
Abstract
Objective:
To investigate the effectiveness of additional acupuncture in patients with chronic low back pain participating in an inpatient rehabilitation program.
Design:
Patients were randomly assigned to one of two groups (A and B), both receiving a standard rehabilitation program according to German guidelines. Patients in group A additionally underwent acupuncture twice weekly, conducted by two Chinese physicians with education in Traditional Chinese Medicine (TCM). At the beginning and end of the program, as well as at 3 months after, patients completed questionnaires about health-related quality of life (Short-Form 36 Health Survey [SF-36]), sociodemographic and clinical data, attitude towards TCM, pain, and adverse events.
Setting:
Inpatient rehabilitation clinic in Germany.
Patients:
Patients with chronic low back pain participating in an inpatient rehabilitation program.
Outcome measures:
Acceptance of acupuncture, health-related quality of life, and pain/symptoms.
Results:
One hundred and forty-three patients were analyzed: 74 in group A (intervention) and 69 in group B (controls); 67% were men and 33% were women, with a mean age of 50.7 years. Acceptance of TCM was excellent: 89% of the patients would want TCM to be integrated into standard inpatient rehabilitation, and 83% would even have paid for TCM if necessary. Responses to SF-36 questionnaires showed that group A reported significantly better physical functioning, general health, vitality, and emotional role than group B. Pain outcomes in group A were superior to those in group B. Specifically, pain with sitting/standing, pain upon carrying loads of 10 kg or more, and prickling in hands and feet were significantly diminished.
Conclusion:
Acupuncture was highly accepted and had positive effects in patients with chronic low back pain. These results show that acupuncture can be an effective, well-tolerated therapy with no major adverse events.
Introduction
I
Several clinical trials concerning acupuncture have been carried out so far, many of insufficient quality. 5 –7 Principles of evidence-based medicine dictate that trials should be prospective, controlled, randomized, and preferably double-blind. These criteria are definitively reasonable in studies of Western medicine but are not transferable to trials of TCM by implication. 5,7 In a meta-analysis of 51 acupuncture trials, Ezzo et al. 6 concluded that many trials are of low quality with respect to Western standards and that this low quality is associated with a positive effect of acupuncture. At the same time, trials of acupuncture with high quality according to evidence-based medicine criteria do not meet the requirements of TCM. 6 Therefore, some studies support the effectiveness of acupuncture and others question it. 6,8 –12
Clarifying the efficacy of acupuncture is particularly relevant because acupuncture has minimal adverse effects and is well tolerated. 13 –15 Therefore, the current study sought to investigate the effectiveness of adding acupuncture to standard inpatient rehabilitation in patients with chronic low back pain.
Methods
Study design
This prospective, randomized, controlled study was carried out between February 2008 and January 2009. Participants were recruited from an inpatient rehabilitation program. Inclusion criteria were chronic low back pain with duration of at least 6 months and age 25–75 years. Exclusion criteria included contraindications to acupuncture, such as anticoagulation with phenprocoumon or warfarin; coagulation disorders or thrombocytopenia (platelet count <150,000 cells/mm3); poor fluency in German language; insufficient adherence; recent surgical treatment; and herniated vertebral discs, either minor herniations of less than 6 months' duration or major herniations of any duration. Because of the variety of main outcomes assessed in this study, the results have to be interpreted as explorative. A total of 160 patients were randomly assigned to one of two treatment groups; each group had 80 patients on the basis of power analysis from a pilot study looking for changes of 15 percentage points in the dimensions of the Short-Form 36 (t-test; significance level, 5%; power, 80%). Randomization was done by the Institute for Epidemiology and Medical Biometry of the University of Ulm, Germany, by using a balanced block randomization.
The study was in accordance with principles of the Declaration of Helsinki and was approved by the ethics committee of Georg-August University, Göttingen, Germany. All participants gave written informed consent.
