
Abstract
Purpose:
Diabetes mellitus with coronary heart disease (DM with CHD) poses a health challenge to people in China and elsewhere in the world. In Traditional Chinese Medicine (TCM), DM with CHD is classified as a type of disease called Xiaoke and Xiongbi. In Asia, TCM has been used to treat Xiaoke and Xiongbi conditions for centuries, especially in China. In this study, it was evaluated whether integrated strategies incorporating both TCM and Western medicines (iTCWM) could improve the curative efficacy of DM with CHD.
Methods:
An extensive search for randomized clinical trials (RCTs) published up to November 2011 in either English or Chinese about iTCWM for DM with CHD was conducted. All listings in PubMed, EMBASE, the Cochrane Library, CBM, CNKI, VIP, and the Wanfang database were included in the literature search. The quality of each trial was assessed using the Cochrane Reviewers' Handbook 5.0. Data analysis was performed by the RevMan 5.0 provided by the Cochrane Collaboration.
Results:
After an initial selection of 207 articles, 21 RCTs and quasi-RCTs were ultimately included in the analysis for this study. All of these trials were conducted in China and published in Chinese journals. The methodological quality of the trials was low in most studies. Selection bias and measurement bias were common in all of the studies. A meta-analysis was not conducted, due to the poor quality of the available studies.
Conclusions:
The current state of the literature regarding the utility of iTCWM for the treatment of DM with CHD is inadequate. The poor quality of the available trials makes it difficult to draw any conclusions regarding the efficacy of iTCWM for the treatment of DM with CHD. This study highlights the paucity of reliable clinical evidence for iTCWM and the need for higher quality RCTs to be conducted in the future.
Introduction
Until now, large numbers of clinical studies have reported on the effects of DM with CHD in patients treated with iTCWM. The objective of this systematic review is to determine whether iTCWM can effectively treat DM with CHD. In this article, iTCWM is defined as any intervention that integrated Chinese herbal medicine and Western medicine.
Methods
Types of studies
A search was done for randomized and quasirandomized clinical trials (RCTs) published before or during November 2011 that evaluated iTCWM for DM with CHD. Both blind and nonblind studies were included in the literature search.
Types of participants
Trials included adult patients who suffered from DM with CHD irrespective of age, sex, and etiology. DM with CHD was diagnosed either according to the World Health Organization criteria or relevant Chinese diagnostic criteria. 4 –6 Patients with DM with other heart diseases, such as myocardosis, peripheral angiopathy, cardiac autonomic neuropathy, were excluded.
Types of interventions
Trials that met the following criteria were included in the present review: The treatment group had to be treated using an iTCWM method with or without routine care, and the control group had to be treated using Western medicine, alone or with routine care. The treatment method used in the control group was defined as conventional treatment (CT). The kinds of TCM used in iTCWM included decoctions made with herbal medicines, Chinese patent drugs regardless of form (e.g., liquids, powders, pills, and capsules). Patients treated using acupuncture were excluded from this review. The endpoints for all of the included studies included effective rate, blood glucose levels, blood lipid levels, adverse events, and similar factors.
Study selection
A search strategy was established according to the Cochrane version 5.0.2. Different search strategies were used in different databases. The following were searched: the Cochrane Central Register of Controlled Trials (2011, Issue 4), PubMed (1950–2011), EMBASE (1985–2011), Chinese Biomedical Database (CBM, 1979–2011), Chinese journal database (CNKI, 1978–2011), VIP Chinese periodicals database (VIP, 1985–2011), and the Wanfang database (1990–2011). The key words were
Two (2) reviewers independently examined the titles and abstracts of the trials that corresponded to the inclusion criteria. The full texts of articles were retrieved if there was any doubt whether an article should be included or not. Inconsistencies were addressed through discussion.
Quality assessment
The quality of the trials evaluated here was assessed according to the Cochrane reviewers' handbook. The limitations of the included trials were evaluated using the following steps: (1) whether the study participants had been properly randomized; (2) whether allocation concealment had been conducted; (3) whether the blinding method had been used; (4) whether the baseline was consistent; and (5) whether patient follow-up status had been described. The quality of evidence was evaluated using the JADAD-score. 7
Data extraction and analysis
Information regarding patients, methods, interventions, outcomes, and results was extracted and summarized independently by 2 individual reviewers using a standardized data extraction form. Indeterminacy was resolved through discussion among all investigators.
