
Abstract
Background:
A previous case study showed that Guasha, an ancient manual therapeutic technique, could exert hepatoprotective effect in a human chronic active hepatitis B carrier (active-CHB) by modulating the liver enzymes, cytokines, and heme oxygenase-1 (HO-1). The present study serves as a control to the aforementioned case report. The controls were chronic inactive carriers (inactive-CHB) and noncarriers of hepatitis B (NCs). Besides showing a difference in biochemical markers between controls and the previously reported active-CHB case, the asymptomatic condition in both inactive- and active-CHB offers an excellent control for the patient's expectation about Guasha's efficacy. The purpose of this case study was to investigate whether hepatoprotective biochemical markers previously measured in active-CHB in response to Guasha were also present in controls.
Participants and Methods:
Four inactive-CHB and nine NC participants were included. Each participant received a 15-minute Guasha treatment. Blood samples were obtained immediately before Guasha (day 0) and after Guasha (days 2, 5, and 7). Biochemistry values for liver function, HO-1, and T-helper (Th) cytokines were determined from blood tests. Neither the participants nor the investigator who administered Guasha were aware of the blood test results until after all data were collected for all participants.
Results:
In both inactive-CHB and NC participants, liver function, serum HO-1, and Th1/Th2 cytokines did not significantly differ before and after Guasha.
Conclusions:
In contrast to results in active-CHB patients, Guasha did not induce any significant modulation of liver enzymes, HO-1, or cytokines in inactive-CHB and NC participants. The current results suggest that a Guasha-induced hepatoprotective effect depends on the inflammatory event or clinical stage of chronic hepatitis B. Because both active and inactive carriers were completely unaware of their liver status at the time of receiving Guasha, the research protocol is effective in discounting the model that attributes the Guasha therapeutic efficacy to a placebo effect due to participants' expectations.
Introduction
Guasha, also known as coining, 2 is an ancient manual therapeutic technique broadly practiced in Asia to reduce inflammation and a host of other disorders. 3 It applies unidirectional “press-stroking” on a lubricated body surface to create transitory therapeutic petechiae. 4 Guasha had been used for chronic neck pain, breast engorgement, and functional problems with impaired movement. 5 –8 In our previous case report 9 on the hepatoprotective effect of Guasha in an asymptomatic active carrier of chronic hepatitis B (active-CHB), biochemical analysis showed a decline of liver enzymes (alanine aminotransferase [ALT] and aspartate aminotransferase [AST]), indicating a transient reduction in the inflammatory markers of liver injury in the patient, a modulation of T-helper (Th)1/Th2 cytokines (including interferon-γ and interleukin [IL]-4, −5, and −10), and an elevated plasma heme oxygenase-1 (HO-1). Our result is consistent with the report of HO-1 upregulation after Guasha in a healthy transgenic mouse model, 10 which showed that given the raised transitory petechiae, Guasha was considered a natural inducer of HO-1. In liver disease models, HO-1 can enhance the catabolism of heme to yield biliverdin/bilirubin, carbon monoxide, and free iron. 11,12 HO-1 is known to protect tissue through its anti-inflammatory and antiapoptotic action. 13 Previous studies on acute and chronic hepatitis B animal models 14 showed that the upregulation of HO-1 repressed HBV replication and reduced liver injury.
In the present study, we studied liver function, serum HO-1, and Th1/Th2 cytokines before and after Guasha in chronic inactive carriers of hepatitis B (inactive-CHB) and in noncarriers (NCs) as the controls to the active-CHB patient in our previous case report. We hypothesized that Guasha would induce modulation of liver enzymes, HO-1, and Th1/Th2 cytokines in both NCs and inactive-CHB participants, but such modulation was different from what was measured in the previously reported active-CHB case. Because hepatitis B reactivation can be asymptomatic 1 in a subset of active-CHB patients (as it was in our patient), no difference in expectation over Guasha could be measurable in our study of active-CHB versus inactive-CHB participants. Neither the chronic hepatitis B carriers nor the investigator who administered Guasha were aware of the blood test results or the participants' hepatic status during the study period.
