her abdomen was soft and flat with an indolent palpable mass over the right hypochondrium. Laboratory examinations revealed a hemoglobin level of 10.3 g/dL, a white blood cell count of 4500/μL (neutrophils, 53.4%; lymphocytes, 35.3%), a C-reactive peptide concentration of 12.5 mg/dL, an albumin concentration of 2.3 g/dL, a total bilirubin level of 0.25 mg/dL, aspartate aminotransferase levels of 16 IU/L, alanine aminotransferase levels of 10 IU/L, alkaline phosphatase levels of 310 IU/L, γ-glutamyl transpeptidase levels of 100 IU/L, serum amylase levels of 24 IU/L, and a glucose level of 74 mg/dL. Serum levels of carbohydrate antigen 19-9 (CA19-9) and carcinoembryonic antigen (CEA) were 21 U/mL and 6.8 ng/mL, respectively. Chest computed tomography (CT) showed a consolidation of the bilateral posterior lung field, which was diagnosed as bilateral pneumonia. Abdominal CT disclosed a large contrast-enhanced liver mass, an enlarged gall bladder, and involvement of the transverse colon (Fig. 1). The liver tumor measured 6 by 8 cm, and the gall bladder measured 7 by 5 cm at its greatest points (Fig. 1). The brush cytology of biliary strictures during endoscopy was revealed to be class IIIb (data not shown), but biopsy could not be performed. Based on these assessments, we diagnosed the patient with advanced BTC (invasive type) with colonic invasion, hepatic metastasis, and accompanying bilateral pneumonia. According to the TNM classification, the disease was staged as IV, which is an inoperative stage. Initially, the patient received antibiotics for treatment of the pneumonia. Due to severe appetite loss, she had to receive nutritional support by intravenous hyperalimentation. She was administered tazobactam/piperacillin (13.5 g/d for 10 days), which resulted in improvement of infectious symptoms. For the treatment of advanced BTC, GEM (1000 mg/m2 at 1, 8, and 15 days) in combination with JTT (Tsumura Kampo granulated extracts; 7.5 g/d, 30 min before every meal every day) was administrated in three cycles over 3 months. This treatment resulted in complete remission, as detected by abdominal enhanced CT (Fig. 2); the liver tumor and colon involvement disappeared, and the gall bladder was dramatically decreased in size. Generally, the most frequently reported (more than 10% incidence) grade 3–4 drug-related adverse events with single GEM administration in a previous clinical trial were infection (15.9%), transaminitis (13.6%), and neutropenia (also 13.6%). 12 Therefore, we initially wondered whether our patient would experience severe neutropenia (grade 4) or infection. However, only grade-2 granulocytopenia, a significant adverse event according to the National Cancer Institute-Common Toxicity Criteria (NCI-CTC, Ver. 3), was observed; the patient did not require administration of granulocyte colony-stimulating factor (G-CSF) or antibiotics during each of the three treatment cycles. She recovered gradually and was able to eat within about 2 weeks of the first chemotherapy cycle. Six months after treatment, complete remission has been maintained.