The software provided by the Cochrane Collaboration (Review Manager 5.0) was used to statistically analyze the data. 8 For dichotomous outcomes, the number of responders and the total number of participants for each trial were extracted. For continuous outcomes (e.g., fasting blood-glucose [FBG], postprandial blood glucose [PBG], glycosylated hemoglobin [HbA1C], total cholesterol [TC], triglycerides [TG], low-density lipoprotein cholesterol [LDL-C], high-density lipoprotein cholesterol [HDL-C]), the mean change and standard deviation for the mean in each group of the trial were extracted along with the total number.
Results
Search flow
Using this search strategy, 207 potentially relevant studies were identified. After evaluating each of the titles and abstracts, it was possible to exclude 86 studies that were clearly duplicates, cell or animal experiments articles, reviews, case reports, or nonclinical studies. After review of the full text, 121 articles were excluded because they were not RCTs, patients did not satisfy the inclusion criteria, baseline data were missing for outcome measures (effective rate [ER], blood glucose level, blood lipid level) (Fig. 1). Ultimately, 21 trials were included in this systematic review. All of the included studies were carried out in China within the past 11 years (1999–2009) (Fig. 1). Twenty (20) of these trials described the baseline characteristics (e.g., sex, age, course of disease) of the patients included in the trials. All of the included studies were single-center and parallel-design trials and claimed to have applied randomization.

Article selection flowchart. RCTs, randomized controlled trials; TCM, Traditional Chinese Medicine.
Characteristics of the trials included in the study
The main characteristics of the 21 trials are given in Table 1. 9 –30 The 21 trials included a total of 2006 patients and the number of participants in each study ranged from 45 to 260. Four (4) trials were found that did not indicate the exact number of female and male patients. The overall proportion of males and females was approximately 53% and 47%. Patient age ranged from 34 years to 80 years. The diagnostic criteria for DM with CHD were specified in all of the 21 trials, the inclusion criteria were indicated in 6 trials, and the exclusion criteria were indicated in 9 trials, but only 3 trials listed all of the diagnostic, inclusion, and exclusion criteria. The duration of treatment ranged from 15 days to 4 months.
CT, conventional treatment; HI, hemorrheologic indices; BG, blood glucose; BL, blood lipid.
Articles were included that compared the effects of iTCWM and CT on DM with CHD. Traditional Chinese medicines used in these studies included both herbal medicines and Chinese patent medicines. CT included Western medicines and basic treatments such as exercise and dietary control. Multiple outcomes were evaluated at the end of treatment in all 21 studies (Table 1). Seventeen (17) trials used the ER to evaluate treatment efficacy. Only one trial reported the follow-up period. Three (3) trials reported adverse events. One (1) trial reported the aggravated case. No trials reported mortality.
Methodological quality
All 21 trials used some form of randomization. Six (6) trials used a randomization table. 9,16,18,25,26,29 Three (3) clearly described a random number table. 16,18,29 One (1) trial reported that the random sequence had been generated by the throwing-coin method. 20 No trials described allocation concealment. Five (5) trials reported blinding procedures. Of these, four trials were single blind and one trial was double blind. No trials described intention-to-treat analyses (ITT) or the method of assessing compliance. In general, the methodological quality of the included trials was poor (Table 2). Most trials had Jadad scores of 1–2, and only one trial had a score of 3.
① randomized table; ② random digits table; ③ throw coin method; ④ single blinding method; ⑤ double blinding method.
Effective rate
Most of the included trials (15/21) used the ER as a measure of outcome. The ER was counted as the ratio between the proportion of responders in the treatment group and the proportion of responders in the control group. For DM with CHD, responders were defined as patients who showed improvement in electrocardiogram (ECG), reductions in the number of heart attacks, and improvement in TCM symptoms. Because the ERs reported for ECG and the frequency of heart attacks in patients with and without TCM symptoms were similar, separate figures were not used to compare the studies. The forest plot in Figure 2 indicates the results of the studies using the ER as a measure of outcome. Twelve (12) studies were found to be statistically significant with respect to ER. This shows that iTCWM can improve ECG, reduce the rate of heart attacks, and resolve the TCM symptoms. The other three studies showed no statistical significance.
