
Abstract
Objectives:
To evaluate the effectiveness and safety of Chinese herbal medicine (CHM) as an adjunctive treatment for patients with dilated cardiomyopathy (DCM) and heart failure.
Design:
Studies on biomedical treatment plus CHM versus biomedical treatment alone in treating patients with DCM and heart failure were retrieved from PubMed and other major databases (1980–2011). Meta-analysis was performed on the overall effects on effective rate, left ventricular ejection fraction, left ventricular diastolic end diameter, and other outcome measures.
Results:
Twenty-seven studies with 1887 patients were included. Compared with biomedical treatment alone, biomedical treatment plus CHM showed significant improvement in effective rate (relative risk, 1.26; 95% confidence interval [CI], 1.19–1.34), left ventricular ejection fraction (%) (mean difference, 5.88; 95% CI, 3.92–7.85), left ventricular diastolic end diameter (mm) (mean difference, −2.78; 95% CI, −5.15 to −0.42), and other outcome measures. Most adverse events observed in the studies were not severe and resolved without special treatment.
Conclusions:
This meta-analysis indicated that biomedical treatment plus CHM is more effective than biomedical treatment alone in treating patients with DCM and heart failure. However, further studies with long-term follow-up, systemic adverse events evaluation, and other ethnic groups are still required to verify the efficacy and safety of CHM as an adjunctive treatment in all patients with DCM and heart failure.
Introduction
Medical therapy remains the mainstay in patients with DCM and heart failure. With the purpose of improving clinical status and slowing the evolution of ventricular remodeling, angiotensin-converting enzyme inhibitors (ACEIs) and β-blockers with or without diuretics continue to be standard treatment. 8 The most appreciable distinction between China and western countries in DCM therapy is the use of Chinese herbal medicine (CHM) as an adjunctive treatment. However, few English-language studies have addressed the effectiveness and safety of commonly used CHM, despite the wide acceptance of this therapy in China for many years. This study was performed because it is still uncertain whether there is robust evidence on the clinical effects of CHM and whether CHM can be recommended for routine DCM therapy.
This study analyzed the existing evidence on CHM as an adjunctive treatment for patients with DCM and heart failure in order to verify whether CHM can provide further benefit when given in addition to biomedical treatment.
Methods
Information Sources
To identify clinical trial reports published between 1980 and 2011, major databases were searched: PubMed, Cochrane Library, Elsevier, EMBASE, SpringerLink, Blackwell (Interscience), Cambridge Journals Online, OVID, China National Knowledge Infrastructure (CNKI), WanFang Data (WF), China Master Theses Full-text Database (CMFD), China Doctoral Dissertations Full-text Database (CDFD), Chinese Electronic Periodical Services, and Chinese Dissertation Database. The last retrieval in all databases was performed on July 1, 2011.
Keywords
The following keywords were used in search strategies in all fields, entered in English or Chinese depending on the working language of databases: “dilated cardiomyopathy,” “kuozhangxingxinjibing” (Chinese pinyin of “dilated cardiomyopathy”), “Chinese herbal medicine,” and “zhongyao” (Chinese pinyin of “Chinese herbal medicine”). The following search strategy and keywords were used in PubMed and other English-language databases: 1. Dilated cardiomyopathy 2. Chinese herbal medicine 3. Traditional Chinese medicine 4. Chinese drugs 5. 1 and 2 6. 1 and 3 7. 1 and 4
For searching CNKI and other Chinese databases, the following search strategy and keywords were used: 1. kuozhangxingxinjibing [dilated cardiomyopathy] 2. zhongyao [Chinese herbal medicine] 3. zhongyi [traditional Chinese medicine] 4. zhongxiyijiehe [integration of traditional Chinese medicine and biomedical] 5. 1 and 2 6. 1 and 3 7. 1 and 4
Selection Criteria
Eligible studies met the following inclusion criteria: (1) design of randomized controlled trial was explicitly described, (2) CHM was used only in the experimental group and biomedical treatment was used in both the experimental group and the control group, (3) in both groups, biomedical treatment contained one ACEI and one type of β-blocker with or without diuretics and cardiocinetics, (4) DCM and heart failure were diagnosed by the criteria consistent with the World Health Organization guidelines, 9 and (5) treatment duration lasted 4 weeks or more.