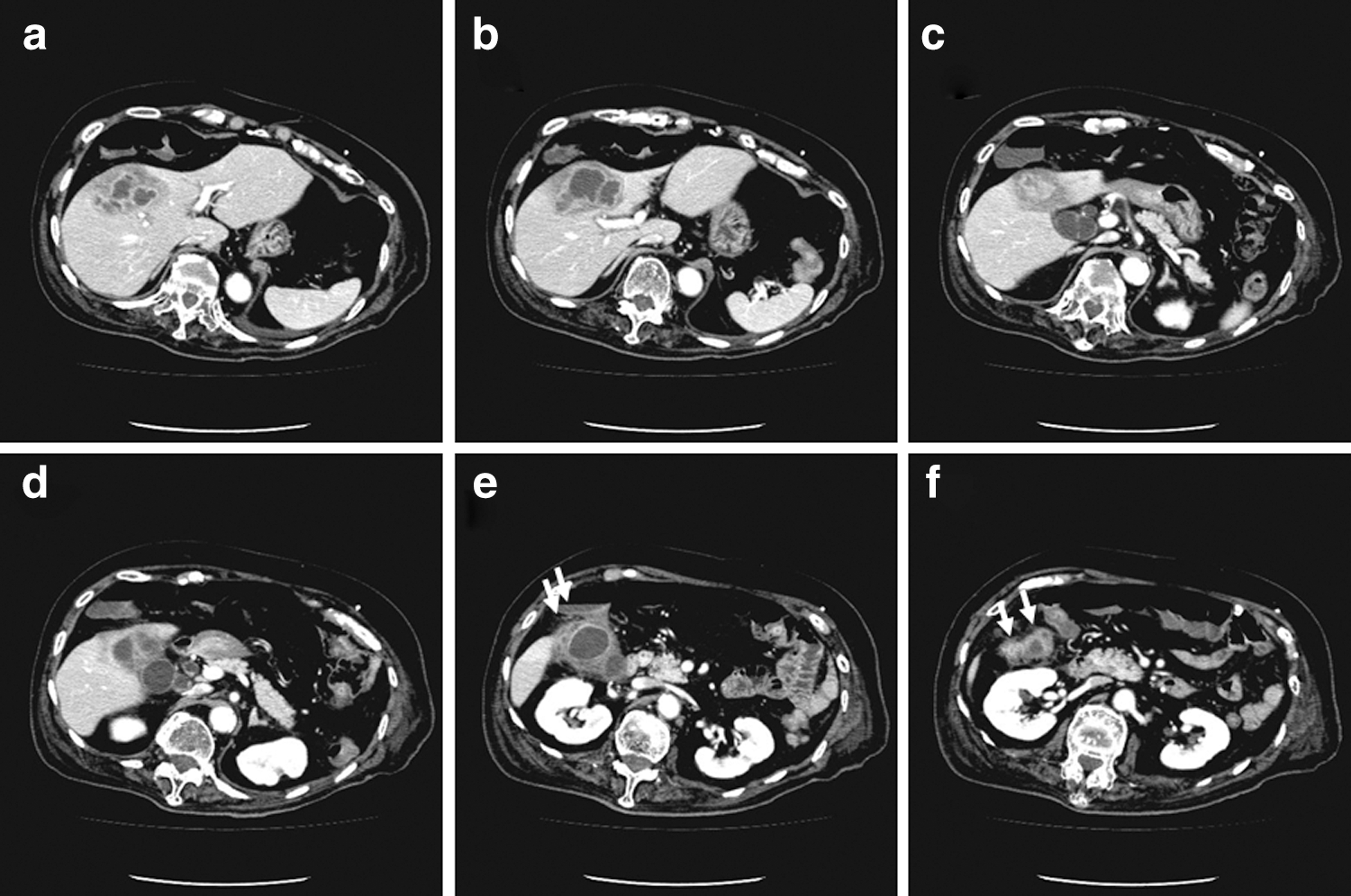
Abdominal computed tomography (CT) images obtained before combination chemotherapy.