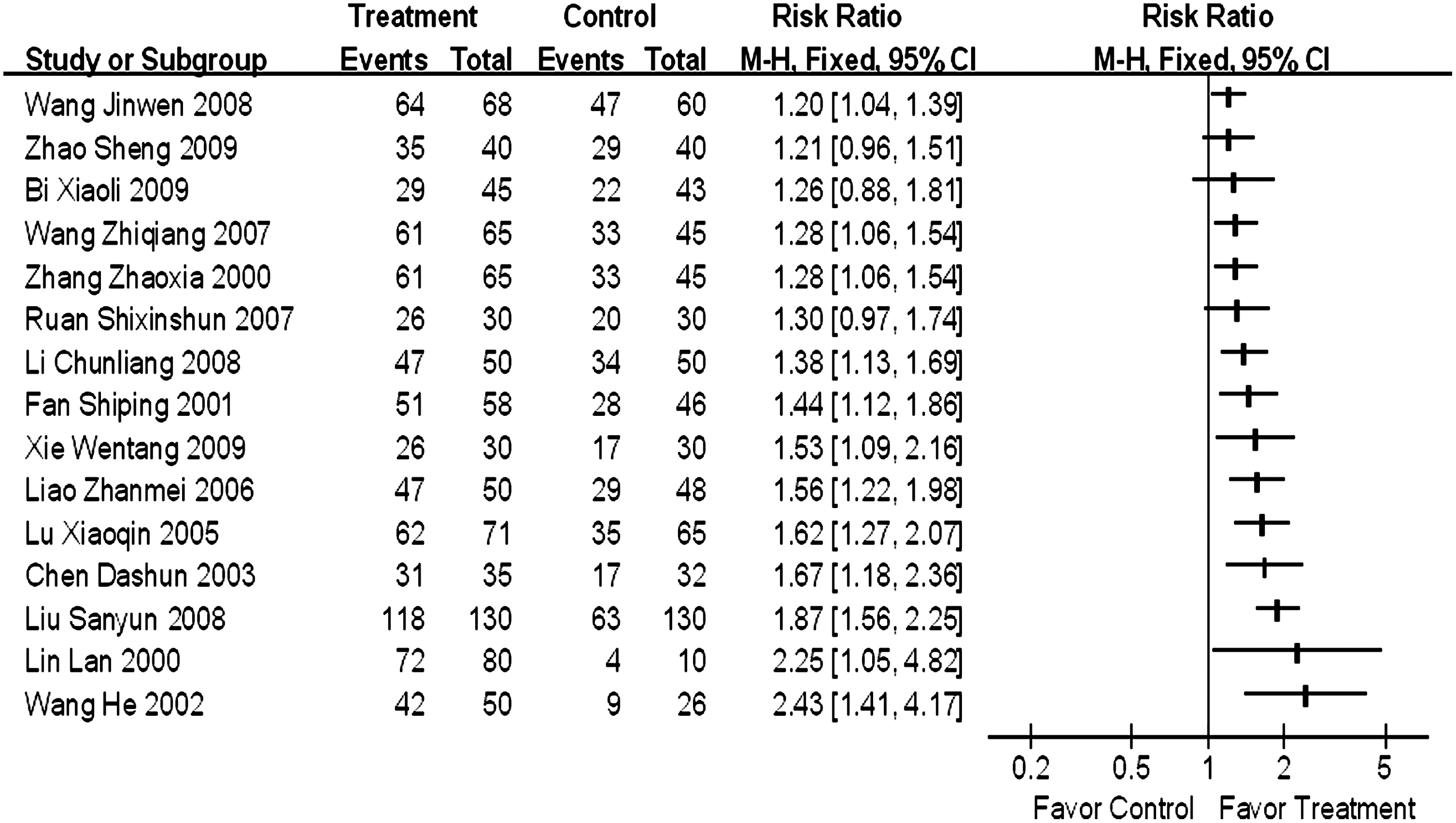
Effective rate of integrated Traditional Chinese Medicine and Western Medicine for diabetes mellitus with coronary heart disease. M-H, Mantel-Haenszel methods; CI, confidence interval.
Blood glucose
In patients with diabetes, blood glucose level is usually used to evaluate drug efficacy. The indexes used to assess the blood glucose level include FBG, PBG, and HbA1c. Seventeen (17) studies reported the outcomes for FBG. Eleven (11) studies reported the outcomes for PBG. Only five studies reported HbA1c results. The results of the trials that used FBG, PBG, and HbA1c as measures are reported in the forest plot in Figure 3. Among studies that used FBG as an indicator, eight showed that iTCWM tended to decrease FBG more effectively than CT, but the other eight studies showed no statistically significant differences between the two types of treatment. For PBG indicator, four studies showed that iTCWM was able to reduce PBG more effectively than CT group, but the other five studies had no statistically significant results. For HbA1C, two studies showed no statistically significant difference between iTCWM and CT, and three studies showed that iTCWM reduced HbA1C more effectively than CT.