Treatment
Patients were randomly assigned to the intervention group (group A) or control group (group B). All patients participated in a standardized 21-day inpatient rehabilitation program according to current German guidelines. Patients in group A additionally received acupuncture twice weekly on a fixed schedule. Acupuncture was done by two Chinese physicians, who had completed education in TCM in China and had practiced in Germany for several years. Diagnosis and treatment accorded with TCM principles, with a focus on medical history, tongue, and pulse diagnosis. Fixed positions of the needles were not mandated so that the therapists were not restricted in their treatment options. Each patient was treated individually according to the opinion of the TCM physician. Acupuncture was done with two different types of sterile disposable needles: VQ-3210 (0.25×25 mm) and VQ-3205 (0.25×13 mm). The duration of each session varied between 30 and 40 minutes. Tuina massage and a magnet lamp (TDP-lamp CQ-35, Chongqing Xinfeng Medical Instruments Co. Ltd., Chongqing, China) were additionally used at the discretion of the TCM physicians. Patients were advised to rest for 30 minutes after acupuncture.
Outcomes
At the beginning (t0) and end (t1) of the rehabilitation program, as well as 3 months after rehabilitation (t2), patients completed questionnaires about health-related quality of life (SF-36), 16 –18 sociodemographic and clinical data, attitude towards TCM (including acupuncture), pain (quality, intensity, duration), and adverse events.
The SF-36 is a validated questionnaire with 36 items that assess physical functioning, physical role, bodily pain, general health, vitality, social functioning, emotional role, and mental health. Results were scored between 0 and 100, with higher scores indicating better health. All items on the SF-36 were equally regarded as main outcomes.
Sociodemographic and clinical data, attitude towards TCM, quality, intensity and duration of pain, and adverse events were determined by using questionnaires developed by the research team. The questionnaire on pain was completed by the patients themselves to describe how often in the previous week they had back pain while sitting/standing, walking, or bearing moderate (≤5 kg) or heavy (≥10 kg) weight. Additionally, patients were asked to report the frequency of prickling in hands or feet as “never,” “sometimes,” “every day,” “several times a day,” or “constantly.” Patients also reported the duration of painful episodes.
Statistical analysis
Statistical analyses were descriptive, using means with standard deviation and frequency counts. To compare the different groups, the chi-square test and the t-test were used, with an α value of 5%. Because of the multiplicity of outcome variables (e.g., dimensions of SF-36), this analysis must be interpreted as an explorative study; no adjustment for multiple testing was done. Linear regression was done to test for possible correlations between different characteristics. Analysis was carried out using the statistical software SAS, version 9.1 (SAS Institute, Cary, North Carolina).
Results
Study cohort
Between February 2008 and January 2009, 160 patients with chronic low back pain who attended the study clinic for inpatient rehabilitation were invited to participate in the study. These patients were randomly assigned to the two groups. Four patients (2.5%) were excluded: Three had insufficient proficiency in the German language, and one had no back pain. Thirteen patients (8.1%) discontinued the study early: Seven wished to participate in other rehabilitation programs, two had severe comorbid illness, one had no back pain, one had insufficient adherence, one experienced pain during acupuncture, and one revoked consent to participate. The distribution of patients who were excluded or who withdrew was six patients in group A and 11 patients in group B (Fig. 1).