Studies were excluded if (1) diagnostic criteria for DCM were not specified, (2) patients had hypotension (systolic blood pressure <90 mmHg or diastolic blood pressure <50 mmHg) or shock, (3) patients had decompensated heart failure, (4) patients had other heart diseases (coronary heart disease, valvular heart disease, hypertensive heart disease, or congenital heart disease) or systemic disorders, or (5) the data in the methods or results section were unreliable or unavailable.
Outcome Measures
Primary outcome measures were the effective rate (ER), left ventricular ejection fraction (LVEF), and left ventricular diastolic end diameter (LVDED). Secondary outcome measures were mortality, 6-minute walking test (6MWT), and other outcomes for Doppler echocardiography.
Study Selection
Four authors independently retrieved the titles and abstracts of studies according to the preceding eligibility criteria. Disagreements between the investigators in the results were resolved by consensus. Two investigators independently selected randomized controlled trials that met the selection criteria. Full texts were retrieved and further assessed in the same method as per the selection criteria. Repeated publications of studies were removed after discovery by juxtaposing author names, sample sizes, and outcomes. The process of selecting relevant studies retrieved from the databases is shown in Figure 1.
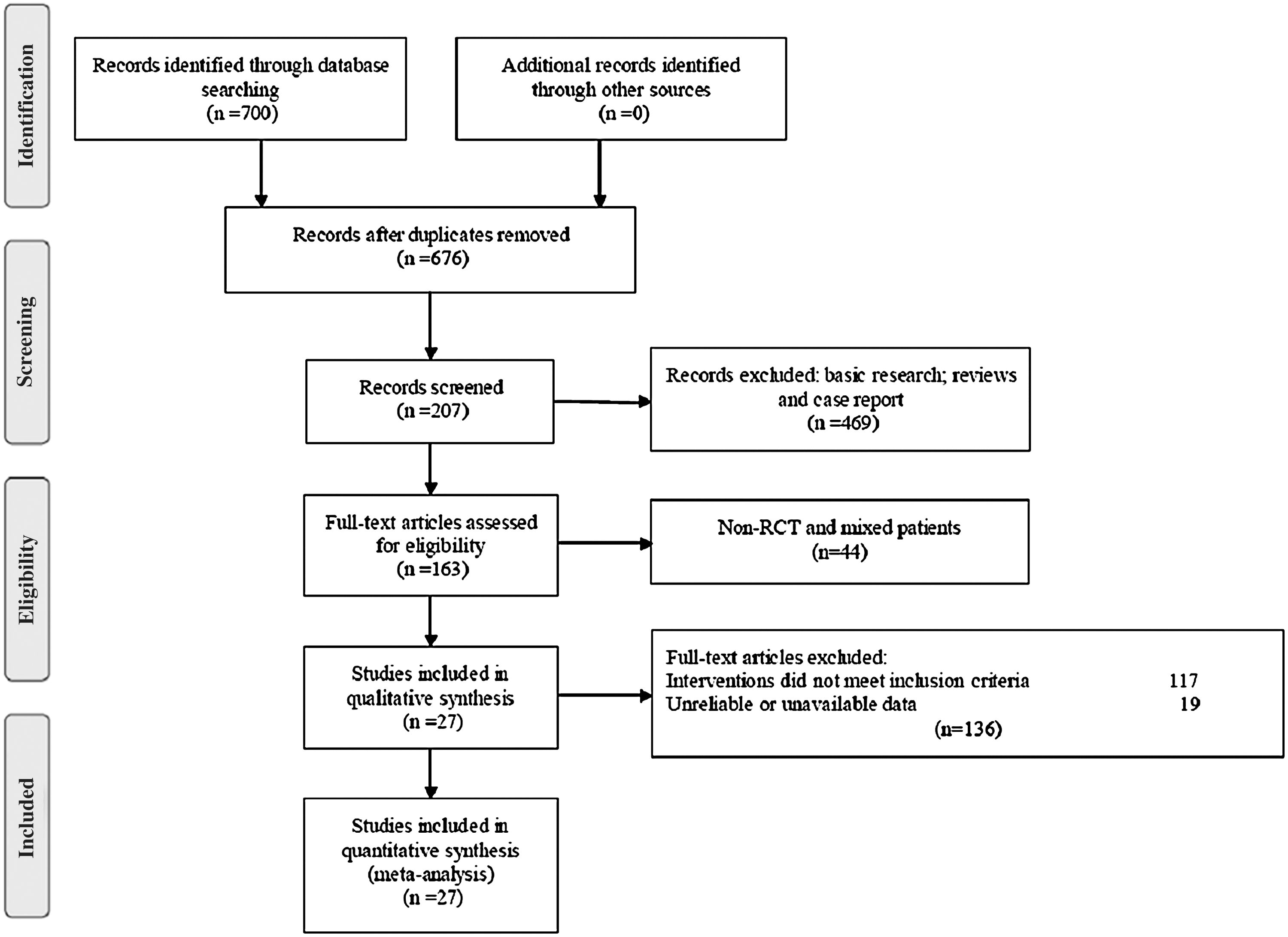
Flow diagram of study selection. RCT, randomized controlled trial.
Data Extraction
One investigator extracted data from the included studies and entered them into an electronic spreadsheet (Microsoft Excel, Microsoft, Redmond, Washington), and another investigator double-checked the extracted data. Data comprised the characteristics of patients, methods, interventions, outcome measures, and results. Missing data were obtained from the original authors whenever possible. Extracted data were then transferred to Review Manager 5.1 (Cochrane IMS, Copenhagen, Denmark) for this meta-analysis.