Materials and Methods
Participants
Thirteen male participants were included. Their hepatitis status was defined by the level of HBV e antigen on an HBV test. Four of them were inactive-CHB (mean age±standard deviation, 29.75±11.12 years; mean body–mass index, 22.18±4.76 kg/m2), and the remaining 9 were NCs (age, 25.11±3.69 years; body–mass index, 24.33±4.20 kg/m2). Their HBV status was confirmed by the normal levels of ALT, AST, and alkaline phosphatase (ALP) on liver function tests at the end of the study (Table 1). Results on ultrasonographic examination of the liver were normal, with no fibrotic or cirrhotic changes. None of the participants had known systemic diseases, were taking regular medications that affect the levels of liver function and cytokines, or were taking any antiviral drugs before or during the study period. The day the participants received Guasha was defined as day 0. Immediately before Guasha, blood samples were collected for the liver function test and the measurement of HO-1 and Th1/Th2 cytokines. After Guasha, participants underwent another three sessions of blood tests on days 2, 5, and 7 for liver function, HO-1, and Th/Th2 cytokines. All blood tests were carried out at almost the same time of day on days 0, 2, 5, and 7. A blood sampling at 48 hours is a reasonable choice on the basis of the time course of HO-1 upregulation. 10,15
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CHB, chronic hepatitis B; GGT, γ-glutamyltransferase; HBeAg, hepatitis B e antigen; HO-1, heme oxygenase-1; NC, noncarrier.
Blood tests
The blood samples were immediately separated into plasma by centrifugation. The plasma was processed for the liver function test, which included measurements of total bilirubin, total protein, albumin, globulin, albumin/globulin ratio, ALT, AST, ALP, and γ-glutamyltransferase. The plasma level of HO-1 was measured by using a human HO-1 enzyme-linked immunosorbent assay kit (Assay Designs Inc., Ann Arbor, Michigan). The levels of Th1 cytokines (interferon-γ, IL-2, IL-12, and tumor necrosis factor-β) and Th2 cytokines (IL-4, IL-5, IL-6, IL-10) were measured on a Cytomics FC500 flow cytometer (Beckman Coulter, Miami, Florida) equipped with CXP software, version 2.2, using the Flow Cytomix human Th1/Th2 11plex (Bender MedSystems, Vienna, Austria).
Guasha procedure
Guasha was delivered to the upper back of the patient lying in the prone position by using a stone plate with a rounded edge and skin lubricant (Aquasonic®, Parker Laboratories Inc., Fairfield, New Jersey). The Guasha procedure started at the midline of the patient's back. A smooth, rounded edge was press-stroked into the flesh enough to contact the fascial layer, but not so hard that it caused pain or discomfort. A stroke line was typically 4 to 6 inches long. Stroking was repeated in one direction until the petechiae were raised on that stroke line, typically 8 to 12 strokes, before ecchymosis was produced. Guasha was then continued at the next stroke line directly adjacent to the one before, until the area covered the upper one third of the back. The procedure took approximately 15 minutes.
Statistical analysis
A linear mixed model was used to assess the effect of measurement day (dichotomous variable, days 0, 2, 5 and 7) and hepatitis status (dichotomous variable, noncarrier=0, hepatitis carrier=1) on liver function test results, plasma level of HO-1, and Th1 and Th2 cytokines. This model included a random subject intercept to account for possible within-subject correlation. Analysis using linear mixed models was carried out with SPSS software, version 18.0 (IBM Corp., Armonk, New York), for unstructured covariance type, with the measurement day as a repeated effect. Statistical significance was considered to be present at p<0.05.