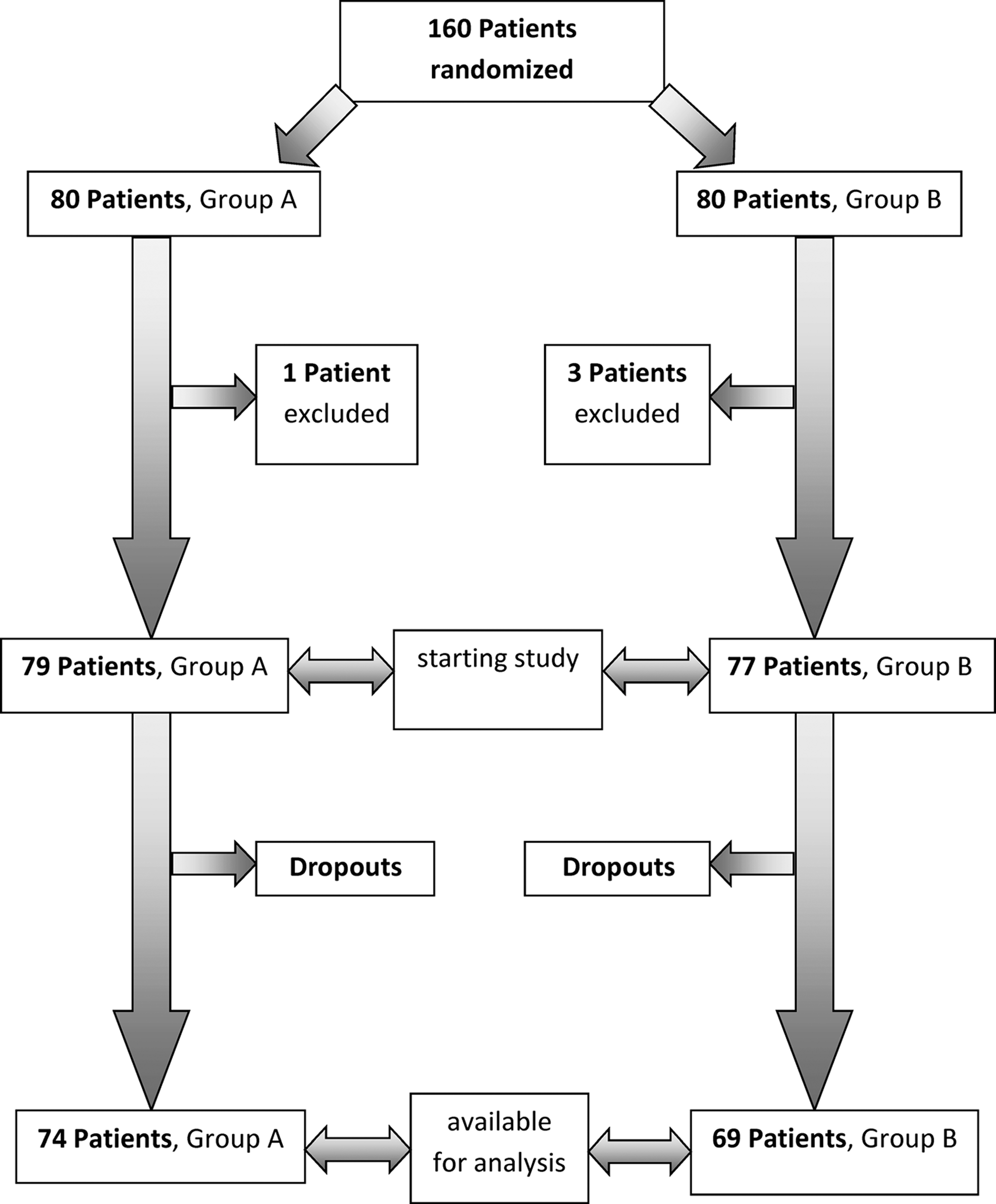
Randomization of the patients.
The remaining 143 patients were allocated according to the original randomization process: 74 (51.8%) in group A (intervention group) and 69 (48.3%) in group B (control group). Ninety-six of the participants (67.1%) were men and 47 (32.9%) women, and the mean age±standard deviation was 50.7±7.7 years (range, 31–73 years). Table 1 shows demographic data for the total population and for groups A and B. Baseline values did not significantly differ between the two groups.
Values expressed with a plus/minus sign are the mean±standard deviation.
SF-36, Short-Form 36 Health Survey.
Acceptance of TCM
According to a questionnaire developed by the authors, acceptance of complementary medicine was excellent. One hundred and twenty-seven patients (88.8%) wanted TCM to be integrated as standard in inpatient rehabilitation programs, only 1 patient (0.7%) explicitly did not, and 15 patients (10.5%) were undecided. One hundred and nineteen patients (83.2%) said they would be willing to pay for TCM if necessary, 23 (16.1%) would not, and 1 (0.7%) was undecided.
SF-36 questionnaire
SF-36 results for the total study population showed that patients scored worse than the average healthy German general population in the age groups 41–50 years and 51–60 years, 16 which correlate with the mean age of the study population (Table 2).