Subgroup Analysis
Subgroup analysis was conducted to assess the overall effects in subgroups based on characteristics of studies, including treatment duration and sample sizes.
Statistical Analysis
Meta-analysis was conducted using Review Manager 5.1 software. Dichotomous data were presented as relative risk (RR) with 95% confidence intervals (CIs). Continuous data were presented as mean difference with 95% CIs. Forest plots were generated to visualize and evaluate the efficacy results of meta-analysis. I2 and χ2 were determined by Review Manager 5.1 as measures of heterogeneity. Publication bias was analyzed by funnel plots. All p values less than 0.05 were considered to represent statistically significant findings. The Cochrane Collaboration's tool was used for assessing risk of bias.
Results
Study Selection
Seven hundred potentially relevant studies were identified; 537 studies were excluded by the screening of titles and abstracts. Full texts from 163 studies were retrieved and carefully assessed. One hundred and seventeen studies were excluded because the intervention did not meet the inclusion criteria, and 19 were excluded for unreliable or unavailable data.
Study Characteristics
A total of 27 included studies were published in Chinese from 2001 to 2011, 10 –36 and 6 of these had an English abstract. 11,13,20,25,30,31 These studies involved 1887 patients with DCM and heart failure age 7–86 years. All included patients were in the compensation course of heart failure. Fourteen studies reported the course of disease (range, 3 months–26 years). The treatment duration was a minimum of 4 weeks and a maximum of 1 year. Table 1 shows the baseline characteristics of these studies. Table 2 provides the names and ingredients of CHMs.
Blackbody herbal ingredients were the most frequently used in Chinese herbal medicine of studies included.