Results
Biochemical markers indicating the difference before and after Guasha were significantly different between the control participants in this study (Table 1) and the active-CHB case in the previous study. 9 The levels of HO-1 and ALT (within the normal range) were consistently higher in inactive-CHB participants than in NCs on days 0, 2, 5, and 7 (Fig. 1), but the difference did not reach statistical significance given the current sample size; the HO-1 and ALT levels were not associated with the effect of measurement day of Guasha. There was no consistent changing pattern for the levels of total bilirubin and AST in both inactive-CHB participants and NCs. Table 1 shows that in both inactive-CHB participants and NCs, no significant effects of measurement day and hepatitis status were found on liver function, HO-1 levels, or levels of Th1/Th2 cytokines (p>0.05). Biochemical analysis of the plasma samples from the remaining inactive-CHB participants and NCs showed no detectable levels of any cytokine measured.
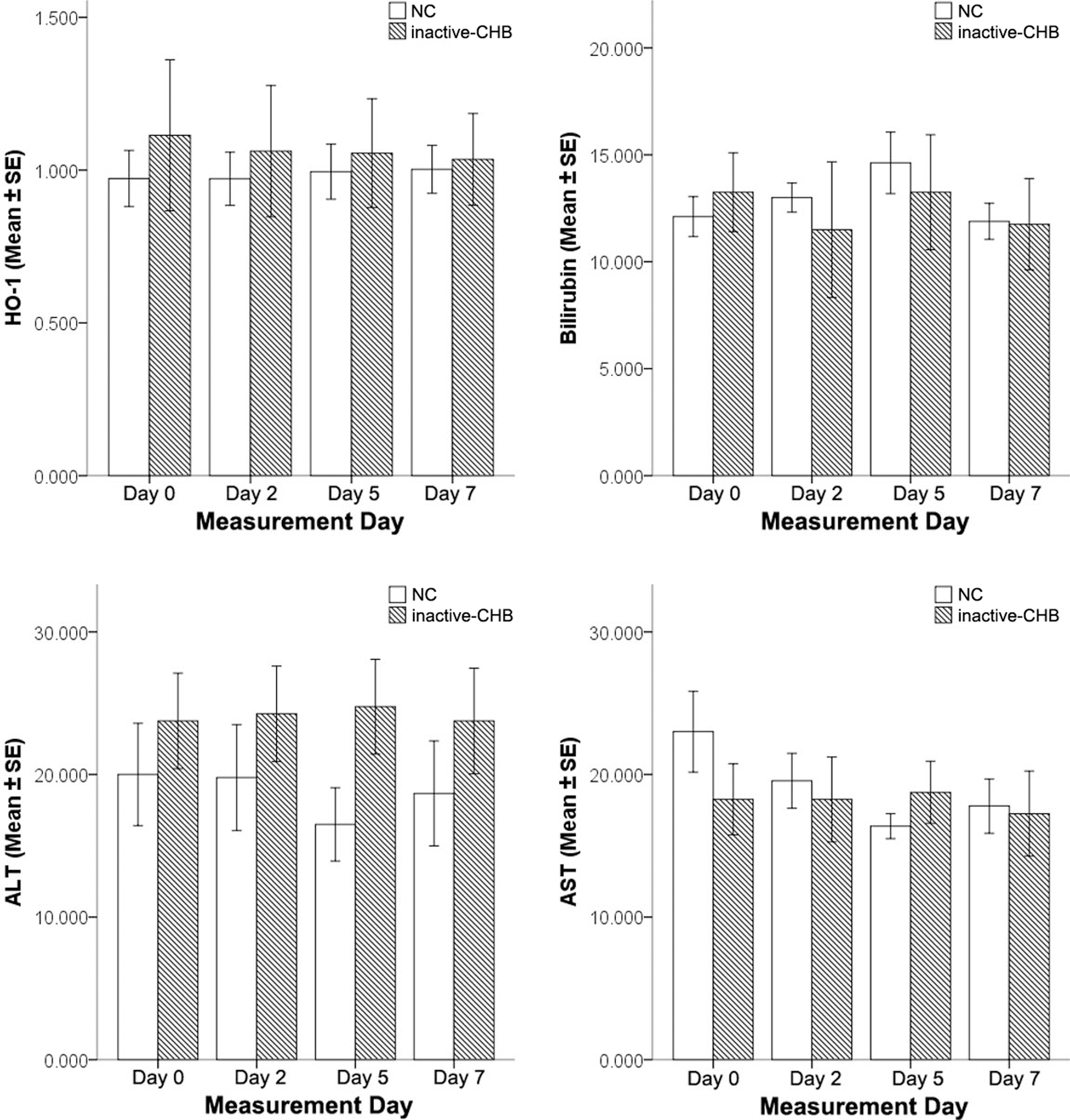
Changes of HO-1, total bilirubin, aspartate aminotransferase, and alanine aminotransferase levels in chronic inactive carriers (inactive-CHB) and noncarriers (NCs) of hepatitis B virus before and after Guasha. ALT, alanine aminotransferase; AST, aspartate aminotransferase; HO-1, heme oxygenase-1.