Values are the mean±standard deviation.
At the beginning of the rehabilitation program (t0), groups A and B did not differ significantly on the SF-36 (Table 1). On the scale of physical functioning, both groups improved from t0 to t1, with no significant difference between groups. However, with regard to the interval t0 to t2, groups A and B differed significantly, with superior results in group A. Physical role scores favored group A, with no significant difference between groups; for bodily pain, both groups showed a nonsignificant improvement from t0 to t1. With respect to vitality, the two groups differed significantly from t0 to t2, favoring group A. General health also differed significantly in favor of group A from t0 to t1 (improvement) and from t0 to t2 (deterioration). Finally, emotional role showed a nonsignificant improvement in both groups from t0 to t1 and a significant deterioration from t0 to t2; deterioration was worse in group B. Social functioning and mental health did not significantly differ between groups (Table 3).
p<0.05 considered to represent significant difference; no correction for multiple comparison. p-Values calculated with t-test.
t0, beginning of study; t1, end of study; t2, 3 months after end of study.
Pain questionnaire
In the total population, mean duration of back pain was 11.34±8.47 years (range, 0.5–40 years). At t0, most patients had pain at least sometimes; only a few patients never experienced pain, and a sizable portion had pain constantly. About 9% (n=13) of the patients avoided bearing loads of 10 kg or more because of pain, but only 1 patient (0.7%) avoided bearing loads less than 5 kg. Most patients experienced paresthesias in hands or feet at least sometimes. For these variables, no relevant differences were noted between groups A and B (Table 4).
Values did not significantly differ between groups.
Table 5 shows the changes in responses to the pain questionnaire by group. The development of pain upon sitting or standing (t0 to t2) showed significantly more favorable results in group A (improvement in 64.1% versus 36.9% of patients; p=0.009). For pain upon carrying loads of 5 kg or less, no significant difference was noted between groups (p=0.098), but group A showed better results. With regard to loads of 10 kg or greater, there was a significant difference between groups for t0 to t2 (p=0.02), with more favorable outcomes in group A. No significant difference was seen concerning pain when walking, but with regard to paresthesias, group A showed more favorable results (t0 to t1, p=0.01; t0 to t2, p=0.04).
p<0.05 considered to represent significant difference; no correction for multiple comparison.
ND, not determined; t0, beginning of study; t1, end of study; t2, 3 months after end of study.
No major adverse events occurred. Minor adverse effects were nausea in 2.7% of patients, dizziness in 13.5%, urgency in 20.3%, and pain at puncture site in 36.5%.
Discussion
In recent years, acupuncture and TCM, respectively, have gained more and more attention in the Western world, and several clinical trials have been conducted. However, there is no consensus about the clinical outcomes of acupuncture. 6,8,9 –12
Many acupuncture trials, however, do not sufficiently consider traditional diagnostics and treatment modalities in TCM, especially high-quality studies conducted according to evidence-based medicine standards. 5,6,19 In several trials on chronic back pain, the exact locations of the needles were determined in advance, whereas in TCM the positions and numbers of the needles vary from patient to patient, according to traditional diagnosis. 5,7 To use acupuncture appropriately, not just individual diagnosis and positions of needles are important; qualifications and experience of the acupuncturist are also relevant. 5,20,21 In the current study, acupuncture was conducted by experienced TCM physicians who chose unique needle positions for each patient. Therefore, needle location is not reported here, as partially postulated in the literature. 22,23
Some trials of acupuncture recommend 10 sessions, 22,24 whereas another favors 4 sessions at least. 25 Thus, there is no absolute consensus about the optimal number of treatments. Patients in the present study received a mean of only 6.3 sessions. As a result, extending acupuncture for additional sessions after rehabilitation might have led to an even greater effect.
To assess outcomes, the SF-36 health survey and investigator-developed questionnaires were used. The SF-36 questionnaire has been validated in several studies with regard to reliability, sensitivity, and internal consistency. 26 –31 The investigator-developed questionnaires have not been validated and thus must be handled in another way.