The studies compared biomedical treatment plus CHM versus biomedical treatment alone. Biomedical treatment followed the guidelines for DCM and heart failure, 8,9 including one ACEI and one type of β-blocker, with or without diuretics and cardiocinetics. The ACEIs used in these studies included captopril, benazepril, enalapril, perindopril, and fosinopril, which were administrated by half-value to double dose. The use of β-blockers (metoprolol, bisoprolol, and atenolol) began with a low dose in all included studies, and 8 studies used them up to the maximum tolerated dose.
Primary Outcomes
ER
The ER, as the most commonly used measure to evaluate drug efficacy, was reported by 18 studies 10,12 –15,17 –19,21,25,27,28,30 –33,35,36 involving 1373 patients. In these studies, responders were defined as showing improvement in least one New York Heart Association class. ER was calculated as the proportion of responders in the experimental group or the control group. The meta-analysis showed that biomedical treatment plus CHM had a better ER than did biomedical treatment alone (RR, 1.26; 95% CI, 1.19–1.34; Z=7.78; p<0.00001), with no significant heterogeneity (I2 =0%, χ2=13.61, df=17, p=0.69). None of these studies showed that the experimental group had a lower ER than the control group (Fig. 2).

The Forest plot of effective rate. Error bars indicate 95% confidence intervals (CIs). Diamonds designate overall effect and squares, the effect for each individual study; both represent the width of the CI. CHM, Chinese herbal medicine; M-H, Mantel-Haenszel.
LVEF
