
Abstract
Objective:
To evaluate the effect of acupuncture on hot flushes and other menopause-related symptoms used in an integrated system, including such therapeutic techniques as diet therapy and Tuina self-massage.
Design:
Randomized trial.
Setting:
Outpatient center.
Participants:
One hundred women in spontaneous menopause with at least three episodes of hot flushes daily were randomly allocated to two treatment groups (50 per group): Women in group A were given diet, self-massage training, and treatment with acupuncture, and women in group B (the control group) were given the same diet and self-massage training, but treatment with acupuncture started 6 weeks after they were enrolled into the study.
Intervention:
Acupuncture treatments were scheduled twice weekly for 6 consecutive weeks.
Outcome measures:
Mean change in frequency and/or intensity in menopause-related symptoms were estimated by questionnaire after treatment at week 4.
Results:
Treatment with acupuncture significantly reduced the occurrence of hot flushes and sudden sweating (p<.001). Other symptoms (sleep disorders, tightness in the chest, irritability, bone pain, feeling depressed) significantly improved.
Conclusions:
Acupuncture in an integrated system that includes therapeutic techniques such as diet therapy and Tuina self-massage can be used to treat hot flushes and selected symptoms in postmenopausal women.
Introduction
S
These studies indicated an increased risk in cardiovascular events and breast cancer associated with HRT. This has led many doctors and patients to question whether the risk of HRT outweighs the benefits. Thus, the importance of alternatives to HRT, such as acupuncture, has become evident.
Acupuncture has fewer adverse effects than does pharmacologic therapy. 4 Treatment with Traditional Chinese Medicine (TCM) also has a positive influence on lifestyle because it is integrated with dietary information.
Acupuncture is used in Europe and the United States for the treatment of many menopausal symptoms. Clinical trials on the efficacy of acupuncture 5 –7 have shown controversial results. Some studies, in fact, have suggested an effect of acupuncture, 8 but other researchers have reported that part of the effect may be due to the placebo effect 6 or to an effect on sleep. 5 Further, methodologic weaknesses (for example, a limited sample size 9 ) or differences in acupuncture treatments jeopardize the validity of findings from the literature. With regard to methodologic aspects, several authors suggest that it is difficult to include a control group because the inactive procedures chosen in several studies are actually not inert. 6 –8,10 However, some recent studies have suggested that acupuncture has a positive effect on hot flushes. 5,11,12 Along this line, reviews, meta-analyses, and randomized controlled trials 13 –15 have shown a significant effect of acupuncture and auricular therapy in patients with breast and ovarian cancer 16 compared with sham acupuncture and pharmacologic therapy.
The objective of this study was to evaluate the effects of a treatment with acupuncture on the occurrence of hot flushes and selected menopausal symptoms in women with three or more hot flushes per day.
In this study the treatment was conducted according to TCM. In particular, this study analyzed the effectiveness of acupuncture together with other TCM techniques, which are important in encouraging lifestyle changes (correct diet, self-massage techniques) and help maintain the results obtained with the treatment. This study also analyzed the effect of acupuncture on several menopausal symptoms, including sleep disturbances, irritability, headaches, and loss of memory.
Materials and Methods
This randomized controlled trial was carried out with 4 months follow-up after the end of the treatment. Eligible women were randomly assigned to two groups in sequence by using numbered, opaque envelopes containing treatment allocation.
The women in the first group (group A) were given a diet according to the principles of TCM and were individually taught self-massage. Further, they received treatment with acupuncture immediately after they were enrolled into the study. The women in group B (the control group) were initially given the same diet and self-massage training, but treatment with acupuncture started 6 weeks after they were enrolled into the study.
The study was conducted at the Center of Traditional Chinese Medicine “Fior di Prugna,” a public outpatient clinic of the Florentine health care system. The Ethics Committee approved the study. The women were enrolled between April 2005 and February 2008 from Florence and the surrounding province. The participants were informed of the design and the objectives of the trial, and they all signed a consent form.
Population under study
Inclusion criteria were the following: spontaneous menopause (amenorrhea for ≥12 months but ≤24 months), age 45 to 56 years, and three or more episodes of hot flushes daily. Exclusion criteria were use of HRT within the last month, the use of other medication for the treatment of menopause symptoms, and menopause induced by surgery or chemotherapy. None of the women included in the study needed hormonal treatment, and they were free to access this type of treatment upon withdrawal from the trial.