Acupuncture showed positive effects on pain and paresthesias. Comparing both groups, group A showed better results in almost all items, with some measures reaching statistical significance. In group A, pain upon sitting/standing, pain upon carrying loads of 10 kg or greater, and paresthesias in hands and feet improved in significantly more patients than in group B between t0 and t2. Considering that both groups had similar pain at baseline and both groups received the same multimodal therapy besides acupuncture, these results suggest that this effect is attributable to acupuncture, which is especially remarkable because the multimodal therapy itself is shown to be highly effective. 32,33
In the literature, acupuncture is reported to reduce prickling in carpal tunnel syndrome and paresthesias in diabetic neuropathy. 34 –37 Although back pain and carpal tunnel are distinct conditions, the pathophysiology of prickling in both conditions may be similar. There appears to be nothing in the literature about the effect of acupuncture on paresthesias in back pain; thus, it would be interesting to conduct further clinical trials in this area.
Concerning the SF-36, the items on physical functioning, general health, vitality, and emotional role showed significantly better results in group A at t2 (which also applied for general health at t1). In the other measures, which did not reach statistical significance, group A showed consistently better results as well.
Patients received only a mean of six acupuncture sessions; the findings seen with just these six sessions suggest that maintenance acupuncture after rehabilitation would be reasonable. Nevertheless, for some items results deteriorated from t0 to t2 in both groups. This is a known effect discussed in several studies. 38 –40 Because the results of the current study suggest that acupuncture has a positive effect, this deterioration in some patients is not accounted for any further. Other studies dealing not only with back pain but also with disorders of the cervical spine, gonarthrosis, headache, menopausal disorders, and nausea in chemotherapy confirm the positive effect of acupuncture. 8 –10,41 –44
Several trials have investigated the physiologic mechanisms of acupuncture. It is hypothesized that analgesia results from liberation of opioid mediators and endorphins that bind to μ-, δ- and κ-receptors. Other mediators, such as serotonin, nitric oxide, cholecystokinin, catecholamines, and glutamate, seem to play a role as well. 45 –48 In this context, differences in effects in several genetic expressions of cholecystokinin receptors were postulated and investigated. 49 Individual differences in sensitivity in the activation of afferent nerve fibers (Aβ, Aδ, and C) is also assumed. 45 Zhao reports that signals over the ventrolateral pathway of the spinal cord are conducted to different nuclei of the brain, where they activate inhibitory parts of the central nervous system, leading to analgesia. In addition to biological processes set in motion by acupuncture, psychological effects are discussed in the context with the properties of acupuncture.
A main goal of the current study was to assess the acceptance of TCM among patients, which proved to be excellent. The patients were mainly male (67%), with relatively low education and minor occupational qualifications. This differs from the profile of patients who have typically been described as accepting of TCM. In the literature, patients using alternative medical therapies are typically described as female, with a higher level of education and higher income. 50 –53 The current results suggest a wider acceptance of acupuncture. This is mirrored by the patients' high willingness to pay for TCM. Although the study patients do not derive from a prosperous social class, most of them would be willing to pay an additional fee to obtain acupuncture during rehabilitation.
This study has several limitations. First, several patients withdrew from the study, but an intention-to-treat analysis was not performed. There is a small possibility of a selection bias because the dropout rate was higher in group B than group A. Second, several main outcomes were measured simultaneously, so the results have to be interpreted as explorative and as showing tendencies, without giving statistical proof. The power and sample size were insufficient for adjustment for multiple testing, but interpretable indications and tendencies for some effects can be shown. The results apply to a population similar to the study patients (see inclusion and exclusion criteria) in a similar clinical setting but are not generalizable.
In conclusion, acupuncture was highly accepted by the study patients and had positive effects both during and 3 months after rehabilitation. The trial showed once more that acupuncture can be effective, well tolerated, and free of major adverse events. Acupuncture therefore should be integrated regularly into rehabilitation programs, a feasible prospect according to our experience.
Footnotes
Disclosure Statement
No competing financial interests exist.