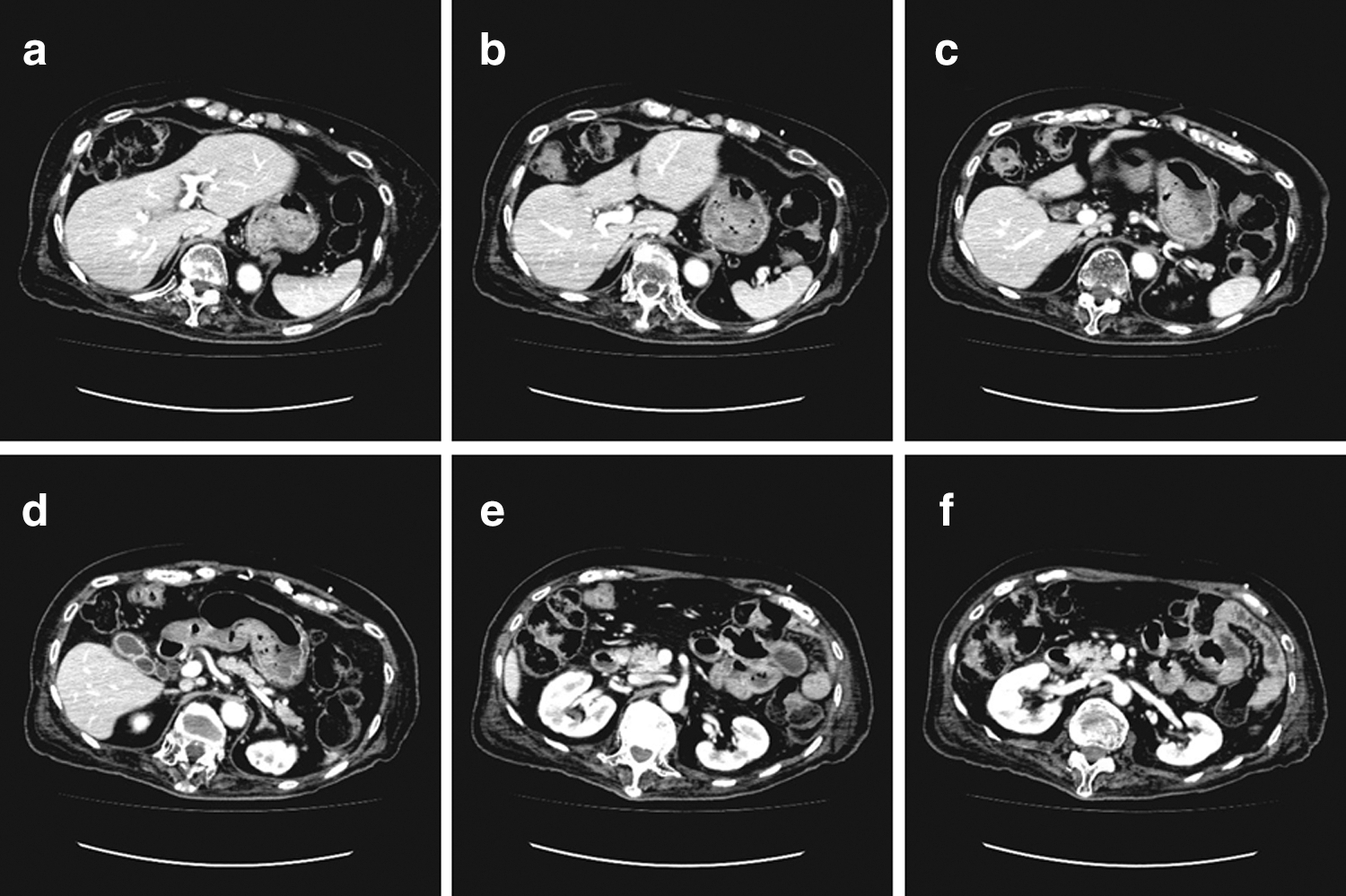
Abdominal CT images obtained after three courses of combination chemotherapy.
Discussion
Chemotherapy plays an important role in treating advanced BTC and contributes to improvement in survival and QOL. However, despite advances in chemotherapy regimens, its effect is limited to a partial response. Surgical resection is generally not feasible even after intensive standard chemotherapy, and advanced BTC still has a poor prognosis. Thus, strategies for more effective reduction of BTC tumors are required.
Stimulation of the dormant anticancer immune system is now attracting the attention of researchers, with the aim of increasing the antitumor effect of chemotherapy. Generally, cancer can be thought of, in part, as an abnormal tolerance of the immune system to the uncontrolled proliferation of cells. Tumor cells develop successfully as result of evading antitumor immune forces in the tumor microenvironment. Thus, decreasing tumor immune tolerance is the objective of cancer immunotherapy. Recently, the distribution of tumor-infiltrating lymphocytes (TILs) within tumor cell islets have reported to show a clear interaction between the host immune system and the tumor; this correlates with better clinical outcome in several types of neoplasia, including ovarian cancer and breast cancer. 13 Previous studies have confirmed the occurrence of spontaneous and induced antitumor immune responses, indicated by the presence of TILs in the tumor microenvironment. 13,14 TILs are lymphocytes isolated from the inflammatory infiltrates present in and around surgical resection samples of solid tumors and are composed of tumor-specific cytotoxic T lymphocytes (CTLs), natural killer (NK) cells, and dendritic cells. The availability, antigen presentation, survival, and proliferation of these immune cells are increased by cytokines such as GM-CSF and interleukin (IL)-2. 15 Indeed, GM-CSF and IL-2 have been evaluated in clinical trials as immune “boosters” in the treatment regimen for solid tumors such as advanced colon cancer and locally advanced breast cancer. 16,17 In addition, some specific chemotherapy agents, such as anthracyclines and GEM, are also effective boosters of the immune response through tumor-specific antigen overexpression after apoptotic tumor cell destruction. 16 –18 Therefore, it is assumed that there is a synergistic link between anthracyclines or GEM and the use of immunotherapy agents such as synthetic cytokines, in which TILs play an important role. However, as with the development of many nascent pharmacological strategies, the occurrence of adverse events such as anemia, fever, or general fatigue generates barriers to successful therapeutic applications. Such obstacles have delayed the introduction of several synthetic cytokines.
