
Abstract
Objectives:
This study evaluated a simple relaxation breathing exercise for acute improvement of postprandial glycemic and insulinemic status.
Design:
Healthy human subjects were randomized to control breathing (CB; n=13) or a relaxation breathing exercise (RB; n=13) that was repeated every 10 minutes for the 30 minutes before and 90 minutes after consuming a glucose challenge (oral glucose tolerance test; OGTT; 75 g/240 mL). Blood samples were collected before, and 30, 60, and 90 minutes post OGTT for glucose and insulin analysis.
Results:
Blood glucose at 0 minutes (pre-OGTT), and 30, 60, and 90 minutes post-OGTT with continued RB was 93.7±1.9, 136.5±8.1, 165.7±8.1, and 130.2±6.9 mg/dL, and 97.1±2.4, 173.1±8.4, 158.7±11.1, and 137.1±10.1 with CB, respectively. RB blood glucose was significantly lower at 30 minutes than CB. Glucose area under the curve (AUC) for CB and RB were not significantly different. Plasma insulin for both CB and RB was significantly increased relative to baseline at 30, 60, and 90 minutes. Insulin values for RB tended to be higher than CB at 30 and 60 minutes, although the difference was not statistically significant. Insulin AUC for CB and RB was not significantly different.
Conclusions:
Relaxation breathing acutely improves the glycemic response of healthy subjects, and breathing pattern could be important for interpretation of glycemic index measurements.
Introduction
Glucose tolerance in humans is known to be impaired by hypoxia, and sleep apnea is a hypoxia condition that is highly correlated with type 2 diabetes. 9 –11 Administration of hyperbaric oxygenation improves oxygenation and appears to improve glycemic status in those with type 2 diabetes. 12 While a 3-week intervention with meditation and relaxation breathing has been suggested to improve postprandial glycemic status, 13 the acute effects of relaxation breathing on postprandial glycemic response remain unclear. The present study sought to determine the effect of a simple and clinically reproducible relaxation breathing exercise on the glycemic and insulinemic response to an oral glucose tolerance test (OGTT; 75 g dextrose/240 mL) in healthy college-aged subjects.
Methods and Materials
Participants and study design
This study was approved by the Winona State University Human Subjects Committee with health exclusions including diabetes, smoking, asthma, or sleep apnea. Healthy subjects (21 female and 5 male; 20.1±0.2 years old; and a body mass index of 22.8±2.5

Relaxation breathing pattern repeated every 10 minutes of study. Each arrow represents a slow deep inhalation lasting 2 seconds, followed by an expiration of the duration listed in the circle starting at 1 second and was increasing with each expiration until a 10-second expiration was reached.
Following an overnight fast (9 hours) with exclusion of all food and beverages except water, subjects arrived at between 5:00
Data analysis
Values are reported as mean±standard deviation. Following analysis of variance, a repeated-measures analysis was completed using SAS Version 9.0 to examine time and treatment as independent variables using repeated measures, least mean squares, and a Tukey adjustment for multiple comparisons. Area under the curve (AUC) values were calculated using the trapezoidal method and statistically analyzed using a Student's t-test. Statistical significance was assumed when p<0.05.
Results
The RB exercise was found to be acceptable by all subjects, with no subjects stopping study participation because of respiratory pattern noncompliance. A total of 31 healthy college-aged subjects started the study; 3 subjects left the study because of nausea after consuming the OGTT beverage, and 2 left due to fainting during blood collection, with 26 persons completing the study. The glycemic response to RB is shifted down and to the right relative to CB (Fig. 2). The 30-minute postprandial glucose concentration (Table 1) of both treatment groups was significantly increased relative to baseline, but the peak blood glucose was significantly lower for those performing RB (136.5±8.1 mg/dL) relative to CB (173.1±8.4 mg/dL). Blood glucose for both RB and CB remained significantly elevated relative to baseline at 60 minutes, although the difference between RB and CB was no longer significant. Glucose AUC (Table 1) was slightly lower for RB than CB (12,717±567 versus 13,832±595 mg/dL-90 minutes), demonstrating a trend toward significance (p=0.091). Plasma insulin was significantly increased following OGTT administration for both CB and RB relative to baseline at 30, 60, and 90 minutes, with the peak being reached at 60 minutes (Table 1). While insulin tended to be higher in the RB group, no statistically significant differences between the two treatment groups were observed, nor was the insulin AUC for CB and RB significantly different (Table 1).