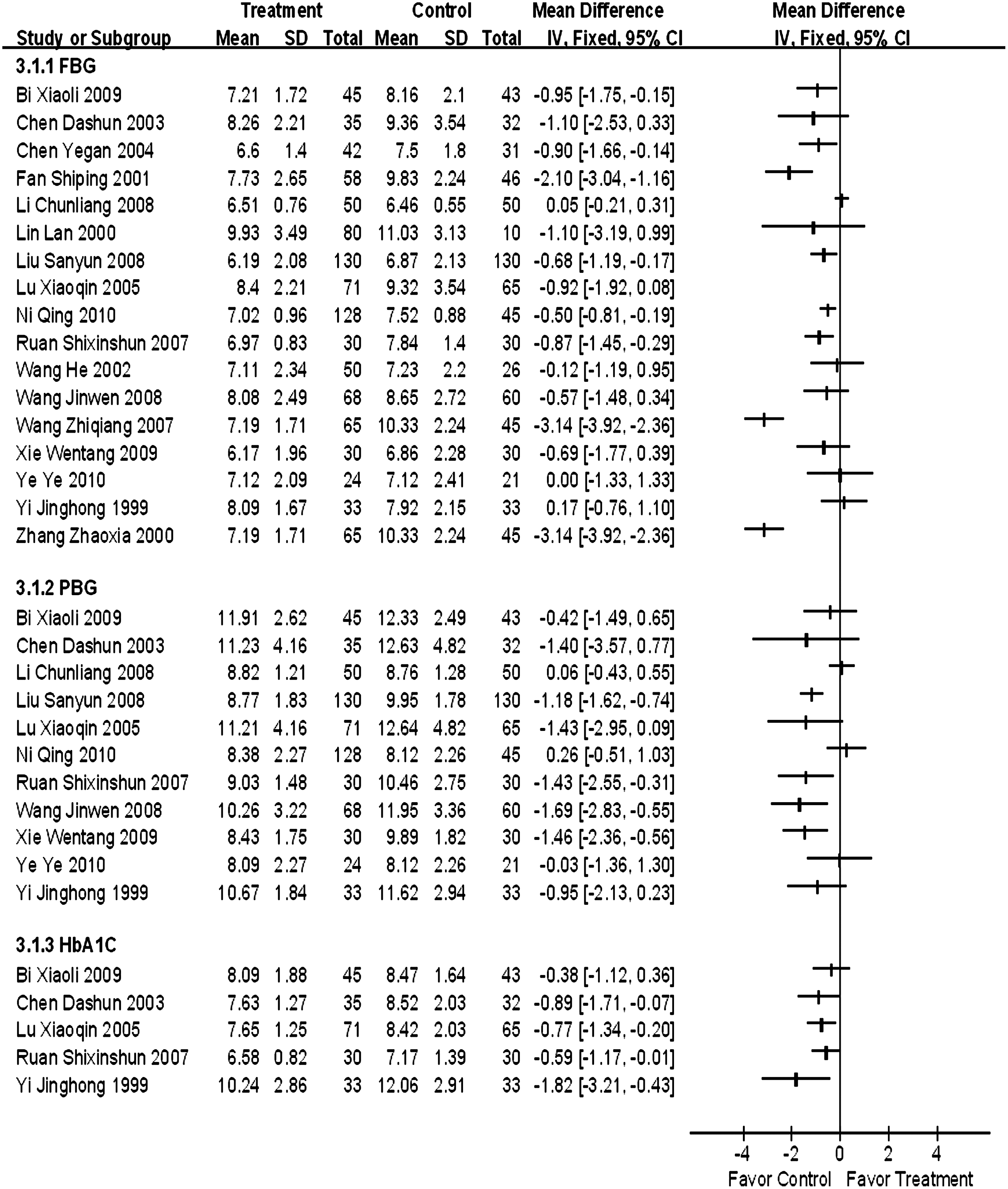
Blood glucose of integrated Traditional Chinese Medicine and Western Medicine for diabetes mellitus with coronary heart disease. SD, standard deviation; CI, confidence interval; FBG, fasting blood glucose; PBG, postprandial blood glucose; HbA1C, glycosylated hemoglobin.