LVEF is frequently used to assess heart failure and evaluate drug efficacy. The meta-analysis for 25 studies, 10 –26,28 –32,34 –36 including 1803 patients, showed that biomedical treatment plus CHM was associated with a higher LVEF than biomedical treatment alone (mean difference, 5.88; 95% CI, 3.92–7.85; Z=5.87; p<0.00001), with significant heterogeneity (I2 =92%, χ2=284.92, df=24, p<0.00001). Only 2 of the 27 studies showed that the experimental group had a lower LVEF than the control group 23,25 (Fig. 3).
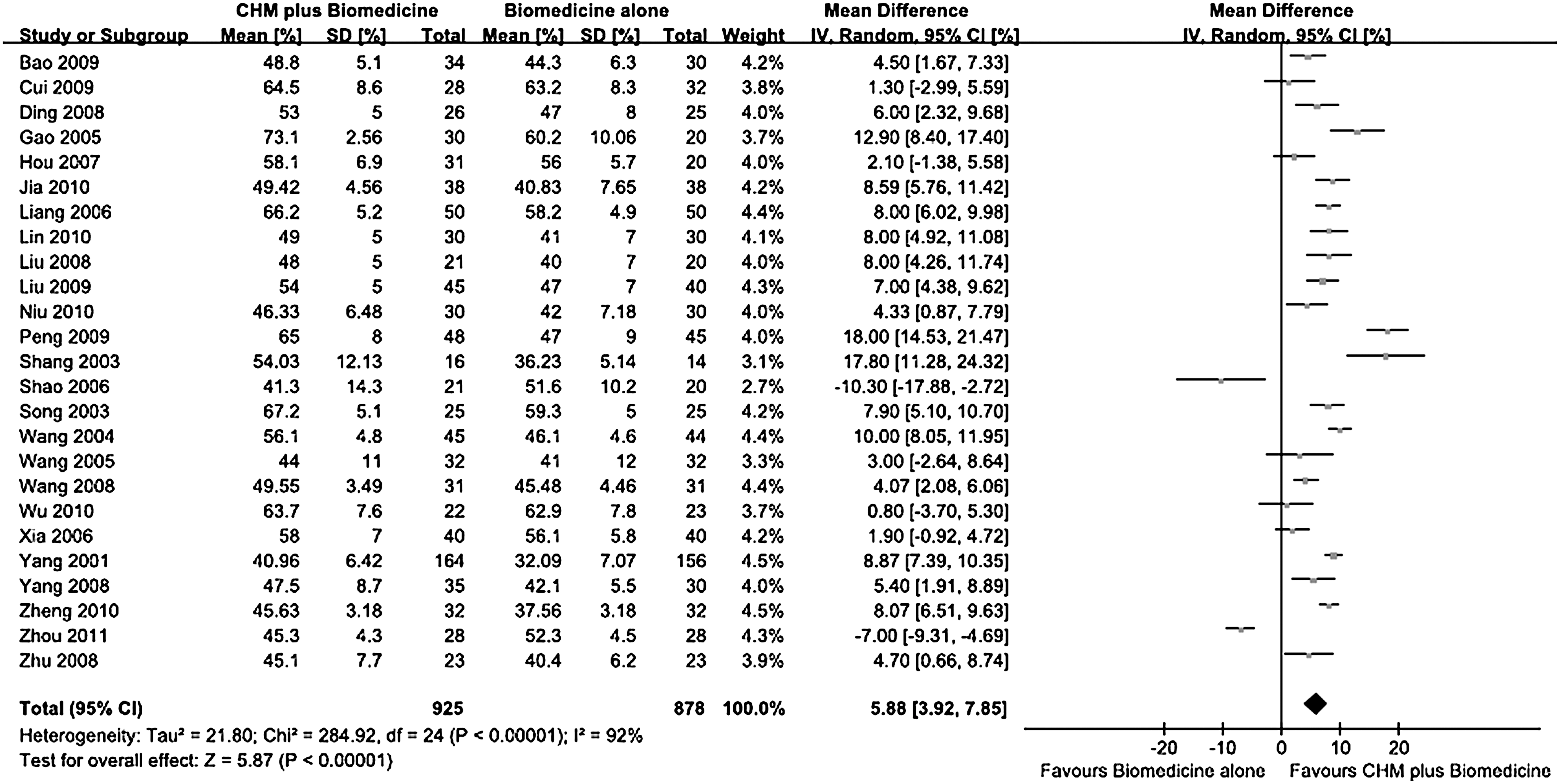
The Forest plot of left ventricular ejection fraction (%). Error bars indicate 95% CIs. Diamonds designate overall effect and squares, the effect for each individual study; both represent the width of the CI. SD, standard deviation; IV, inverse variance.
LVDED
LVDED is an important outcome measure in diagnostic and prognostic assessment for DCM. The meta-analysis of 8 studies, 10,15,17,21,23,26,28,35 including 516 patients, showed that biomedical treatment plus CHM was associated with a shorter LVDED than biomedical treatment alone (mean difference, −2.78; 95% CI, −5.15 to −0.42; Z=3.45; p=0.02) with a significant heterogeneity (I2 =87%, χ2=55.75, df=7, p<0.00001). Only 1 study showed that experimental group had a longer LVDED than the control group 23 (Fig. 4).
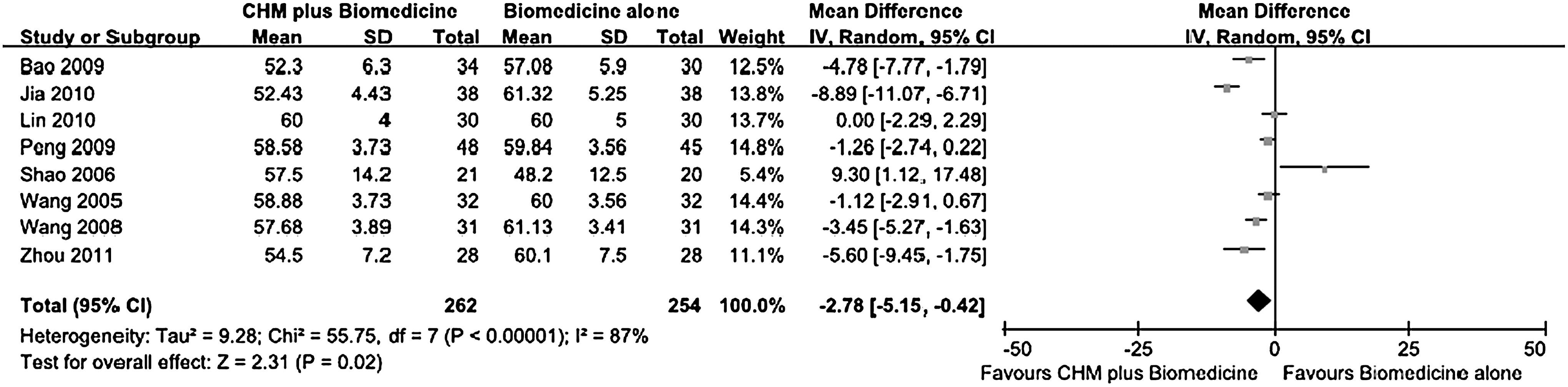
The Forest plot of left ventricular diastolic end diameter (mm). Error bars indicate 95% CIs. Diamonds designate overall effect and squares, the effect for each individual study; both represent the width of the CI.