Recruitment
The study was publicized in newspapers and brochures and through general practitioners and gynecologists. One hundred and forty women volunteered to participate. The first 100 women who met the study criteria were enrolled. These women had a first meeting with a gynecologist, at which they received both written and oral information about the trial and signed the consent form.
Treatment method and therapeutic protocol
Self-massage
All the women received training in self-massage. This was defined according to the theory of Tuina Chinese massage. It foresees a 30-minute massage of the areas (forehead, tempo parietal area, top of the head, ear area, lower back area, abdomen, feet, and ankles plant) in which acupuncture points are present.
Diet
All the women received written material indicating the correct diet for menopause. The diet did not foresee caloric restrictions. The diet was based on the TCM diagnosis (determined by standardized interview, physical examination, and evaluation of pulse and tongue). Women were classified according to the prevalence of yin and yang type, and the prescribed diet took into account these findings. 17 –21 The diet is based on the theory of yin and yang and of the Law of Five Phases. These theories allow interpretation of the psychophysical characteristics of the individual in relation to the surrounding environment.
According to Chinese tradition, the correct diet uses all foods. The type of food chosen is based on the energetic balance of the individual. The basic concept is: “To cure cold with heat, to cure heat with cold.” Foods are divided according to their nature, taste, and color (Table 1). Most enrolled women with hot flushes had yang symptoms. Consequently, the suggested foods had a typology that was predominantly yin.
Acupuncture
The acupuncture sessions were conducted by medical doctors trained at the TCM School of Florence. In Italy, no law regulates training in acupuncture, but in Tuscany, a minimum of 400 hours of postgraduate training after a medical degree is required to perform acupuncture. Practitioners in this study also received specific training before the beginning of the study (8 hours of practical experience) and were supervised by the director of the study.
Treatment for the 6-week period consisted of the following: (1) Twelve sessions, held twice weekly for 6 consecutive weeks, involved stimulation with seven star needles (plum blossom) in the dorsal region C7–T5 (5 minutes); stimulation of three lines in the area of the shoulder blades on both sides was repeated three times on each line with average intensity. (2) Twelve sessions of electroacupuncture (30 minutes), held twice weekly for 6 consecutive weeks, used disposable metal needles on the following points: (a) dispersion with electrostimulation (100 cycles/sec) on GV 23 (23 VG shangxing) towards the nose; CV 22 ( 22VC tiantu), BL 2 (2V zanzhu), LI 11 (11GI quchi), LI 4 (4GI hegu); (b) tonification with electrostimulation (40 cycles/sec) directing the needle toward the groin on SP 10 (10 Rt; Xuehai) and SP6 (6 Rt sayinjiao); and (c) tonification with the needle in the direction of the energetic circulation on GV 20 (20 VG Baihui), CV 4 (4VC guanyuan), CV 6 (6 VC qihai), ST 37 (37 E shangjuxu), and LR 3 (3 F taichong).
The treatment protocol was defined on the basis of individual energy diagnosis conducted according to the theory of yin and yang, the Law of Five Phases, and syndromes prevalent in menopause. 22 In menopause there is usually an insufficiency of the yin of the kidney accompanied by a flare-up of the fire of the liver, deficiency of yang of the kidney or general deficiency of the kidney, stagnation of the blood and accumulation of phlegm and stagnation of the qi of the liver, and disharmony of the heart and kidney.
The basic treatment was the same for all women and included points to tonify the blood (deficient during menopause) and to disperse the heat. Further, an individualized diagnosis was defined on the basis of the theory of yin and yang, the Law of Five Phases, and prevalent symptoms. Thus, we added to the common protocol specific points according to the prevalence of one or more of the five phase or symptoms defined according to the clinical history and examination of the pulse and the tongue. Specifically, in the case of prevalence of specific symptoms, the acupuncturist added predefined points (deficiency of energy [BL 23] and hot flushes during the night [Ht 3]).
The first visit consisted of a 45-minute period during which history, physical examination, and evaluation of pulse and tongue were performed, followed by 30 minutes dedicated to the teaching of self massage. Therefore, the first visit lasted 75 minutes. During the first visit electroacupuncture was not performed. The subsequent sessions consisted of 15–20 minutes for the insertion of needles, 30 minutes for the seat of electroacupuncture, and 5 minutes for the treatment with plum blossom.