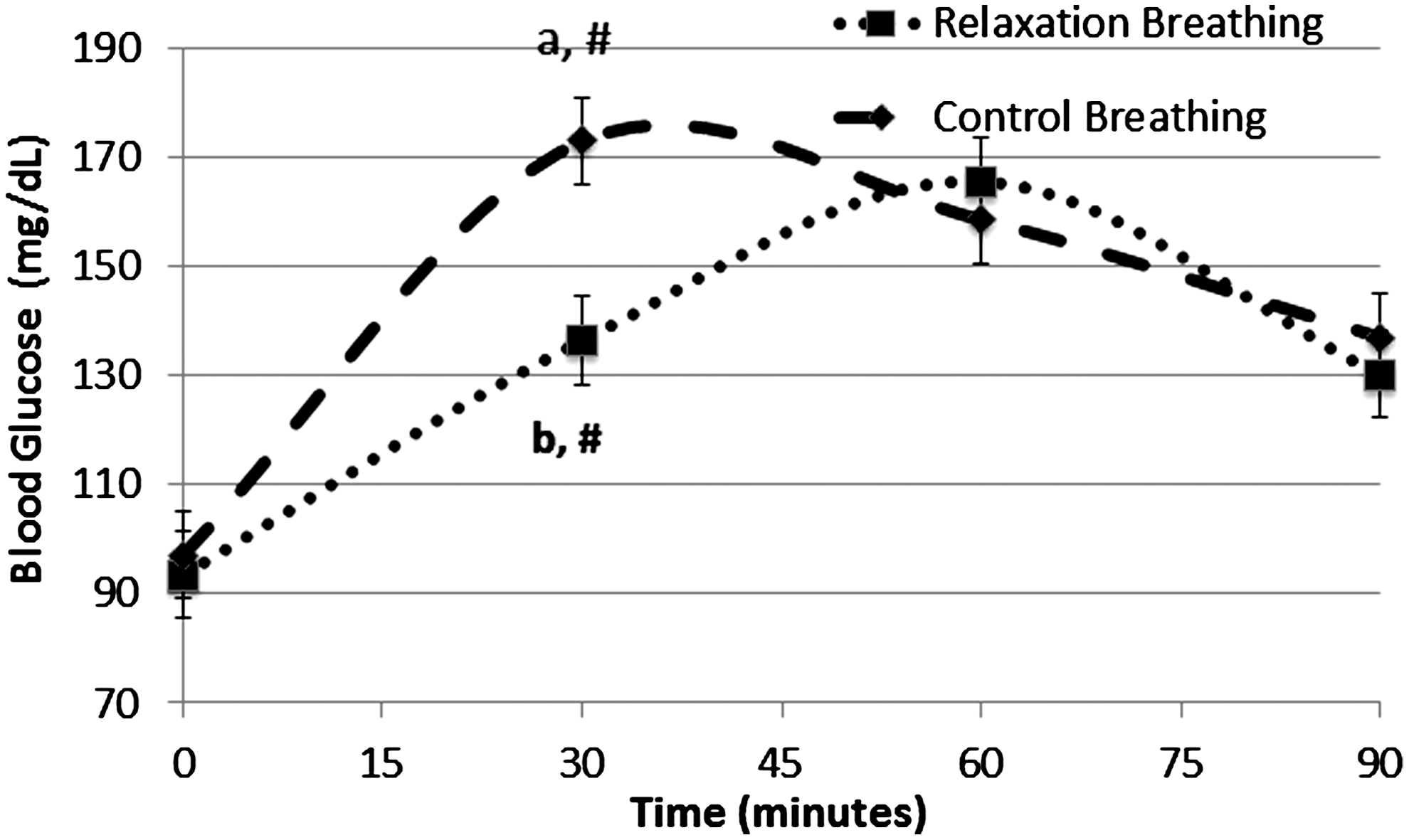
Changes in blood glucose in response to an oral glucose tolerance test (75 g dextrose/240 mL). Relaxation breathing was associated with significantly lower blood glucose at 30 minutes than persons using control breathing.