Secondary Outcomes
Mortality
Only 6 studies of total 681 patients reported mortality. 11,16,24,25,28,31 Furthermore, these studies were not designed to evaluate mortality as a primary outcome. The result of meta-analysis showed a significant decrease in mortality in the experimental group compared with the control group (RR, 0.53; 95% CI, 0.35–0.82).
6MWT
The meta-analysis of 8 studies, 11,15 –18,24,25,29 including 496 patients, showed a significant improvement in 6MWT in the experimental group compared with the control group (mean difference, 71.04; 95% CI, 32.12–109.96). It seemed that the experimental group had better exercise tolerance.
Other Outcomes for Doppler Echocardiography
Some studies provided data for other outcomes in Doppler echocardiography. The experimental group showed a significant increase in left ventricular shortening fraction (mean difference, 5.79; 95% CI, 2.94–8.65; 3 trials 20,21,25 including 242 patients), stroke volume (mean difference, 8.88; 95% CI, 5.25–12.51; 10 trials 12 –14,16,19,20,22,24,25,30 including 646 patients), cardiac output (mean difference, 0.86; 95% CI, 0.46–1.26; 11 trials 12 –14,16,19,20,22,24 –26,30 including 710 patients) and cardiac index (mean difference, 0.42; 95% CI, 0.16–0.68; 7 trials 12 –14,19,20,22,30 including 407 patients).
Subgroup Analysis
We performed subgroup analysis on treatment duration and sample sizes to investigate specific factors affecting the overall effect in the studies. Overall mean difference in LVEF did not significantly differ among the subgroups with differing treatment durations and sample sizes (Table 3). The agreement among the subgroup analysis results indicated that the efficacy among all included studies was consistently stable.
CI, confidence interval.
Risk of Bias Assessment
Included studies were of poor methodologic quality. All included studies included indicated randomization; 4 of reported that the random sequence was generated by a random-digits table, 11,28,29,31 and 4 by the patient treatment order. 14,22,27,30 The remaining 19 studies did not describe the methods of randomization. Only 1 of the studies mentioned that it was single-blind, 20 and 2 used a placebo control. 20,29 Only 6 studies reported the number of patients lost to follow-up, 11,16,24,25,28,31 and 4 had used intention-to-treat analyses. 11,24,25,31 No study suggested selective outcome reporting. Publication biases for two major outcomes, ER and LVEF, were assessed by funnel plots (Fig. 5 and Fig. 6). Both figures were slightly asymmetrical, indicating that potential publication bias might influence the results of this meta-analysis.