Data collection
The participants were interviewed at different times during the study through use of a structured questionnaire. The occurrence of hot flushes and sudden sweating was recorded according to their daily frequency. The following symptoms were recorded according to their weekly frequency: chest pain, irritability, headache, genital bleeding, bone pain, depression, sleep disorders, and breast tenderness.
The symptoms measured by their intensity were vaginal dryness, memory loss, genital itching, urinary tract problems, and skin changes. The following scale was used: 1=no; 2=slight; 3=moderate; and 4=considerable, very marked, serious, intense, or unbearable (as appropriate).
The questionnaire used for assessing menopausal symptoms was the questionnaire defined by the largest Italian scientific gynecological association (Associazione Ostetrici Ginecologi Ospedalieri Italiani) and used in more than 250 menopausal centers in the framework of the 2001 Italian Menopausal Project. 23 The questionnaire that the women filled out upon enrolling into the study included questions about sociodemographic characteristics, obstetric and gynecological history, and family and personal medical history. Group A answered the questionnaire during an interview upon enroll and after treatment was completed. Group B filled out the questionnaire (via an interview) upon enrollment, before starting acupuncture treatment, and after completing it.
Four months after treatment end, each participant was contacted by phone and the questionnaire was completed again. At this point the participants were asked about their general health. In particular, each woman was asked whether her perception of general health was definitely improved, a little improved, more or less the same, a little worse, or definitely worse.
Statistical analysis
Statistical analysis was carried out with Stata SE software, version 10.0 (Stata Corp., College Station, Texas). The outcome variables were converted into scores. The chi-square test was used to verify any significant differences in the qualitative variables between the two groups, and the t test was used to assess significant differences between the scores on the two groups. To evaluate the effectiveness of the treatment, improvement was calculated as the difference between the scores at the beginning and end of treatment for group A and between enrollment and six weeks later for group B. The significance of the differences in improvement between the two groups was tested using the t test.
The linear regression model allowed adjustment for variables that could have influenced results, such as alcohol or sedative use, the presence of thyroid disease, hypertension, and the initial state of symptoms. A paired t test was performed among the women in group A to test the equality of score at the end of the treatment and at follow-up (4 months later). A paired t test was also used in group B to test the equality of score improvement between recruitment and the beginning of treatment and the score improvement between the beginning and the end of treatment.
Results