Blood lipid levels
TC, TG, LDL-C, and HDL-C levels were used as indices to screen CHD. 31 Some trials used blood lipid levels as an additional outcome to assess treatment efficacy. Twelve (12) studies reported TC and TG levels before and after treatment. Among these 12 studies, 8 studies also reported outcomes of HDL-C and LDL-C. Only one trial used mg/dL as the units of blood lipids. 11 The other trials used mmol/L as the unit of blood lipid level. These are reported in the forest plot in Figure 4.
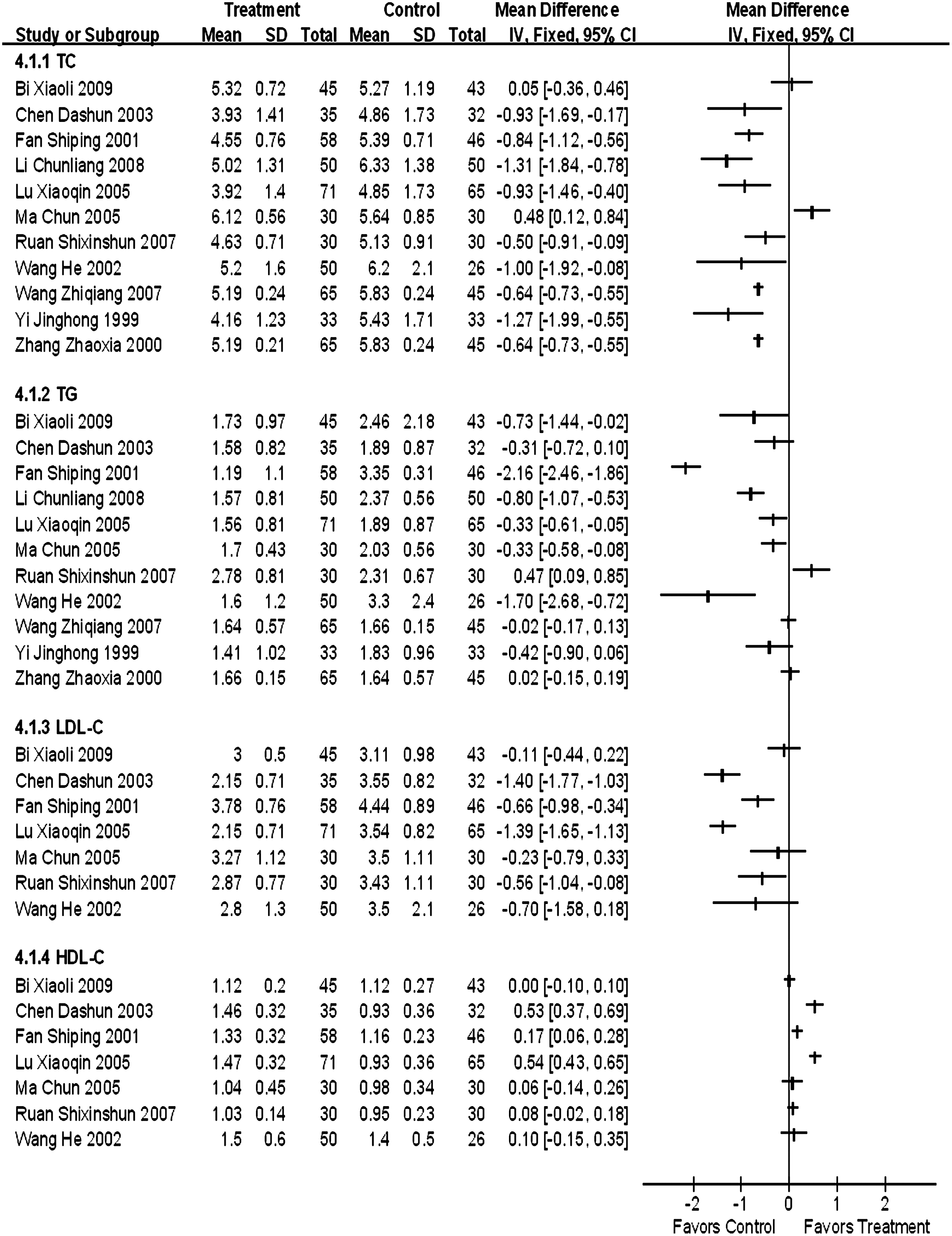
Blood lipid level of integrated Traditional Chinese Medicine and Western Medicine for diabetes mellitus with coronary heart disease. SD, standard deviation; CI, confidence interval; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein; HDL-C, high-density lipoprotein.