Discussion
Because all the investigated active and inactive chronic HBV carriers were asymptomatic and unaware of liver function from blood test results, our research protocol was effective in discounting the model that attributes the Guasha therapeutic efficacy to a placebo effect due to participant's expectation. Investigator bias during Guasha manipulation could also be discounted because of blinding of the blood test results. In contrast to the modulation of HO-1 and Th1/Th2 cytokines in our previously reported active-CHB case, 9 the null changes of HO-1, bilirubin, AST, ALT, interferon-γ, IL-4, IL-5, and IL-10 from days 0 to 7 in both inactive-CHB participants and NCs may be explained by the less impaired or intact cellular immune responses and insignificant or absent liver injury in our controls.
In the liver, Kupffer cells serve as macrophages for iron recycling in erythrophagotosis, and the proinflammatory free heme from hemoglobin breakdown upregulates HO-1 expression. 16 The cell-mediated immune response in HBV infection involves the activation of CD4 and CD8 T cells, 1 which play the most important role in the host defense against viruses by forming direct cytolysis or apoptosis or by cytokine secretion. 1 These populations generate cytokines and regulate each other to create a dynamic balance. The effect of the coordinated immune response is to eliminate HBV-infected cells. 1 The peripheral blood in patients at the immune inactive carrier stage and in healthy individuals contains more CD4 T cells than CD8 T cells, 17 which activates Kupffer cells in iron recycling. 18 In contrast, chronic active hepatitis is associated with an increased proportion of CD8 T cells relative to CD4 T cells. 17 In our inactive-CHB participants and NCs, it is possible that the Kupffer cells activated by high proportion of CD4 T cells can dissociate the slight increase of free heme generated by Guasha. Any increase in free heme by Guasha is expected to be insignificant. On the contrary, in active-CHB patients similar to the patient in our previous case study, the decreased proportion of CD4 T cells may not be able to activate Kupffer cells properly. Free heme produced during the Guasha process may trigger the upregulation of HO-1 expression, which in turn modulates the Th1/Th2 cytokine levels for the reduction of inflammation. The present results suggest that Guasha-induced HO-1 enhancement depends on the clinical stage of chronic hepatitis B.
Conclusion
In contrast to the active-CHB, Guasha did not induce any significant modulation of liver enzymes, HO-1, or cytokines in inactive-CHB participants and NCs. Guasha-induced hepatoprotective effect probably depends on the inflammatory event or clinical stage of chronic hepatitis B. Because both active and inactive carriers were completely unaware of their liver status at the time of receiving Guasha, our research protocol discounts the model that attributes the Guasha therapeutic efficacy to a placebo effect due to the patient's expectation. To our knowledge, this is the first report of the application of Guasha to inactive-CHB participants and NCs rather than an active-CHB patient. The long-term role of Guasha and the effect of repeated Guasha treatment on patients with chronic hepatitis B at different clinical stages remain to be investigated.
Footnotes
Acknowledgments
This research was supported by The Hong Kong Polytechnic University (5-ZD64). We thank the subjects for their participation in this study.
Disclosure Statement
No competing financial interests exist.