Figure 1 shows groups A and B during the different phases of the study. The 100 women who participated in the trial were 51 years old on average and were predominantly Italian (90%); all were Tuscany residents. Sociodemographic characteristics (education, marital status), alcohol intake, and thyroid diseases that could have influenced menopause symptoms did not significantly differ between groups. In particular, alcohol intake during the study period did not change markedly, and only one woman in group A reported drinking more than two glasses of wine per day. Five women in group A and seven in group B reported thyroid diseases (p=not significant). No association emerged between alcohol intake, sedative drug use, and history of hypertension or thyroid diseases and frequency of menopausal symptoms.
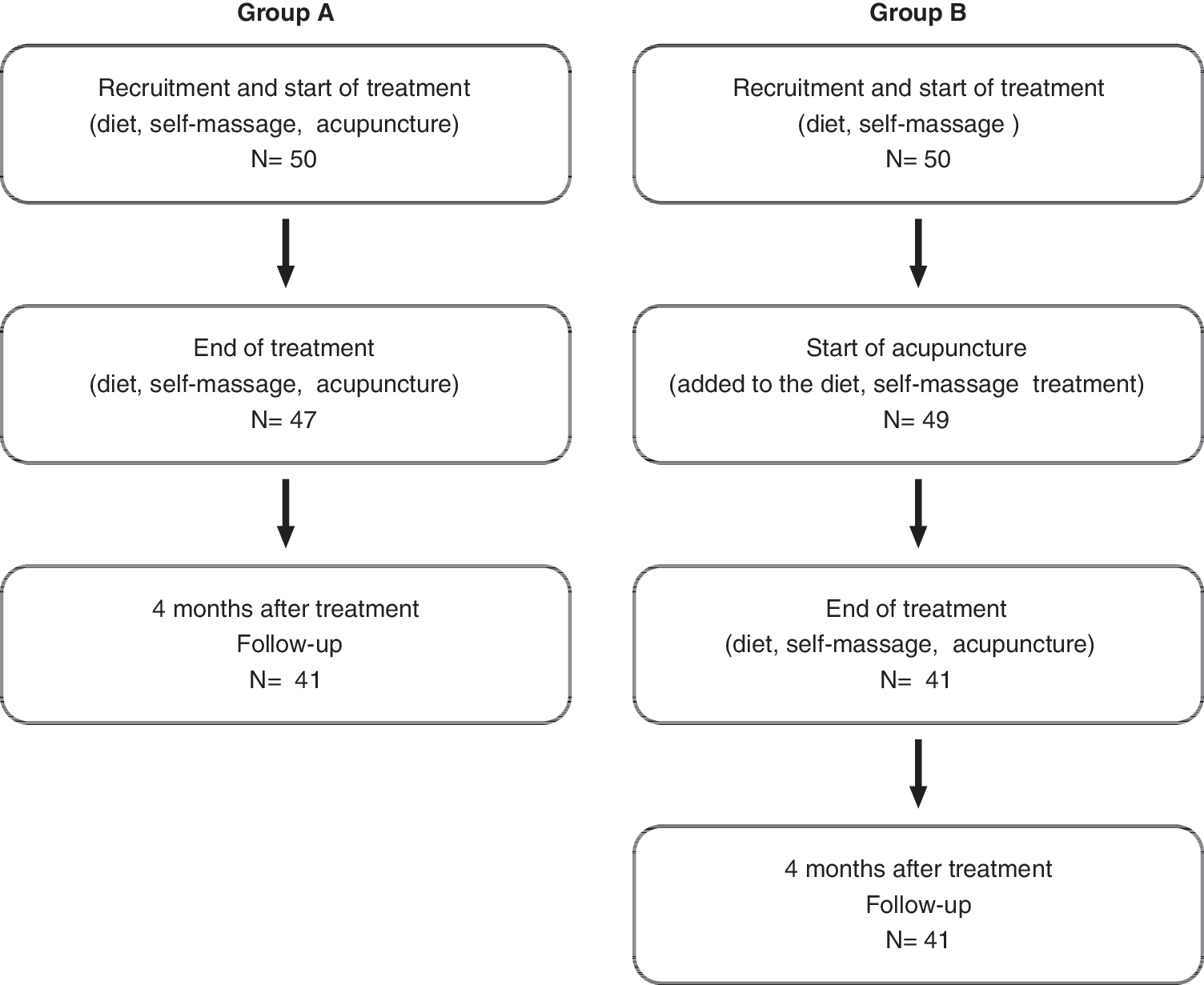
Flow of patients throughout the study.
Table 2 shows the average scores (standard deviation) of menopause symptoms that women experienced during the 2 weeks preceding the interview. There were no significant differences related to the frequency and intensity of symptoms with the exception of vaginal dryness, which was more frequent in group A. The mean scores for hot flushes, sudden sweating, and sleep disturbances were 3 or higher.
At the end of treatment, group A showed a statistically significant mean improvement in frequency and intensity score compared with women in group B for hot flushes, sudden sweating, sleep disorders, irritability, bone pain, feeling depressed, headache, chest pain, memory loss, vaginal dryness, skin changes, urinary tract problems, and genital itching (Table 3).
Values expressed with a plus/minus sign are the mean±standard deviation.
Differences of mean score improvement adjusted for alcohol or sedative use, the presence of thyroid disease, hypertension, and the initial state of symptoms.
CI, confidence interval.
Forty percent of the women in group A stated that their general health had improved considerably, and 42% indicated a slight improvement. Most women in group B (86%) said that their general health had not changed. The same question was asked in reference to menopause symptoms only: Sixty-four percent of the women in group A reported a significant improvement and 42% a slight improvement, while 84% of the women in group B reported no change in their symptoms. The women in group A declared an improvement in all symptoms at the end of the treatment (self-massage, diet, and acupuncture) with respect to recruitment (Table 4). All symptoms significantly improved, with the exception of breast tenderness (an infrequent symptom) and genital bleeding (present in only two women).
Values expressed with a plus/minus sign are the mean±standard deviation.
After adjustment for factors that could influence the outcome, the difference in the improvement of scores in group A was significantly greater than that in group B: 1.3 points for hot flushes; 1.2 for sudden sweating and skin changes; 1.1 for sleep disorders; 1.0 for headache, chest pain, and vaginal dryness; 0.9 for irritability, bone pain, memory reduction, and urination disorders; 0.7 for depression; and 0.5 for genital itching.