On the other hand, Kampo medicines are already known to enhance phagocytosis, cytokine induction, antibody production, and antitumor activity with or without additional chemotherapy. Moreover, co-administration of Kampo medicines with chemotherapy or radiation therapy can reduce the side effects of these treatments and improve the general condition. 19,20 Therefore, such herbal medicines have gained recognition as BRMs. Recently, JTT has been recognized as a BRM that stimulates the immune response against cancer by enhancing cytokine induction. 9,11 JTT consists of 10 crude components obtained from natural herbs described in Table 1 from the 2006 Japanese Pharmacopoeia. 21 Ginseng radix is one of these components; its botanical origin is the root of Panax ginseng (C.A. Meyer). Ginsan is a polysaccharide extracted from Panax ginseng. Recently, ginsan has been reported to stimulate normal lymphoid cells to proliferate and produce cytokines such as IL-1, IL-2, interferon (IFN)-γ, and GM-CSF. 22 –24 In addition, pharmacological evaluation using a pharmaceutically homogeneous preparation of JTT has shown that this herbal formula affects not only the hematopoietic systems but also the systemic immune functions of T and B cells, macrophages, and NK cells. 25 –27 These findings suggest that in the present case, JTT effectively boosted the patient's antitumor immune response by inducing cytokines, enhancing antitumor effectiveness of GEM, and reducing adverse effects of chemotherapy such as myelosuppression, all of which led to a significant clinical synergistic effect.
In order to derive various useful effects from Kampo medicine, it is important that oriental traditional medicines should be used after confirming that they are suitable for the identified Sho of the patient. Sho, a term used in oriental traditional medicine, refers to the particular pathological status of a patient evaluated by a traditional diagnostic procedure and is patterned according to the patient's constitution and symptoms, amongst other considerations. 28 According to Sho criteria, JTT has been used for patients similar to the current patient, who have been diagnosed with Kyo-sho (in Japanese, this means deficiency syndrome) of both Ki (in Japanese, this means vital energy) and Ketsu (a Japanese concept referring to blood, hormones, the autonomic nervous system, and other regulatory functions of the body's internal environment). Namely, Ki-Kyo-Sho indicates mainly the symptom of weakened general condition such as general fatigue, loss of appetite, or mental depression, while Ketsu-Kyo-Sho describes dry skin, anemia, or cold extremities. JTT has been used traditionally for treatment of Ki-Ketsu-Ryo-Kyo-Sho (Ryo means “both” in Japanese). In our case, the Kampo diagnosis Sho and its relatedness to JTT use were important.
In conclusion, despite further investigations being necessary, this case report suggests that the combination of GEM-JTT may be worth researching systematically to determine whether it may be useful to enhance antitumor effects, reduce the toxicity of chemotherapy, and maintain general condition in a larger patient population. Moreover, compared with Western drugs such as synthetic or recombinant products, Kampo medicine is generally characterized by a low frequency of adverse effects and a low cost. Thus, chemotherapy combined with appropriate Kampo medicine can also contribute to a lower medical cost to cancer patients by reducing the use of antibiotics, blood transfusion, and G-CSF products.
Footnotes
Author Disclosure Statement
All authors have stated that no competing financial interests exist.