Nine (9) studies showed that the iTCWM could decrease TC more effectively than CT. The other two studies showed no statistically significant differences between these two treatments. Five (5) studies showed that iTCWM reduced TG more effectively than CT. The other five studies showed no statistically significant differences between these two treatments. For LDL-C, three studies showed no statistically significant differences between iTCWM and CT, and the other four studies showed that iTCWM could reduce LDL-C more effectively than CT. For HDL-C, four studies showed no statistically significant differences between iTCWM and CT, while the other three studies showed that the iTCWM could improve HDL-C more effectively than CT.
Adverse events
Fifteen (15) studies reported adverse events. Liao reported that two participants in the control group withdrew from the study due to serious sinus bradycardia. 15 Researchers did not analyze the reason for this sinus bradycardia, but we concluded that it had nothing to do with TCM because it only occurred in the control group. Other adverse events included mild headache and mild gastrointestinal reactions. 9,17 These adverse symptoms disappeared after medication adherence or dose reduction. Ruan et al. reported two cases of aggravated patients in the control group. 23
Funnel plot
Funnel plots based on the data for ER, mean difference of blood glucose, and blood lipid are given in Figure 5. The asymmetrical shapes of these funnel plots indicate potential publication bias, which may influence the results of this systematic review.

Funnel plots of
Discussion
This review includes a total of 21 trials, all of which evaluated the effects of the iTCWM method compared to CT methods in patients with DM with CHD. The primary outcomes of the DM with CHD were the ER, blood glucose level, and blood lipid level. Most of the trials included in this analysis evaluated these outcomes. Results indicated that, in general, the effects of iTCWM were no worse than those of CT. In some cases, iTCWM showed better results than CT. However, because of several problems, it could not definitively be proven that iTCWM is superior to CT.
The primary reason for this is the low methodological quality of the individual studies. Only 19% of the trials reported all inclusion and exclusion criteria, all of which can affect baseline information. Although all the trials claimed to have used randomization methods, only seven of them described the specific method of randomization. Inappropriate randomization can lead to selection bias. Allocation concealment was not mentioned in any of the trials, but it is just as important as randomization with respect to preventing bias. Because allocation was not concealed, the effects of intervention may have been exaggerated by 30%–40%. 32 Of these 21 trials, only 5 were performed blinded. Four (4) of these were single blinded and one was double blinded. None of these trials described how blinding was conducted. The lack of appropriate blinding can result in measurement bias. The reason why blinding was not used in most trials is possibly because of the difficulty in making convincing placebo versions of TCMs. Only one trial gave details on the duration and specific nature of patient follow-up. Dropouts were reported in two trials, but no ITT were performed. No other trials provided dropout information, and it was unclear whether these studies had any dropout cases. In conclusion, the methodological quality of the individual studies was low, and their results were found to be insufficiently reliable. In order to produce more reliable evidence, future studies should place more emphasis on follow-up research and overcome the drawbacks discussed above.
One of the advantages of TCM is the potential for reduced adverse events compared to Western medicine. Therefore, evaluating the adverse events of iTCWM is an important aspect of this review. Fifteen (15) studies recorded the presence of any adverse events, with only 3 of the studies reporting any details regarding the types of symptom and the number of events. No details were provided with respect to the degree, time of occurrence, or duration of the adverse events. No evaluation was performed of the relationship between the adverse events and medicines given.
Treatment based on syndrome differentiation is an important characteristic of TCM. The TCMs used in these 21 trials included Chinese patent medicines (injections, pills, and capsules) and herbal prescriptions. Because treatment is so often based on syndrome differentiation, the prescriptions used to treat the DM with CHD can differ. A large number of trials failed to report the precise composition and dose of each prescription. In herbal preparations, quality control is very important for the critical appraisal of the results. All participants should be given exactly the same intervention in terms of production identity, purity, dosage, and formulation for the results to be reliable. Studies that meet these criteria will be more persuasive than those that do not.
Another limitation that was found in this systematic review was that all the trials were conducted in China and published in Chinese journals. No articles reported negative results. Location and publication bias may be unavoidable.
Conclusions
In order to evaluate the efficacy of TCM more thoroughly, the Chinese government increased the investment into the research of TCM. Among the 21 studies included in this systematic review, only 7 were funded by the national or local governments. The authors believe that higher-quality RCTs on the effects of TCM and iTCWM are needed in the coming years. In the future, low-level studies should be avoided and more attention paid to perform large-sample, multicenter, randomized controlled trials with double-blind designs.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81102683 and No. 30973813) and the Doctoral Fund of the Ministry of Education of China (No. 20110001120055).
Disclosure Statement
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.