Considering the average scores at the end of the treatment and the average scores 4 months after the completion of the treatment for the women in group A, the results obtained at the end of the treatment and at follow-up did not differ except for vaginal dryness, skin changes, and vaginal itching. These symptoms worsened, and consequently their scores were higher at follow-up; however, the difference was statistically significant only for vaginal dryness (Table 5).
Values expressed with a plus/minus sign are the mean±standard deviation.
Among women in group B, the average improvements experienced during the period when they received dietary information and training in self-massage in comparison with the period in which they received dietary information, training in self-massage, and acupuncture treatment were in most cases statistically significant.
Discussion
The results of this study show that plum blossom therapy in an integrated system that includes therapeutic techniques, such as diet therapy and Tuina self-massage, had a statistically significant effect on menopausal hot flushes, as well as on sudden sweating, skin changes, sleep disorders, headache, chest pain, vaginal dryness and genital itching, irritability and depression, bone pain, memory reduction, and urination disorders.
The incidence of hot flushes and sudden sweating (p<.001) improved in accordance with other randomized controlled studies. 5,11,12 These studies indicated positive effects of acupuncture on vasomotor symptoms and health in general, also compared with HRT. 24,25 Sleep disorders, irritability, depression, memory loss, headache, chest pain, vaginal dryness, bone pain, and urinary tract problems improved significantly. This finding is consistent with those reported in previous studies. 5,12,26
Despite these favorable results, it is still not fully understood how acupuncture relieves menopause symptoms. Researchers have reported effects on the function of the hypothalamic-pituitary-ovarian axis on the central nervous system, with changes in the levels of some neurotransmitters (such as serotonin, 27 β-endorphins, and neuropeptides 28 ) and on the secretion of melatonin at night. 29
The control group consisted of women who received dietary instruction and training in self-massage instead of sham acupuncture because this type of control group is known to present methodologic problems concern. 30 Almost every recent study that examined verum and sham acupuncture interventions for menopausal symptoms demonstrated no statistically significant differences between the two interventions. 31 –33 In systematic reviews, Lee and colleagues 34 and Cho and colleagues (2009) 35 found an improvement in vasomotor symptoms in groups treated with both traditional and sham acupuncture, but there was no difference between the two groups. 8,35 It is conceivable that comparing the effects of acupuncture and sham acupuncture can underestimate the actual benefits of acupuncture because sham acupuncture is not inactive, as a placebo is supposed to be.
It is important to emphasize that treatment with acupuncture has practically no adverse effects, has no contraindications, and is associated with a high level of adherence and concordance on the part of the patient. 36,37
This study used TCM as a whole and integrated system that included therapeutic techniques such as diet therapy and Tuina self-massage; plum blossom and acupuncture, which are the TCM techniques best studied in the Western world, were also added. The initial assumption was that the integration of several techniques could enhance the therapeutic effect; therefore, this study compared the set of treatments from classic Chinese medicine with acupuncture and plum blossom, added or removed in the control group.
In the study sample, a TCM therapeutic diet and self-massage were not sufficient to relieve menopausal symptoms, including hot flashes. In conclusion, acupuncture in an integrated system that includes therapeutic techniques such as diet therapy and Tuina self-massage, plum blossom can be an effective treatment to deal with the symptoms of menopause. It is recommended for women who cannot be treated with HRT because of oncologic risks or because of an ongoing or past oncologic pathology. It is also advisable when patients who have declined HRT or have already been treated with HRT continue to experience hot flushes, psychological problems, insomnia, and other symptoms.
Footnotes
Acknowledgments
The authors dedicate this article to Eva Buiatti, an epidemiologist of worldwide renown, who was deeply committed to designing and carrying out this randomized controlled trial. Her great scientific interest in the evaluation of complementary medicine and her professional expertise helped us achieve strong relationships among the Regional Bioethics Committee, the community of researchers, and the public clinics of complementary medicine, all sharing a common scientific methodology.
The authors gratefully acknowledge Barbara Cucca and Barbara Meyer, staff of the Center of Traditional Chinese Medicine Fior di Prugna, for their assistance while the trial was under way and in proofreading, as well as their comments during the preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.