Data expressed as mean±standard deviation.
Statistical significance: difference from baseline (0 minutes) indicated by #, differences between treatments at same time indicated by letters.
Discussion
The practice of yoga in a general sense is often associated with intentional alteration of one's breathing pattern. However, there are many versions and interpretations of yoga; therefore, clinical assessment of breathing pattern on glycemic and insulinemic response to an OGTT is difficult. The practice of yoga is associated with physical stretching, meditative, and other physical activities that could also influence response to an OGTT. The current study limited the effect of these confounding factors and created an experiment wherein respiratory pattern was the primary condition that was altered. The RB exercise limited the effect to just breathing pattern on human glycemic and insulinemic response to an OGTT.
RB before and during an OGTT was associated with an improved glycemic response. Blood glucose at 30 minutes for those practicing a RB exercise was 36.6 mg/dL lower than CB. In addition, the glucose AUC was lower with a trend toward significance (p=0.091). In contrast, at 60 minutes, RB was associated with blood glucose that was slightly, and nonsignificantly higher than with CB. This observation may have been due to improved insulin sensitivity, increased insulin secretion, or delayed gastric emptying while performing RB. In the authors' previous glycemic and insulinemic response trial examining healthy college-aged populations, a smaller 140-calorie challenge resulted in a peak glucose within 30 minutes of consumption. 14 Other studies examining similarly aged healthy populations have been observed a 75-g OGTT response that was similar to the present study. 15 –17 In the present study, RB was associated with a blunted appearance of the glycemic peak (60 minutes) in contrast to these prior studies where the blood glucose peak was in response to a 75-g OGTT at around 30 minutes. RB breathing could have caused these effects by slowing the rate of gastric emptying; however, to the authors' knowledge, there are no published reports that RB can alter gastric emptying time. Future studies may wish to examine this possibility more closely, especially in persons with known insulin resistance (i.e., type 2 diabetes).
RB-dependent improvements in glycemic response to the OGTT could have been more robust in a population whose arterial oxygenation is already known to be impaired. Hypoxia is induced by severe pneumonia, and hyperglycemia is used as a marker of pneumonia severity in nondiabetics. 18 Yoga breathing has been suggested to improve arterial oxygenation in persons with chronic obstructive pulmonary disease. 19 Given that the subjects in the current study were healthy, it is unlikely that this difference could have been statistically detected using finger-pulse oximetry without very large study population sizes; therefore, oximetry measurements were not attempted in our study regimen. Future studies of RB in populations known to experience hypoxia, such as those with chronic obstructive pulmonary disease or pneumonia, could provide a useful assessment of the potential benefits of RB.
Indexing foods to a standard glycemic index helps consumers choose foods with a more favorable glycemic response for improved nutritional health. 20 Clinical glycemic index (GI) reference values exist for nearly all foods, and these values are central to many nutrition counseling regimens, especially for those applied to persons with metabolic syndrome and diabetes. The present study suggests that subject breathing pattern at the time of food GI evaluation may influence the measurements used to calculate a food's GI value. Future GI measurement guidelines may wish to describe the use of a standardized breathing pattern.
Conclusions
RB exercises improve the glycemic response in healthy college-aged persons and could provide an inexpensive nonpharmacological way to improve postprandial glycemic control in a manner independent of exercise or other activities central to yoga. Establishment of a standardized breathing pattern during GI calculation could be clinically important for improving the accuracy of GI measurements. Persons with type 2 diabetes or chronic obstructive pulmonary disease may also benefit from RB.
Footnotes
Acknowledgments
The authors would like to thank S. Covey, S. Murphy, C. Caldwell, R. Heimerman (WSU) for laboratory assistance, and the individuals who participated in the study. The authors would also like to acknowledge the WSU Foundation for funding support.
Disclosure Statement
No competing financial interests exist.