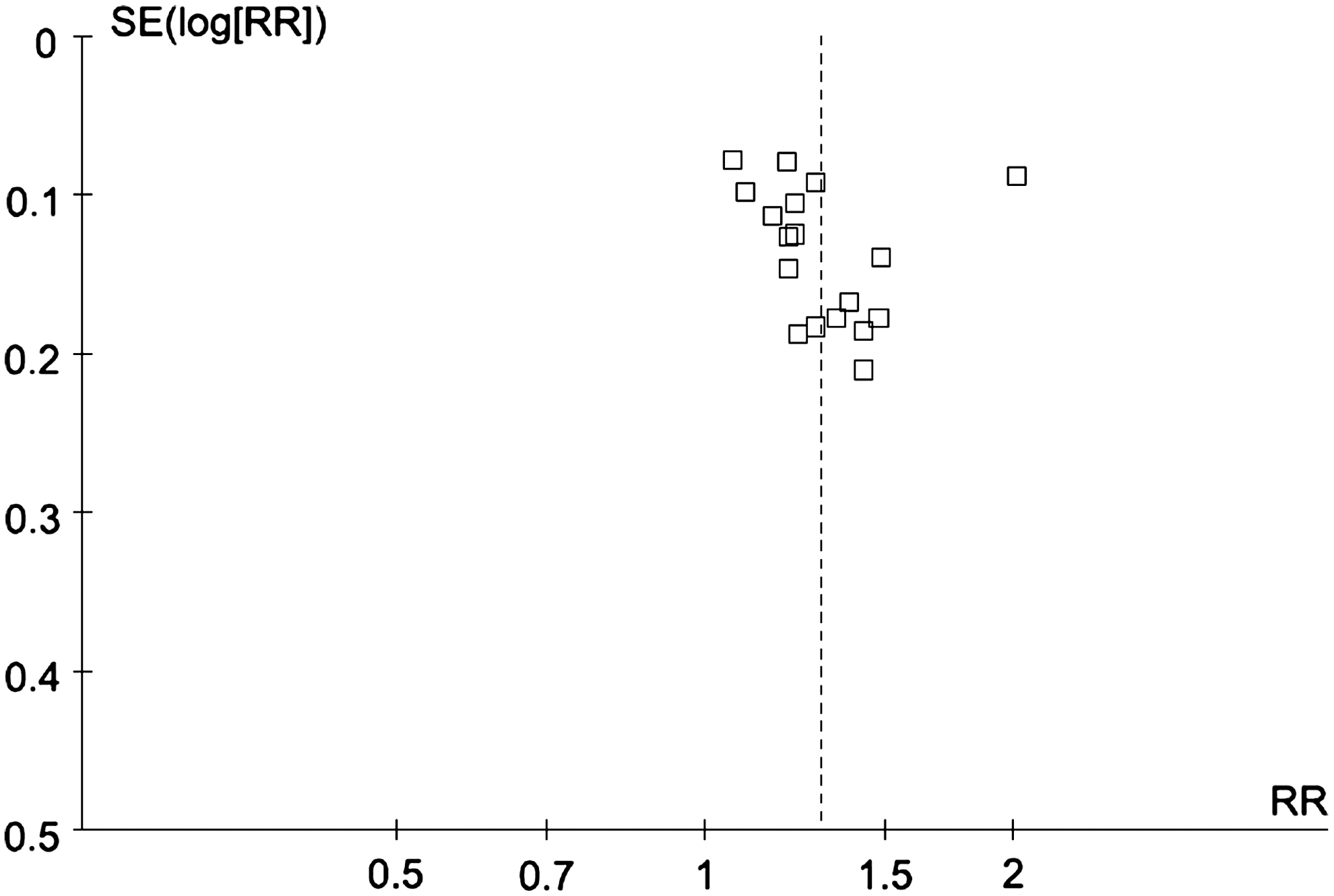
Funnel plots of included studies with effective rate data. RR, relative risk; SE, standard error.

Funnel plots of included studies with left ventricular ejection fraction data. MD, mean difference.
Adverse Events
Among 27 included studies, 17 did not report adverse events and 5 reported no adverse events. Only 5 studies reported adverse events, including epigastric discomfort, dizziness, dry mouth, and nausea. 11,14,17,18,29 Most of the adverse events were not severe, and they resolved without special treatment.
Discussion
To our knowledge, this article is the first comprehensive investigation of the existing evidence on CHM as an adjunctive treatment for patients with DCM and heart failure. Compared with biomedical treatment alone, biomedical treatment plus CHM showed significant improvement in symptoms, exercise tolerance, mortality, and outcome measures for Doppler echocardiography. In a word, biomedical treatment plus CHM improved patients' quality of life during observation.
Biomedical treatment has made tremendous progress and remains the dominating treatment for patients with DCM and heart failure worldwide. ACEIs and β-blockers as biomedical treatments for patients with DCM and heart failure were generally accepted. In this meta-analysis, CHM can provide additional benefit with ACEIs and β-blockers. These results showed more diminished left ventricular cavity in the experimental group due to shorter LVDED compared with the control group. Both ACEIs and β-blockers can slow the evolution of ventricular remodeling and reduce the risk for death and the combined risk for death or hospitalization. 37 –40 The ability of CHM to inhibit ventricular remodeling has been reported in some experiments in animals with heart failure. The mechanism of this function may be apoptosis inhibition, regulatory effect of the neuroendocrine system, or regulation of protein expression, 41 –44 and further research is needed to determine the exact mechanism.
In Traditional Chinese Medicine, qi deficiency, yin deficiency, and yang deficiency, as well as water retention, blood stasis, and turbid phlegm, are principal syndrome factors for patients with DCM and heart failure. Thus, the main CHMs for clinical application include the following: for invigorating qi, Astragalus membranaceus and ginseng; for nourishing yin, Ophiopogon japonicus; for warming yang, Radix aconiti lateralis preparata and Ramulus cinnamomi; for draining water, Poria cocos; for activating blood, Salvia miltiorrhiza; and for dispelling phlegm, Semen Armeniacae amarum. 45,46 A. membranaceus, ginseng, O. japonicas, R. aconiti lateralis preparata, R. cinnamomi, P. cocos, and S. miltiorrhiza were also the most frequently used CHMs in the 27 studies included.
The results of subgroup analysis showed that biomedical treatment plus CHM was associated with a higher LVEF than biomedical treatment alone for different treatment durations and sample sizes. Moreover, treatment duration of 13–26 weeks seemed to provide the best response.
Limitations of this study include the following. More positive studies than negative studies are likely to be published. Funnel plots of ER and LVEF seemed slightly asymmetrical, indicating that publication bias might influence the results of this study. Although this study evaluated the effect of treatment on CHM, future studies should assess not only the outcomes of symptoms and hemodynamic changes in the short term but also mortality and quality of life in long-term follow-up. In this meta-analysis, only 6 of the 27 included studies reported mortality. None of these studies reported quality of life in long-term follow-up. The studies reported no systemic adverse events; thus, this meta-analysis cannot adequately evaluate the safety of CHM for patients with DCM and heart failure. In addition, all studies included in this meta-analysis were conducted in China with Chinese patients. The results cannot be generalized to other ethnic groups without verification.
Conclusions
This meta-analysis of 27 studies indicated that biomedical treatment plus CHM is more effective than biomedical treatment alone in treating patients with DCM and heart failure. However, further studies that include long-term follow-up, evaluation of systemic adverse events, and other ethnic groups are still required to verify the efficacy and safety of CHM as an adjunctive treatment for all patients with DCM and heart failure.
Footnotes
Acknowledgments
The authors thank Drs. Feng Wei and Xiaozhen Zhuo for statistical input; Drs. Yuan Du and Tingzhong Wang for contacting authors and manufacturers for further information; Dr. Qun Lu and Bingxue Song for responding to requests for information; and the anonymous reviewers for their comments, which proved very helpful in the revision process. Special thanks to Professor Yingchao Li for helping with manuscript preparation and submission. This work was supported by the National Natural Science Foundation of China, No. 30830051.
Disclosure Statement
No competing financial interests exist.